
A staged “fix followed by flap” strategy is a practical alternative for severe Gustilo Type IIIB/IIIC open fractures when early combined reconstruction is not feasible.
Dr. Tatsuhiko Muraoka, Department of Trauma Reconstruction Center, Yonemori Hospital, Kagoshima - 890-0062, Japan. E-mail: m03089tm@gmail.com
Introduction: Management of Gustilo Type IIIB and IIIC open fractures remains challenging, particularly with regard to the timing of definitive fixation and soft-tissue reconstruction. Although early combined orthoplastic management is widely recommended, it is not always feasible in patients with severe injuries, polytrauma, or complex fracture patterns.
Case Series: [1.1] We retrospectively reviewed 23 consecutive patients with Gustilo Type IIIB or IIIC open fractures treated at our institution between April 2022 and October 2024. Five patients underwent a single-stage “fix and flap” strategy, whereas 18 patients underwent a staged “fix followed by flap” strategy. Treatment selection was based on injury severity, fracture complexity, soft-tissue condition, and the overall physiological status of the patient. Clinical outcomes, including deep infection, non-union, malunion, and amputation, were assessed, together with treatment timing and operative duration.
Results: Patients treated with the staged strategy tended to have more severe overall injuries, with a higher mean injury severity score than those treated with the fix-and-flap strategy (13.8 ± 7.3 vs. 10.8 ± 4.0, P = 0.25). All patients requiring concurrent surgery for other anatomical sites were treated with the staged protocol. Deep infection occurred in two patients in each group. One patient in the staged group required additional surgery for an infected non-union. No cases of malunion or amputation were observed in either group. Importantly, no patients required additional flap procedures, indicating that adequate soft-tissue coverage was achieved in all cases. The interval from injury to osteosynthesis was similar between groups, whereas the interval to soft-tissue reconstruction was significantly longer in the staged group (9.2 ± 2.2 vs. 4.8 ± 0.8 days, P < 0.01). Operative time for osteosynthesis was also significantly longer in the staged group.
Conclusion: A staged “fix followed by flap” strategy appears to be a practical and clinically useful option for managing complex Gustilo Type IIIB and IIIC open fractures when early combined reconstruction is not achievable. This approach may allow more accurate planning of soft-tissue coverage in severe injuries.
Keywords: Gustilo Type IIIB, Gustilo Type IIIC, open fracture, staged reconstruction, fix followed by flap, fix and flap.
The Gustilo-Anderson classification is widely used in the evaluation of open fractures and remains an important predictor of complications such as deep infection, non-union, and amputation [1]. Among open fractures, Gustilo types IIIB and IIIC injuries represent the most severe forms and are associated with markedly increased complication rates compared with lower-grade injuries [2,3,4]. For this reason, these injuries require meticulous orthoplastic management to preserve limb function and reduce the risks of infection, non-union, and limb loss. Early soft-tissue coverage has been emphasised as a key principle in the management of severe open fractures [5,6]. Gopal et al. reported favourable results with the “fix and flap” strategy, in which definitive skeletal stabilisation and flap coverage are performed together within 72 h after injury [7]. This concept has influenced contemporary guidelines, including those recommending definitive soft-tissue coverage within 72 h or, at the latest, within 7 days [8,9,10,11]. Despite the theoretical advantages of early combined reconstruction, this approach is not always feasible in daily clinical practice. Patients with polytrauma, haemodynamic instability, extensive bone defects, or highly complex fracture patterns may require damage control procedures, prioritisation of other injuries, or prolonged time for definitive fixation. In such situations, staged reconstruction may provide a practical alternative. In our institution, when immediate combined fixation and coverage are difficult, definitive fracture stabilisation is performed first, followed by delayed soft-tissue reconstruction once the patient’s condition stabilises and the final extent of the soft-tissue defect becomes clear. During this interval, negative pressure wound therapy (NPWT) is used as temporary wound management [8,9]. The purpose of this study was to describe our institutional experience with two treatment strategies for Gustilo Type IIIB and IIIC open fractures: a single-stage “fix and flap” approach and a staged “fix followed by flap” approach. Rather than attempting to establish comparative effectiveness, we aimed to evaluate the clinical feasibility of staged reconstruction in severe and complex injuries.
Study design:
This study was designed as a retrospective descriptive case series.
Patients:
We retrospectively reviewed all consecutive patients with Gustilo Type IIIB or IIIC open fractures treated at our institution between April 2022 and October 2024. Patients were either admitted directly through our emergency department or referred from regional hospitals after initial debridement and provisional stabilisation. Patients were included if they were 16 years of age or older and underwent treatment using either a single-stage “fix and flap” strategy or a staged “fix followed by flap” strategy. Patients treated with skin grafts alone without flap reconstruction, patients transferred more than 1 week after injury, and patients with pre-existing infection at the time of transfer were excluded. Post-operative outcomes were evaluated in patients with a minimum follow-up of 12 months. No formal sample size calculation was performed because this study was a retrospective descriptive case series. All consecutive eligible patients treated during the study period were included.
Treatment strategy:
The choice of treatment strategy was determined according to injury severity, fracture complexity, soft-tissue condition, and the overall physiological status of the patient. In the fix-and-flap strategy, definitive osteosynthesis and soft-tissue reconstruction were performed on the same day. This strategy was selected when fracture fixation was technically straightforward, and the anticipated soft-tissue defect was not expected to change substantially after fixation. In the fix-followed-by-flap strategy, definitive fracture fixation was performed first, and soft-tissue reconstruction was performed at a later stage. This approach was preferentially used in patients with polytrauma, extensive bone defects, or comminuted or complex fractures or when the extent of soft-tissue coverage could be better determined after osteosynthesis. NPWT was used in both strategies before definitive soft-tissue coverage.
Data collection:
The following variables were collected: age, sex, body mass index (BMI), Gustilo classification, fracture site (upper or lower extremity), skin defect area, presence of fractures at other anatomical sites requiring surgery, American Society of Anaesthesiologists Physical Status (ASA-PS) classification, injury severity score (ISS), type of fixation (plate fixation, intramedullary nailing, or combination), and type of soft-tissue reconstruction (free flap or pedicled flap).
Outcomes:
Primary outcomes included deep infection, non-union, malunion, amputation, and the need for additional flap procedures. Secondary outcomes included time from injury to osteosynthesis, time from injury to soft-tissue reconstruction, operative time for osteosynthesis, operative time for soft-tissue reconstruction, and interval from osteosynthesis to soft-tissue reconstruction in the staged group.
Statistical analysis:
Comparative analysis between the two groups was performed using Student’s t-test for continuous variables and Fisher’s exact test for categorical variables. A P < 0.05 was considered statistically significant. All analyses were conducted using EZR statistical software.
Ethics approval:
This study was conducted in accordance with the Declaration of Helsinki. The Institutional Bioethics Committee of Yonemori Hospital approved the study (Approval No. YR2405, approved on August 5, 2025) and waived the requirement for informed consent because of the retrospective design. Given the retrospective nature of the study, ethical approval was obtained after data collection had commenced.
A total of 23 patients were included in this study: 5 were treated with the fix-and-flap strategy and 18 with the staged fix-followed-by-flap strategy. There were no statistically significant differences between the two groups in age, sex, BMI, Gustilo classification, fracture site, skin defect area, ASA-PS, or the presence of fractures at other anatomical sites requiring surgery. However, patients in the staged group tended to have more severe overall injuries. The mean ISS was higher in the staged group than in the fix-and-flap group (13.8 ± 7.3 vs. 10.8 ± 4.0, P = 0.25) (Table 1).
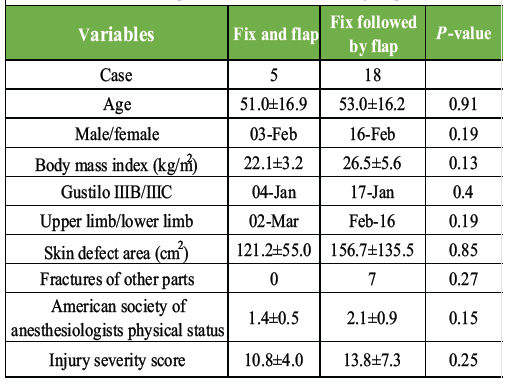
Table 1: Comparison of demographic information of the patients and details of open fracture between two groups
Regarding fixation methods, plate fixation was used in 19 cases, intramedullary nailing in 2, and a combination of plate fixation and intramedullary nailing in 2. For soft-tissue reconstruction, free flaps were used in 15 cases, while pedicled flaps were used in eight cases. In addition, all cases requiring concurrent surgery for other anatomical sites were managed using the staged protocol. Deep infection occurred in two patients in each group (P = 0.19). The causative organisms identified in these infected cases included methicillin-resistant Staphylococcus aureus and Enterobacter cloacae. One patient in the staged group developed an infected non-union and required additional surgical intervention. This patient was considered at particularly high risk because of severe contamination at the time of injury. No cases of malunion or amputation were observed in either group. Importantly, no patients required additional flap procedures after initial soft-tissue reconstruction, indicating that adequate coverage was achieved in all cases. No apparent differences in major complication rates were observed between the two groups (Table 2).
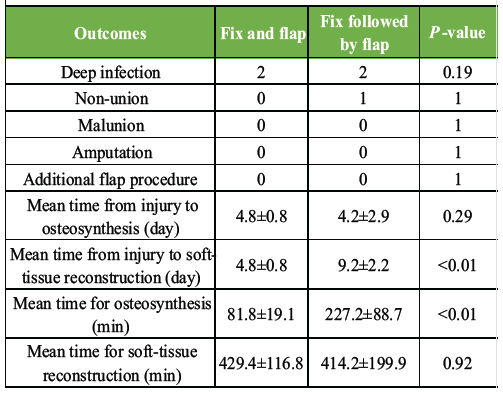
Table 2: Comparison of treatment outcomes between two groups
The mean interval from injury to osteosynthesis was 4.8 ± 0.8 days in the fix-and-flap group and 4.2 ± 2.9 days in the staged group (P = 0.29). The mean interval from injury to soft-tissue reconstruction was significantly shorter in the fix-and-flap group than in the staged group (4.8 ± 0.8 vs. 9.2 ± 2.2 days, P < 0.01). The mean operative time for osteosynthesis was significantly shorter in the fix-and-flap group than in the staged group (81.8 ± 19.1 vs. 227.2 ± 88.7 min, P < 0.01). In contrast, the mean operative time for soft-tissue reconstruction was similar between the two groups (429.4 ± 116.8 vs. 414.2 ± 199.9 min, P = 0.92). In the staged group, the mean interval between osteosynthesis and soft-tissue reconstruction was 5.0 ± 2.1 days. Additional procedures were performed as needed to achieve union. These included bone grafting using the Masquelet technique in selected cases.
A 59-year-old male sustained a work-related injury resulting in an open pilon fracture and a Lisfranc dislocation on the left side (Fig. 1).
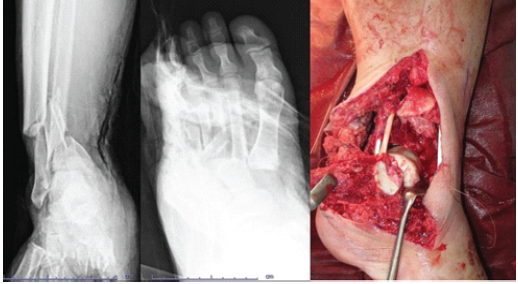
Figure 1: Pre-operative radiographs and clinical photographs of an open pilon fracture with Lisfranc dislocation.
Emergency stabilisation using external fixation and NPWT was performed on admission. The initial soft-tissue defect measured approximately 10 × 5 cm. On hospital day 2, second-look surgery and NPWT exchange were conducted. Internal fixation was performed on day 4, revealing an expanded soft-tissue defect of approximately 25 × 20 cm (Fig. 2). A free latissimus dorsi flap was applied on day 6 (Fig. 3).
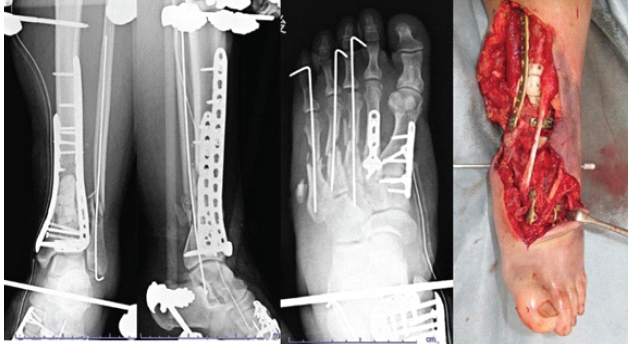
Figure 2: Post-operative images after internal fixation and wound size measurement.

Figure 3: Image of free latissimus dorsi flap reconstruction performed on hospital day 6.
Bone grafting using the Masquelet technique was done at 6 weeks. At 1-year follow-up, the patient had no complications and returned to work.
The present study describes our institutional experience in managing severe open fractures using two treatment strategies: single-stage fix and flap, and staged fix followed by a flap. The staged protocol was preferentially applied to patients with more severe injuries, including polytrauma, complex fracture patterns, and cases requiring prolonged operative time for definitive fixation. This tendency was supported by the higher ISS in the staged group, although not statistically significant. In addition, all patients requiring concurrent surgery for injuries at other anatomical sites were treated with the staged protocol, reflecting real-world clinical decision-making based on injury severity and patient condition. Early combined reconstruction is widely advocated to reduce complications in severe open fractures. The fix-and-flap strategy performed within 72 h has been shown to decrease infection and amputation rates [7], and current guidelines recommend early soft-tissue coverage within 72 h or up to 7 days [10,11]. However, this approach is not always feasible in patients with polytrauma, unstable physiology, or complex fractures requiring prolonged fixation. In such situations, a staged strategy may be more practical. Definitive skeletal stabilisation can be prioritised first, allowing more accurate assessment of soft-tissue defects and improved planning of reconstruction. An additional advantage of the staged “fix followed by flap” approach is the ability to determine the required soft-tissue coverage after osteosynthesis. As demonstrated in the presented case, the extent of the defect may change after fixation due to realignment and stabilisation. Simultaneous fixation and flap coverage may therefore result in inaccurate estimation of flap size and insufficient coverage. In contrast, the staged approach enables reconstruction after the final defect is clearly defined, allowing more reliable coverage. In this series, no cases required additional flap procedures, suggesting that adequate coverage was achieved. NPWT plays an important role in this staged approach by maintaining wound conditions during the interval before reconstruction and potentially contributing to infection control [8,9]. The staged strategy also offers practical advantages, including flexibility in surgical scheduling and improved coordination between orthopaedic and plastic surgery teams. Previous studies have reported favourable outcomes with staged orthoplastic management without increased complication rates [12,13]. Nevertheless, delayed reconstruction may increase the risk of wound complications. Prolonged intervals between fixation and flap coverage have been associated with higher infection rates [13,14,15]. In this study, the interval in the staged group exceeded recommended timeframes in some cases, indicating an area for potential improvement. Although no clear increase in major complications was observed, minimising delay remains important. This study has several limitations, including its retrospective design, small sample size, and heterogeneity of injury patterns. Treatment selection was based on clinical judgement, and the staged group included more severely injured patients. Therefore, these findings should not be interpreted as demonstrating comparative effectiveness, but rather as supporting the clinical feasibility of staged reconstruction. Accordingly, this study should be interpreted as a descriptive case series reflecting real-world clinical practice, rather than as a comparative effectiveness analysis. Importantly, this study reflects real-world trauma care, where ideal timing is not always achievable. In such settings, a staged fix-followed-by-flap approach may represent a practical and adaptable option for managing complex open fractures.
A staged “fix followed by flap” strategy appears to be a feasible and practical option for the management of complex Gustilo Type IIIB and IIIC open fractures. Although soft-tissue reconstruction is delayed, major complications such as deep infection, non-union, and amputation were not increased in this descriptive series. Importantly, no patients required additional flap procedures, suggesting that adequate and reliable soft-tissue coverage can be achieved with this approach.
When early combined orthoplastic reconstruction is not feasible, a staged “fix followed by flap” strategy provides a practical alternative for managing Gustilo Type IIIB and IIIC open fractures. Definitive fixation first allows more accurate assessment of the soft-tissue defect and facilitates appropriate flap selection.
References
- 1. Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: A new classification of type III open fractures. J Trauma 1984;24:742-6. [Google Scholar] [PubMed]
- 2. Castillo IA, Heiner JA, Meremikwu RI, Kellam J, Warner SJ. Where are we in 2022? A summary of 11,000 open tibia fractures over 4 decades. J Orthop Trauma 2023;37:e326-34. [Google Scholar] [PubMed]
- 3. Khoury P, Hazra N, DeMartino A, Birungi-Huff K, Slobogean GP, O’Toole RV, et al. Is the orthopaedic trauma association-open fracture classification better than the gustilo-anderson classification at predicting fracture-related infections in the tibia? J Orthop Trauma 2024;38:655-60. [Google Scholar] [PubMed]
- 4. Turley L, Barry I, Sheehan E. Frequency of complications in intramedullary nailing of open tibial shaft fractures: A systematic review. EFORT Open Rev 2023;8:90-9. [Google Scholar] [PubMed]
- 5. British Orthopaedic Association Trauma Committee. British orthopaedic association standard for trauma (BOAST): Open fracture management. Injury 2020;51:174-7. [Google Scholar] [PubMed]
- 6. Aljawadi A, Islam A, Jahangir N, Niazi N, Elmajee M, Reid A, et al. One-stage combined “fix and flap” approach for complex open Gustilo-Anderson IIIB lower limbs fractures: A prospective review of 102 cases. Arch Orthop Trauma Surg 2022;142:425-34. [Google Scholar] [PubMed]
- 7. Gopal S, Majumder S, Batchelor AG, Knight SL, De Boer P, Smith RM. Fix and flap: The radical orthopaedic and plastic treatment of severe open fractures of the tibia. J Bone Joint Surg Br 2000;82:959-66. [Google Scholar] [PubMed]
- 8. Stannard JP, Singanamala N, Volgas DA. Fix and flap in the era of vacuum suction devices: What do we know in terms of evidence based medicine? Injury 2010;41:780-6. [Google Scholar] [PubMed]
- 9. Krticka M, Ira D, Nekuda V, Svancara J, Masek M. Effect of negative pressure wound therapy on infectious complications in grade III open fractures. Acta Chir Orthop Traumatol Cech 2016;83:117-22. [Google Scholar] [PubMed]
- 10. National Institute for Health and Care Excellence (NICE). Fractures (Complex): Assessment and Management. London: National Institute for Health and Care Excellence; 2016. p. 114-40. [Google Scholar] [PubMed]
- 11. Pincus D, Byrne JP, Nathens AB, Miller AN, Wolinsky PR, Wasserstein D, et al. Delay in flap coverage past 7 days increases complications for open tibia fractures: A cohort study of 140 North American trauma centers. J Orthop Trauma 2019;33:161-8. [Google Scholar] [PubMed]
- 12. Nishida M, Kamekura S, Nakada I, Kiriyama M, Maeda C, Ozone E, et al. Definitive internal fracture fixation followed by staged free flap coverage (“fix followed by flap” protocol) for open Gustilo type IIIB fractures. J Orthop Sci 2025;30:142-6. [Google Scholar] [PubMed]
- 13. Al-Hourani K, Foote CJ, Duckworth AD, White TO, Kelly MB, Tornetta P 3rd, et al. What is the safe window from definitive fixation to flap coverage in type 3B open tibia fractures? Supporting plastics and orthopaedics alliance in reducing trauma adverse events (SPARTA). J Orthop Trauma 2023;37:103-8. [Google Scholar] [PubMed]
- 14. Khouri RK. Avoiding free flap failure. Clin Plast Surg 1992;19:773-81. [Google Scholar] [PubMed]
- 15. Kuripla C, Tornetta P 3rd, Foote CJ, Koh J, Sems A, Shamaa T, et al. Timing of flap coverage with respect to definitive fixation in open tibia fractures. J Orthop Trauma 2021;35:430-6. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial
January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre
November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre January 1, 2025 Outcome of a Nail-plate Fixation Combination for a Distal Femur Fracture in a 99-year-old Patient
January 1, 2025 Outcome of a Nail-plate Fixation Combination for a Distal Femur Fracture in a 99-year-old Patient January 1, 2025 A Case Series on the Devastating Simultaneous Bilateral Fracture of Ankles That Remains Under-reported: Can We Address the Career-Ending Injuries?
January 1, 2025 A Case Series on the Devastating Simultaneous Bilateral Fracture of Ankles That Remains Under-reported: Can We Address the Career-Ending Injuries?