
[box type=”bio”] What to Learn from this Article?[/box]
Sharp hardware should be removed as early as possible once the fracture undergoes union.
Case Report | Volume 6 | Issue 3 | JOCR July-Aug 2016 | Page 75-77 | Anoop Kalia, Kavin Khatri, Jagdeep Singh, Kapil Bansal, Mohammed Sagy, DOI: 10.13107/jocr.2250-0685.518
Authors: Anoop Kalia[1], Kavin Khatri[1], Jagdeep Singh[1], Kapil Bansal[1], Mohammed Sagy[1]
[1]Department of Orthopaedics, GGS Medical College Faridkot, Punjab. India.
Address of Correspondence
Dr. Jagdeep Singh,
Assistant Professor, Department of Orthopaedics, GGS Medical College, Faridkot , Punjab. India.
E-mail : jagatwal83@gmail.com
Abstract
Introduction: The migration of circlage wires used in tension band wiring construct of patella fractures in the posterior soft tissue envelope surrounding the knee joint has been rarely reported.
Case Presentation: A 60-year-old woman presented to us with pain over medial aspect of right knee joint. She underwent open reduction and internal fixation for a patellar fracture which she sustained 4 years back and subsequently underwent kirschner wire(k wire) removal for the same around 2 years back. X-rays of the knee joint shows that the circlage wire used in tension band construct which was left in place had broken into multiple pieces and was lying in the soft tissue envelope surrounding the knee joint and one piece migrate to the popliteal fossa. On examination patient did not had distal neuro- vascular deficit. The pain of the patient was due to the osteo-arthritic changes in her medial side of knee joint rather than broken wire pieces. Patient was advised to undergo total knee replacement along with subsequent removal of broken wires but patient refused for any type of surgery and is kept on regular follow up
Conclusion: This case report summarizes a rare complication resulting from hardware failure used for fixing patella fractures and throws a light on potential unwarned complications due to broken wires alongwith early recogonition and removal of broken hardware by surgeons.
Key Words: Circlage Wire, Popliteal Fossa, Osteoarthritis.
Introduction
Kirschner wires (k wires) and circlage wires are probably the most common implants used in orthopaedic surgery. Various complications can result from their breakage and migration. The patient may be asymptomatic or may be at fatal risk due to the migration upto as far as sternum and heart [1-7]. The nature of patient complaints must be analysed thoroughly through proper history taking before going for hardware removal in case of hardware failure. This case report present 60 year old female with broken circlage wire pieces in the soft tissues of the knee joint and emphasized that degenerative changes in the knee joint were the actual cause of patient’s pain rather than broken hardware.
Case Presentation
A 60-year-old woman presented to us with pain over medial aspect of right knee joint. The pain was non radiating. The pain was relieved by rest and was exacerbated by squatting and sitting cross legged. The patient had difficulty in climbing stairs. On physical examination there was tenderness along the medial aspect of knee joint and a curved scar mark was present over the anterior aspect of knee joint (Fig.1). While history taking the patient told us that she had a patella fracture around 4 years back which was treated by open reduction and internal fixation and she subsequently underwent implant removal 2 years back. The patient had full range of motion (ROM) at knee joint (Fig. 2, 3) and moderate pain was observed on medial side while flexing and extending knee joint. There was no history of any recent trauma to knee joint. A provisional diagnosis of osteoarthritis knee joint was made and weight bearing standing antero-posterior and lateral x-rays of left knee joint were ordered.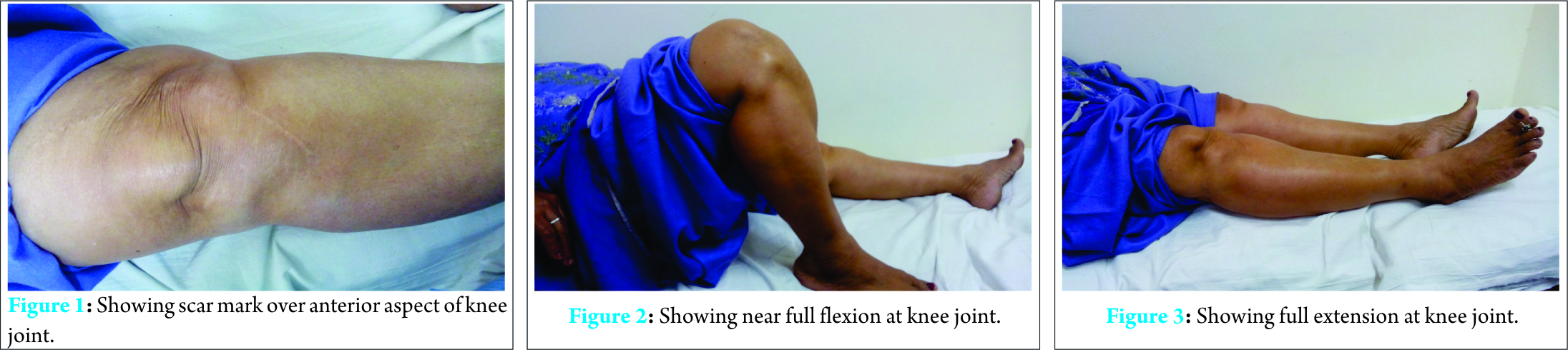
On X-rays it was found that multiple pieces of broken circlage wire were present around knee joint and one piece had migrated posteriorly (Fig. 4). On examination patient did not had distal neurovascular deficit and patients pain was not related to these broken pieces, rather it was due to degenerative changes in the knee joint. It is believed that the surgeon who did implant removal removed only the K wires leaving behind the circlage wires which broke into multiple pieces over the passage of time due to the repeated stresses at knee joint. Patient was advised to undergo total knee replacement along with subsequent removal of broken hardware as potential undue complications can occur because of broken hardware in the form of damage to neuro vascular structure due to migration of pieces posteriorly. It was also explained to the patient that cases have been reported where broken pieces migrate to heart and sternum and produce life threatening complications. However, patient refused to undergo any type of surgery. she was warned and told to be alert whenever the nature of her pain changes or she experiences new onset of symptoms which is different in character from the pain she is experiencing now and was kept on regular follow up.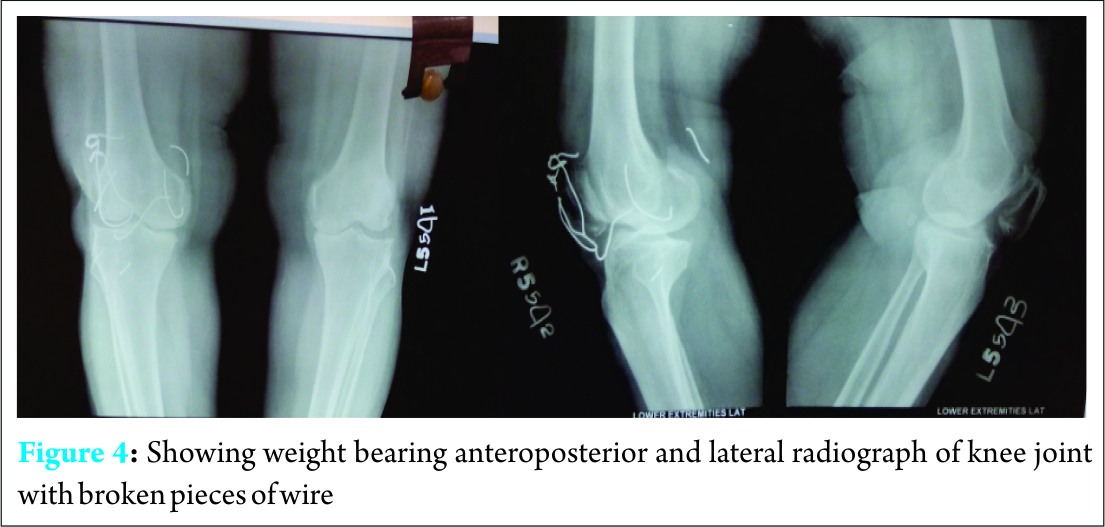
Discussion
K wires and circlage wires are probably the most common implants used in orthopaedic surgery. Breakage and migration of k wires is well established in literature. The migrated broken k wires and circlage wires can be benign with the patient completely symptom free or they can migrate to heart [1-7]. Migration of K wires to the heart have been reported from as close as sternum[2] as well as from as far as distal radius and finger[5, 6]. In our case the circlage wire which was left behind after removal of K wires broke into multiple pieces and one of the piece was lying posteriorly and was not the cause of patients pain which was rather due to osteoarthritic changes in her knee joint. After extensive search of literature it was found that only three such case reports describing four separate patients where broken wire was lying in the soft tissue envelope surrounding the posterior aspect of the knee joint have been reported[8-10]. Out of these four patients, in the three patients the broken implant was present in popliteal fossa and was causing pain [8, 9] .while in one patient the broken wire was lying in the posterior septum and not in the popliteal fossa and was removed arthroscopically [10]. Out of the two patients described in single case report [9], authors believed that in one of the patient, instead of single knot tensioning technique described by weber [11], two knot tensioning technique was used which could have possibly weakened the construct while in another patient too thin a wire was used which could have led to its breakage and migration into the popliteal fossa. In this case report also, use of too thin circlage wire might be the cuase of its breakage and eventually migration. In another reported case of K wire migration into popliteal fossa,the migrated wire was lying posterolaterally in the popliteal fossa, impinging upon the neurer ovascular structures. This was the cause of progressive anterior and postero-lateral pain in that case. The flexion of the knee joint was restricted to 30 degrees. Because of all these complaints the wire had to be removed surgically [10]. While reviewing the literature it was found that broken wires from patella besides lying in the soft tissue envelope around knee joint, have even migrated to the heart [12]. The patient in that case was put on cardiopulmonary by-pass and subsequently underwent right atriotomy to remove the broken piece. The authors after observing such a dreaded and near fatal complication recommended the removal of broken hardware in young active individuals due to the possible risk of migration. They proposed that if the broken hardware was lying around knee joint, Then Doppler ultrasound examination must be performed to rule out its proximity to neurovascular structures. The broken wires from patella can remain extra-articular in the soft tissue envelope around knee joint or can even migrate intra articular into the knee joint. Two such cases were found after extensive search of the literature [13, 14]. In one such case of intra articular wire migration, the patient had a badly comminuted patella fracture and underwent circumferential cerclage wiring. The circlage wire broke and migrated inside knee joint [13]. In another case, the patellar fracture went into non-union and the broken piece migrated inside the knee joint via a pseudo arthrosis line [14]. The patient in that case had a painful knee with intermittent locking symptoms. In our case broken pieces of circlage wire lying in soft tissue of knee joint with one piece migrate posteriorely to popliteal fossa however, patient pain was due to osteoarthritic changes rather than the broken pieces of wire. So she was kept on regular follow up as patient was not willing for any type of surgery. Therefore whenever the surgeon uses K wires or circlage wires he/she should keep all the complications in mind which can result from local as well as distant migration of broken wires. The wires may remain asymptomatic or they can migrate into joints causing damage to the cartilage or can impinge upon neurovascular structures causing pain or can injure neurovascular structures leading to life threatening haemorrhage or broken pieces can migrate via venous system travelling as far as upto heart leading to tamponade [15]. In order to avoid undue complications due to hardware failure, the surgeon must remove the sharp hardware like k wires and circlage wires after union of fracture patella.
Conclusion
This case report conclude that the presence of broken pieces of circlage wire in soft tissue envelope of knee joint is rare entity. This case report emphasized that the cause of the patients pain must be analyzed thoroughly before jumping to any conclusion. The operating surgeon must warn the patient about the possibility of hardware failure and breakage and the potential complications that could result and the patient should be kept under close observation and repeat radiographs at regular intervals must be performed. Even in asymptomatic patients once broken wires is recognized, it should be removed as early as possible.
Clinical Message
Sharp hardware should be removed as early as possible after bony union of fracture site.
References
1. Wirth MA, Lakoski SG, Rockwood CA Jr. Migration of broken cerclage wire from the shoulder girdle into the heart: A case report. J Shoulder Elbow Surg 2000;9:543-4.
2. Daus GP, Drez D Jr, Newton BB Jr, et al. Migration of a kirschner wire from the sternum to the right ventricle: a case report. Am J Sports Med 1993;21:321-2.
3. Medved I, Simic O, Bralic M, et al. Chronic heart perforation with 13.5 cm long kirschner wire without pericardial tamponade: an unusual sequela after shoulder fracture. Ann Thorac Surg 2006;81:1895-7.
4. Mellado JM, Calmet J, Garcia Forcada IL, et al. Early intrathoracic migration of kirschner wires used for percutaneous osteosynthesis of a two-part humeral neck fracture: a case report. Emerg Radiol 2004;11:49-52.
5. Seipel RC, Schmeling GJ, Daley RA. Migration of a k-wire from the distal radius to the heart.: A case report. Am J Orthop2001;30:147-51.
6. Haapaniemi TAT, Hermansson US. Cardiac arrhythmia caused by a kirschner wire inside the heart. An unusual complicationof finger osteosynthesis. J Hand Surg Br 1997;22:402-4.
7. Anic D, Brida V, Jelic I, et al. The cardiac migration of a kirschner wire. A case report. Tex Heart Inst J 1997;24:359-61.
8. Choi HR, Min KD, Choi SW, Lee BI. Migration to the popliteal fossa of broken wires from a fixed patellar fracture. Knee.2008;15:491-3.
9. Sanjay Meena, Hira Lal Nag, Senthil Kumar, Nilesh Barwar, Samarth Mittal, Amit Singla. Delayed migration of K-wire into popliteal fossa used for tension band wiring of patellar fracture. Chinese Journal of Traumatology 2013;16:186-188
10. Yasuaki Tamaki, Takashi Nakayama, Kenichiro Kita, Katsutosi Miyatake, Yoshiteru Kawasaki, Koji Fujii, and Yoshitsugu Takeda Arthroscopic Removal of a Wire Fragment from the Posterior Septum of the Knee following Tension Band Wiring of a Patellar Fracture. Case Reports in Orthopaedics Volume 2015 (2015), Article ID 827140, 5 pages.
11. Weber MJ, Janecki CJ, McLeod P, et al. Efficacy of variousf orms of fixation of transverse fractures of the patella. J Bone Joint Surg Am 1980;62: 215-20.
12. Biddau F, Fioriti M, Benelli G. Migration of a broken circlage wire from the patella into the heart. A case report . J Bone Joint Surg Am 2006;88:2057-9.
13. Chen YJ, Wu CC, Hsu RW, Shih CH. The intra-articular migrationof the broken wire: a rare complication of circumferential wiring in patellar fractures. Changgeng Yi Xue Za Zhi 1994;17:276-9.
14. Lushun WANG, Keng Thiam LEE. Locking knee after intra-articular migration of broken patella tension band wire: an extraordinary intra-articular migration via pseudarthrosis line. Acta Orthop Traumatol Turc 2013;47:444-447
15. Goodsett JR, Pahl AC, Glaspy JN, Schapira MM. Kirschner wire embolization to the heart:an unusual cause of pericardial tamponade. Chest.1999 Jan;115:291-3.
| How to Cite This Article: Anoop Kalia, Kavin Khatri, Jagdeep Singh, Kapil Bansal, Mohammed Sagy. Broken Pieces of Circlage Wire Lying in Soft Tissue Envelope Around Knee Joint: A Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2016 July-Aug;6(3):75-77. Available from: https://www.jocr.co.in/wp/2016/07/10/2250-0685-518-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 April 10, 2024 Case Report: Total Knee Arthroplasty in Ipsilateral Below-Knee Amputee
April 10, 2024 Case Report: Total Knee Arthroplasty in Ipsilateral Below-Knee Amputee June 10, 2022 Cutaneous Actinomycosis of Popliteal Fossa: A Rare Case Report
June 10, 2022 Cutaneous Actinomycosis of Popliteal Fossa: A Rare Case Report- December 10, 2020 Tibial Nerve Schwannoma: An Unexplained Cause of Lateral Foot Pain – A Rare Case Report and Review
 August 10, 2020 Primary Total Knee Replacement in a Case of Lateral Tibial Condyle Delayed Union with Severe Grade 4 Osteoarthritis Knee – A Case Report
August 10, 2020 Primary Total Knee Replacement in a Case of Lateral Tibial Condyle Delayed Union with Severe Grade 4 Osteoarthritis Knee – A Case Report