
[box type=”bio”] What to Learn from this Article?[/box]
Metacarpophalngeal dislocation needs high index of suspicion with prompt reduction and rehabilitation.
Case Report | Volume 6 | Issue 3 | JOCR July-Aug 2016 | Page 67-69 | Ahmed Naeem Atiyya, Ramy Ahmed Soliman. DOI: 10.13107/jocr.2250-0685.512
Authors: Ahmed Naeem Atiyya[1], Ramy Ahmed Soliman[1]
[1]Department of Orthopedic, Ain Shams University, Abbasia Square Cairo-Egypt.
Address of Correspondence
Dr. Ahmed Naeem Atiyya, MD
Associate Professor, Orthopedic Department
Faculty of Medicine, Ain Shams University
Abbasia Square. Cairo-Egypt.
E-mail: anatiyya@yahoo.com
Abstract
Introduction: Multiple simultaneous dislocations of the metacarpophalangeal joints are exceedingly rare. Five cases only were described in the English literature. Only one case necessitated open reduction. A case of simultaneous open and closed dislocation of ipsilateral four metacarpophalangeal joints is presented. The case had a delayed presentation (8 days following the trauma) and needed open reduction.
Case presentation: A 33-year-old manual worker sustained dislocation of the ulnar four metacarpophalangeal joints of his non dominant hand. The hand injury was missed for eight days. The injury was successfully managed by open reduction. The patient regained near normal functional outcome.
Conclusion: Open reduction may be needed for these injuries. Prompt intervention and early rehabilitation are needed for satisfactory outcome.
Key words: multiple MP dislocations, irreducible, volar approach.
Introduction
Metacarpophalangeal (MCP) joint dislocation is uncommon [1].However, injuries to the MCP joint have the potential to severely affect hand function[2]. The border digits (index and little fingers) are most frequently involved because of their increased vulnerability to trauma and lack of stabilization by two adjacent deep transverse metacarpal ligaments [3]. Multiple simultaneous dislocations of the MCP joints are exceedingly rare [2]. Five cases only were described in the English literature [4, 5, 6, 7]. Only one case necessitated open reduction. A case of simultaneous open and closed dislocation of ipsilateral four metacarpophalangeal joints is presented. The case needed open reduction.
Case Report
A 33-year-old manual worker male fell from a six-meter height on his outstretched left hand. He sustained subcapsular hematoma of the spleen which was treated conservatively based on an expectant management policy. The hand injury was missed from the start. All attention was directed toward the spleen injury. Upon discovery of the hand injury the patient was referred to our hospital eight days after the trauma. On examination, there was a wound on the volar aspect of the palm between the proximal and distal palmar creases with only the head of the fifth metacarpal was exposed. X-ray showed dorsal dislocation of the metacarpophalangeal joint of the index, long, ring and little fingers, in addition to old non united scaphoid waist fracture (Fig. 1).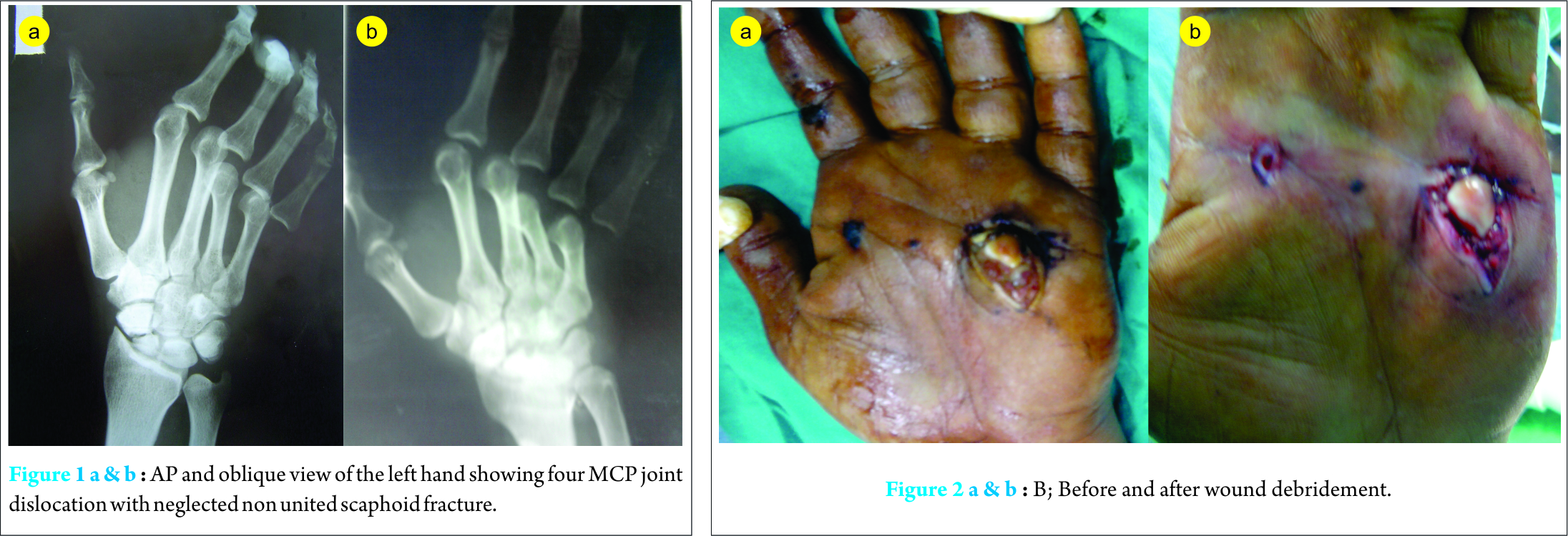
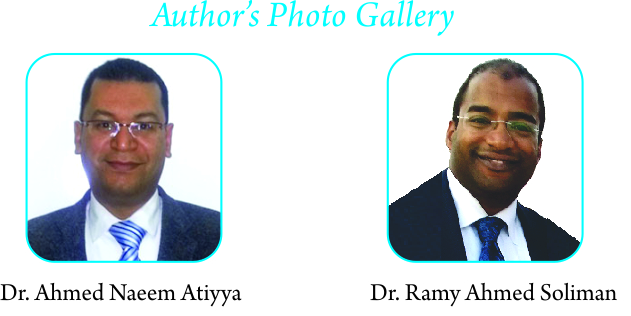
Under general anesthesia, trial of closed reduction of the open dislocation was attempted but failed. Decision was taken to proceed for open reduction using the volar approach. The wound was irrigated copiously with sterile saline, explored for foreign material (Fig. 2). Incision following the distal palmar and thenar creases was utilized. The incision at the palmar crease included the wound exposing the fifth metacarpal head (Fig. 3).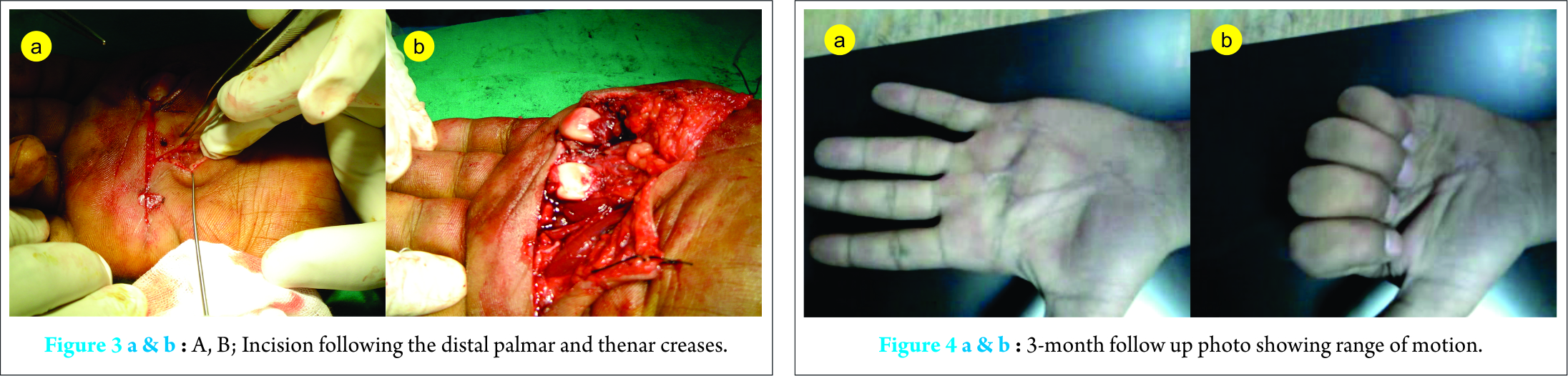
Starting with the little finger, the neurovascular bundles were dissected free and protected, followed by A1 pulley release to decrease the tension of the long flexors. Exposure of the joint revealed the volar plate which was intervening between the metacarpal heads and the base of the proximal phalanx. Reduction of the joint and repair of the volar plate was accomplished. Following reduction of the little and ring finger, the tension of the long flexors of the middle finger was partially relieved. Retraction was done easily with no need for pulley release. Reduction of the 2nd metacarpophalangeal joint occurred spontaneously following reduction of the middle finger MCP joint. A dorsal splint was applied to the patient. MCP joints were fixed at 45 degrees of flexion with full extension of proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints. Immobilization continued for two weeks, followed by progressive physiotherapy under supervision of a hand therapist. At three- month- follow up the patient regained near full range of motion (ROM) of the fingers (Fig. 4) with symmetrical grip strength to the healthy side.
Discussion
Ipsilateral four MCP joint dislocations are very rare. Reviewing the pertinent literature revealed five cases only described in English literature. Ramirez et al [4] reported a case of subluxation of the metacarpophalangeal joints of all four fingers. Three cases were open dislocations of the four metacarpophalangeal joints [5, 6, 7]. The last case was an open irreducible fracture/dislocation of the four ulnar metacarpals at the metacarpophalangeal joints [8]. Our case was different from previous cases regarding its delayed presentation (eight days following the trauma), and hence delayed intervention. This is in contrast to all four cases described in the literature which were managed promptly. Open reduction was needed only in this case in addition to one case of open irreducible fracture dislocation. In both cases, the volar plate was entrapped in the joint space. The remaining three cases were successfully reduced by closed manipulation. Dorsal MCP dislocations are divided into reducible and irreducible (also referred to as complex) dislocations with the volar plate is the primary structure preventing reduction of the dislocation [9]. Perhaps the biggest controversy in surgical management of the dislocation is the approach: whether volar or dorsal?[10] Although the open wound on the volar aspect of the head of the little finger’s metacarpus dictated utilizing the volar approach, it is advantageous to repair the volar plate and thus preventing any theoretical instability to ensue later on, to release the tension in the long flexors and thus facilitating the reduction, and finally to protect the neurovascular bundles rather than to avoid them. Before surgery a closed reduction to the little finger was attempted and the trial was rapidly aborted upon failure to reduce it. Delayed presentation of the patient in addition to the high possibility of irreducible dislocation were convincing for us to rapidly terminate the failed trial of closed reduction and to proceed directly to surgery. However, the ease of reduction of the middle finger with the following spontaneous reduction of the index finger, made us to think -retrospectively- that the dislocation of the MP joint of these two fingers was reducible from the start. It might be possible that if closed reduction was tried for these two fingers, it would have succeeded. It could be assumed that the loading force to the fingers was differential with the highest impact occurred on the little finger (open dislocation) and gradually decreased radial-ward. In contrast to what was done in this case, it may be prudent to try closed reduction for all fingers separately in cases with multiple MCP dislocation before judging the reduction as a whole as an irreducible.
Conclusion
Open reduction may be needed for multiple metacarpophalangeal joints dislocation. Closed reduction for each finger separately is better undertaken before judging the closed reduction trial as a whole as failed. Prompt intervention and early rehabilitation are needed for satisfactory outcome.
Clinical Message
Multiple metacarpophalangeal joints dislocations are exceedingly rare. Trial of closed reduction is needed for each finger. Open reduction will be the alternative should the closed reduction failed.
References
1. Dutton RO, Meals RA. Complex dorsal dislocation of the thumb metacarpophalangeal joint. Clin Orthop 1982;164:160–4.
2. Stowell JF, Rennie WP. Simultaneous open and closed dislocations of adjacent metacarpophalangeal joints: a case report. J Emerg Med 2002;23:355–8.
3. May Jr JW, Rochrich RJ, Sheppard J. Closed complex dorsal dislocation of the middle finger metacarpophalangeal joint: anatomic considerations and treatment. Plast Reconstr Surg 1988;82:690–3.
4. Ramirez RG, Combalía AA, Valer TA, Bordas SJL, Rofes CS. Simultaneous subluxation of the metacarpophalangeal joints of all four fingers: a case report. J Hand Surg 1985;10 A(1):78-80.
5. McCarthy LJ. Open metacarpophalangeal dislocations of the index, middle, ring and little fingers. J Trauma 1980;20:183-5.
6. Wright CS. Compound dislocations of four metacarpophalangeal joints. J Hand Surg 1985;10B:233-5.
7. Fraser KE, Stamer DT. Open dorsal dislocations of the index, long, ring, and small finger metacarpophalangeal joints. J Hand Surg 1995;20 A(4): 576-7.
8. Monteiro E, Negrão P, Vidinha V, Gutierres M, Pinto R. Open irreducible fracture/dislocation of the four ulnar metacarpals at the metacarpophalangeal joints: case report. Eur Orthop Traumatol. 2013; 4: 277–80.
9. Afifi AM, Medoro A, Salas C, MS, Taha MR, and Cheema T. A cadaver model that investigates irreducible metacarpophalangeal joint dislocation. J Hand Surg 2009; 34A:1506–11.
| How to Cite This Article: Atiyya AN, Soliman RA. Simultaneous open and Closed Dislocation of four Metacarpophalangeal Joints: A Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2016 July-Aug: 6(3):67-69. Available from: https://www.jocr.co.in/wp/2016/07/10/2250-0685-512-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2025 Management of a Rare Case of Complex and Irreducible Dislocation of the Metacarpophalangeal Joint in the Little Finger – A Case Report
June 1, 2025 Management of a Rare Case of Complex and Irreducible Dislocation of the Metacarpophalangeal Joint in the Little Finger – A Case Report August 10, 2023 Irreducible Dislocation of the Great Toe Interphalangeal Joint, Dorsal, and Plantar. Management and Long-term Evolution
August 10, 2023 Irreducible Dislocation of the Great Toe Interphalangeal Joint, Dorsal, and Plantar. Management and Long-term Evolution October 10, 2022 Volar Dislocation of Second Metacarpophalangeal Joint-open Reduction with Volar Approach – A rare Case Report
October 10, 2022 Volar Dislocation of Second Metacarpophalangeal Joint-open Reduction with Volar Approach – A rare Case Report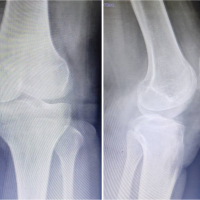 May 10, 2021 Neglected Locked Patellar Dislocation in an Adult Female: Report of a Rare Case
May 10, 2021 Neglected Locked Patellar Dislocation in an Adult Female: Report of a Rare Case