
[box type=”bio”] What to Learn from this Article?[/box]
Diagnosis of glomus tumor clinically sometimes doubtful but contrast enhanced M.R.I supported by clinical findings help us to reach the definate diagnosis of the condition.
Case Report | Volume 6 | Issue 3 | JOCR July-Aug 2016 | Page 38-39 | Dharam Singh, R S Garg, Vikas, Yashika Garg, Vijinder Arora. DOI: 10.13107/jocr.2250-0685.494
Authors: Dharam Singh[1], R S Garg[1], Vikas[1], Yashika Garg[2], Vijinder Arora[3]
[1]Department of Orthopaedics, Govt. Medical College, Amritsar. India.
[2]Department of Pharmacology, E.S.I Dental College, New delhi. India.
[3]Department of Radiology, S.G.R.D Medical college, Amritsar. India.
Address of Correspondence
Dr. Dharam Singh,
House no. 24/6, Yaseen Road, Amritsar Distt.[143001], Punjab. India.
E-mail: dharamsahota@rediffmail.com
Abstract
Introduction: Glomus tumor is a rare benign tumor arising from neuroarterial plexus concentrated beneath the nailbed usually in women of age group 20-40 yrs. The plexus is an arteriovenous anastomosis functioning without intermediary capillary bed, we report a case of glomus tumor affecting the nailbed of left little finger with characteristic periodic, spontaneous excruciating pain and temperature related algesia for the last 6 months. MRI helped in clinching the diagnosis at an early stage. Patient was operated for excision of the tumor making her completely pain free after resection of tumor.
Case Presentation: A 40-year-old female patient came in Ortho. OPD with complaints of pain, cold algesia, and point tenderness on the radial side of base of the nailbed of left little finger for the last 6 months. Diagnosis was delayed despite the patient having sought the advice from different clinicians a number of times before coming to us. Pain used to occur on accidental touching of tender spot, cold water immersion; excruciating at times, making the patient faint. On physical examination clinical diagnosis of glomus tumor was made, which was confirmed on MRI as the plain X-ray was noncontributory.
Conclusion: Most of the glomus tumors are benign, which are amenable to cure with complete surgical excision. Rarely, if the lesion exceeds 2 cm malignant transformation of the tumor must be suspected unless proven otherwise. Delay in clinical diagnosis due to dithering on the part of the clinician unnecessarily prolong the suffering in the patient which can be greatly helped by M.R.I in clinching the diagnosis early.
Key Words: Glomus body, sucquethoyer canals, M.R.I hand.
Introduction
The glomus tumor is a rare benign neoplasm that arises from the neuroarterial structure called a glomus body [7]. The glomus body is a specialized neuroarterial receptor composed of efferent arteriole, an anastmotic sucquethoyer canal, afferent venule. Hyperplasia of one or more parts of glomus body results into glomus tumor. This accounts for 1 % to 4.5 % of all tumors encountered in the hand. The normal glomus body is located in the stratum reticulare of the skin throughout the body, but is more concentrated in the digits. They are believed to help in thermal regulation. The glomus tumor usually affect a person of age between 30 to 50 years, although no age is exempt. It is relatively more common in females. The patient with glomus tumor seeks medical attention early, but the tumor itself is too small to be identified on physical examination. Although the classic triad of moderate to severe pain, temperature algesia, and point tenderness (loves pin test) are invariably present to help reach a definitive diagnosis, yet dithering on the part of treating clinician is the main cause of delay in treatment. But advent of MRI[10] and its interpretations will help tide over this problem as well. The tumor mass is usually less than 7 mm in dimensions, which can rarely be picked up on plain radiography as ‘bony erosion underneath the lesion” but can be picked up on MRI in every case [8, 9].
Histology- Glomus tumor is a well circumscribed mass consisting of small vessels surrounded by glomus cells (Fig. 1). Glomus cells have round to oval nuclei, pale eosinophilic cytoplasm and clearly defined cell margins. Mitotic figures and pleomorphism if present represents malignancy making it a malignant glomus tumor which is a rarer entity.
Case Report
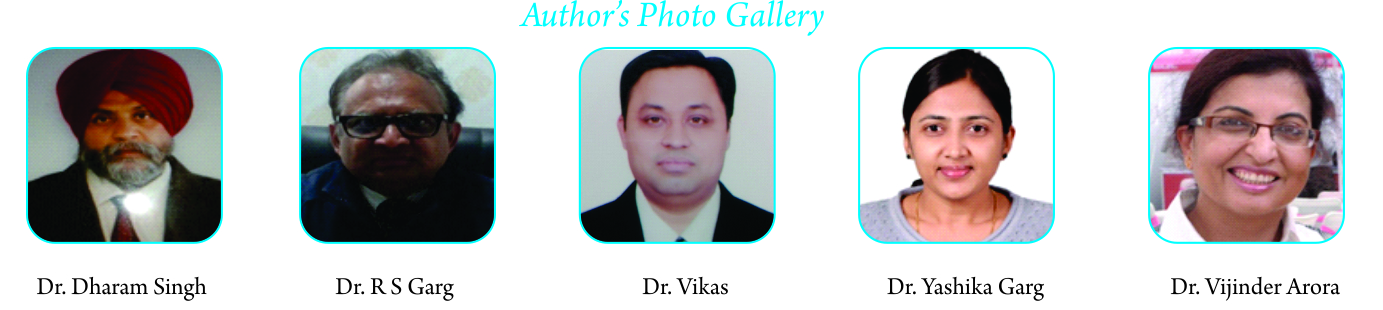
A 40-year-old female patient came in Ortho. OPD with complaints of pain, cold algesia, and point tenderness on the radial side of base of the nailbed [Fig. 2] of left little finger for the last 6 months. Diagnosis was delayed despite the patient having sought the advice from different clinicians a number of times before coming to us. Pain used to occur on accidental touching of tender spot, cold water immersion; excruciating at times, making the patient faint. On physical examination clinical diagnosis of glomus tumor was made, which was confirmed on MRI as the plain X-ray was noncontributory complete resection of tumor was done surgically [Fig. 3] under local anaesthesia and tourniquet control. Post-operative period was uneventful and stitches were removed on 12th day. Patient was fully relieved from her agonising pain [Fig. 4] to the extent that the patient repeatedly expressed her sincere gratitude to the treating surgeons. She lamented for having waited and suffered the agony for six months.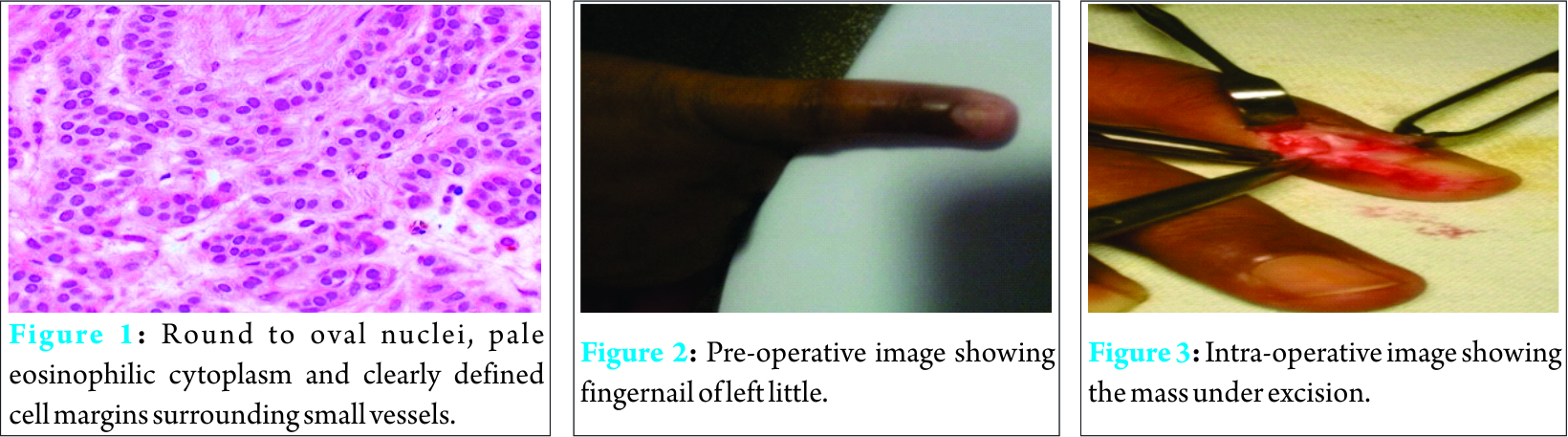
Discussion
Glomus tumor usually is a benign condition which responds favorably to a complete excision leading to cure, with low incidence of recurrence. Thorough interrogation, meticulous history taking and physical examination invariably clinch the diagnosis although MRI can be done to confirm the diagnosis. On MRI glomus tumor is a vascular entity, which is typically dark on T1 [Fig. 5] and bright on T2 weighted images. Post-gadolinium and fat saturation images further delineate [Fig. 6] the mass. Although this signal pattern can be present in any vascular tumor on MRI, the location of the tumor, its small size are salient features characteristics of the glomus tumor.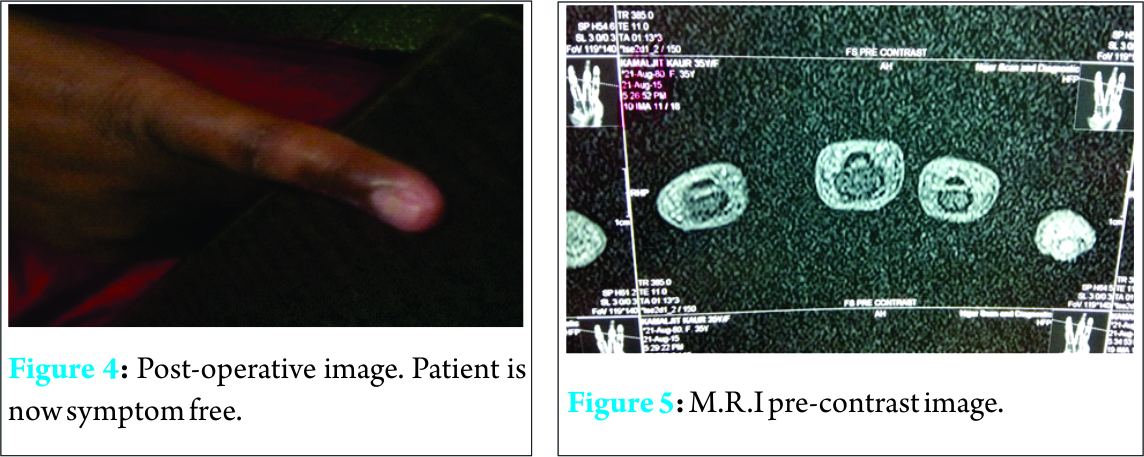
Conclusion
Most of the glomus tumors are benign, which are amenable to cure with complete surgical excision.Rarely, if the lesion exceeds 2 cm malignant transformation of the tumor must be suspected unless proven otherwise. Delay in clinical diagnosis due to dithering on the part of the clinician unnecessarily prolong the suffering in the patient which can be greatly helped by M.R.I in clinching the diagnosis early.
Clinical Message
On the face of strong clinical suspicion of glomus tumor with no radiological findings, M.R.I can help confirming the diagnosis and hence modality of choice in early diagnosis.
References
1. Kamarashev LE, French R, Dummer K. Symplasticglomus tumor – a rare but distinct begnin histological variant with analogy to other ancient begnin skin neoplasms. J CutanPathol. 2009;36:1099-1102.
2. Ponnelle T, Gounny P, Boudghène F, et al. [Glomus tumor of the extremities]. J Mal Vasc. 1999; 24(5):364-7
3. Wong CH, Chow L, Yen CH, Ho PC, Yip R, Hung LK. Uncommon hand tumors. Hand Surg. 2001;6:67-80.
4. Robbins SL, Cotran RS, Kumar V. Patologiaestrutural e functional. Vasossanguíneos. Rio de Janeiro: Guanabara; 1986. p. 522-3.
5. Pulitzer DR, Martin PC, Reed RJ. Epithelloidglomus tumor. Hum Pathol. 1995;26:1022-7.
6. Debol SM, Stanley MW, Mallery S, Sawinski E, Bardales RH. Glomus tumor of the stomach: cytologic diagnosis by endoscopic ultrasound-guided fineneedle aspiration. DiagnCytopathol. 2003;28:316-21.
7. Carroll RE, Berman AT. Glomus tumors of the hand. J Bone Joint Surg. 1972;54A(4):691–703.
8. Matloub HS, Muoneke VN, Prevel CD, Sanger JR, Yousif NJ. Glomus tumor imaging: use of MRI for localization of occult lesions. J Hand Surg. 1992;17A:472–275.
9. Mohler DG, Lim CK, Martin B. Glomus tumor of the plantar arch: A case report with magnetic resonance image findings. Foot & Ankle Int. 1997;18(10):672–674.
10. David H Kim. Glomus Tumor of the Finger Tip and MRI Appearance. Iowa Orthop J. 1999; 19:136-8.id H Kim. Glomus Tumor of the Finger Tip and MRI Appearance. Iowa Orthop J. 1999; 19:136-8.
| How to Cite This Article: Dharam Singh, R S Garg, Vikas, Yashika Garg, Vijinder Arora. Glomus Tumor – A Rarity; M.R.I- A big help in early Diagnosis. Journal of Orthopaedic Case Reports 2016 July-Aug;6(3):38-39. Available from: https://www.jocr.co.in/wp/2016/07/10/2250-0685-494-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


