
[box type=”bio”] What to Learn from this Article?[/box]
Nicoll’s graft is ideal for gap non-union of bones like radius and ulna where defect is up to 3 cm.
Case Report | Volume 7 | Issue 2 | JOCR March – April 2017 | Page 17-20| Chaitanya Krishna, Jayanta Mondal, Anirudhha Sengupta. DOI: 10.13107/jocr.2250-0685.730
Authors: Chaitanya Krishna[1], Jayanta Mondal[1], Anirudhha Sengupta[1]
[1] Department of Orthopedics, Medical College and Hospital, College Street, Kolkata, West Bengal. India.
Address of Correspondence
Dr. Chaitanya Krishna,
Fellow in Joint Replacement and Reconstruction Centre, Sir Ganga Ram Hospital, New Delhi. India.
E-mail: chatconfident@gmail.com
Abstract
Introduction: Despite the multitude of studies for the treatment of non-unions, no clear criterion has been established for treating a fracture of non-union. Non-union of radius and ulna produces a discrepancy in length which must be restored for adequate rotation and function. Nicoll described a technique of bridging gaps in long bones with solid blocks of cancellous bone and fixing the fragments with metal plates. We utilized modified Nicoll’s graft using corticocancellous graft taken from iliac crest.
Case Report: In the present case, a 17-year-old male patient of eastern India presented with gap non-union of 3 cm in ulna of non-dominant hand, left side after 3 years and 6 months of trauma. There was linear surgical scar mark of 8 cm overlying ulna, but there was no sign of infection. He was functionally crippled with severe restriction of range of motion.
Conclusion: The tricortical cancellous bone graft under optimal compression provides a good solution for the management of gap non-union of both bone forearm for deficit up to 3 cm with no evidence of infection.
Keywords: Both bone, gap non-union, Nicoll’s graft, ulna.
Introduction
Orthopedic surgeons can choose from numerous surgical and nonsurgical methods that vary greatly in their invasiveness and propensity for minor and catastrophic complications in the treatment of gap non-union. In a situation with equal risks and benefits, the simplest, most easily tolerated method should be chosen. For many years, the most frequently used method of treatment of non-unions has been bone grafting. Autogenous cancellous bone, although limited in quantity and associated with significant donor site morbidity, remains the “gold standard” in grafting material. Various treatment modalities described in treating forearm bone loss include using boiled cadaveric bones [1], use of cortical tibial graft with screws [2], grafts using ulnar segment held by screws [3], use of iliac crest graft to fill the bone gap and fixation with an intramedullary nail [4], cancellous insert grafts with plate fixation [5, 6], bone transport in forearm bones using the principles of ilizarov [7], using fibula as an intercalary bone graft and with a tibial cortical bone graft fixed opposite to a plate [5, 8], and vascularized fibular iliac bone graft [9]. In 1956, Nicoll [5] described a method of overcoming this problem by filling the defect left by excision of dead bone with cancellous bone from the anterior iliac crest, securing the graft by a plate and screws. In 1980, grace and Evers modified Nicoll’s technique using a corticocancellous graft, fixed by a plate. The present paper discusses results of gap non-union of ulna treated by tricortico-cancellous bone graft with plate fixation.
Case Report
A 17-year-old male patient came to us with severe restriction of movement of left elbow joint and inability to do his daily activities. On examination, linear surgical scar mark was present over the left forearm on dorsal aspect; there was no sign of infection. The range of motion was 70-90° with restricted supination and pronation. On palpation, the metal plate was palpated over dorsal ulna. X-ray showed distinct gap non-union of ulna. There was no distal neurovascular deficit.
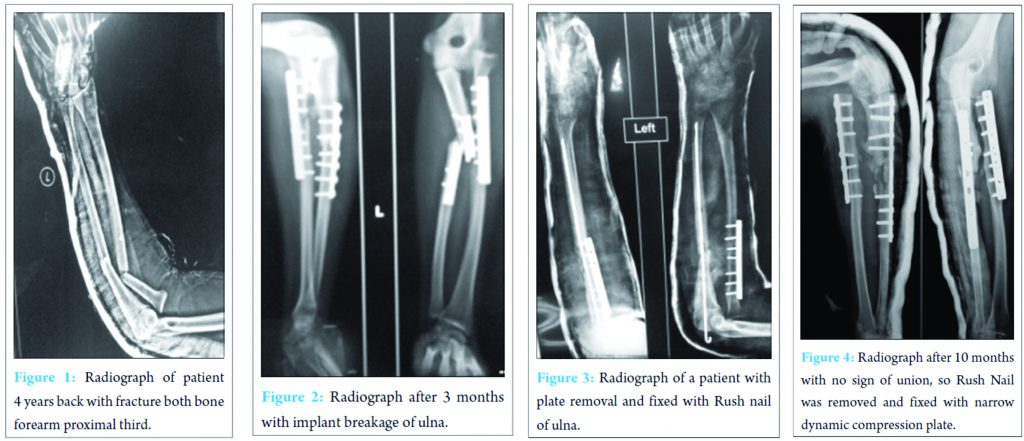
The patient had a history of road traffic accident 4 years back with fracture of both bone forearm proximal third (Monteggia variant) (Fig. 1). This fracture was internally fixed with narrow dynamic compression plate (DCP), but after 3 months implant breakage occurred of ulna (Fig. 2).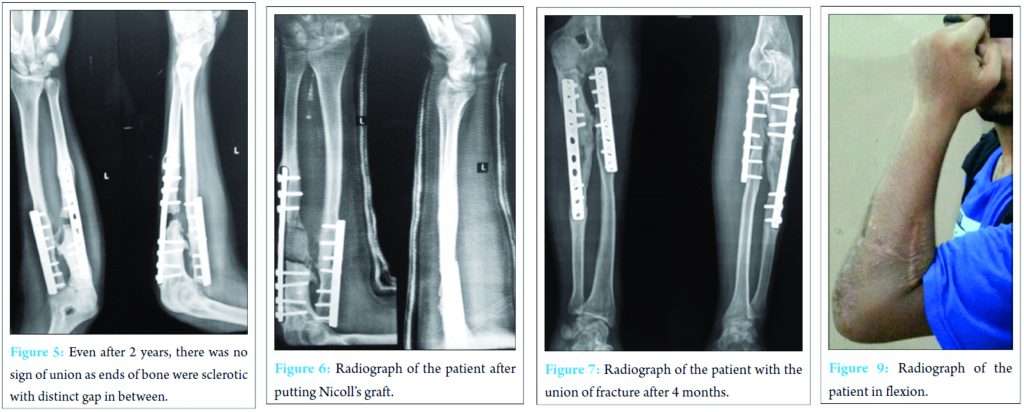 Then, plate was removed and fixed with Rush nail (Fig. 3). After 10 months, there was no sign of union, so rush nail was removed and fixed with narrow DCP (Fig. 4). Even after 2 years, there was no sign of union as ends of bone were sclerotic with a distinct gap in between (Fig. 5). Hence, we decided to go for modified Nicoll’s graft. We put a corticocancellous strut graft taken from anterior iliac crest and put it at the gap site after freshening the ends and under compression with arthrolysis of the joint (Fig. 6). After 4 months, there was a union at fracture site with 20-120° range of movement and 50° supination and 40° pronation (Fig. 7). The patient now can do his daily activity and is very much satisfied (Fig. 8 and 9).
Then, plate was removed and fixed with Rush nail (Fig. 3). After 10 months, there was no sign of union, so rush nail was removed and fixed with narrow DCP (Fig. 4). Even after 2 years, there was no sign of union as ends of bone were sclerotic with a distinct gap in between (Fig. 5). Hence, we decided to go for modified Nicoll’s graft. We put a corticocancellous strut graft taken from anterior iliac crest and put it at the gap site after freshening the ends and under compression with arthrolysis of the joint (Fig. 6). After 4 months, there was a union at fracture site with 20-120° range of movement and 50° supination and 40° pronation (Fig. 7). The patient now can do his daily activity and is very much satisfied (Fig. 8 and 9).
Discussion
A gap non-union is often characterized by significant scarring, sclerosis, and absorption of bone at fracture ends, leading to devascularization and lack of osteogenic potential due to biological failure. There are numerous treatment modalities of non-unions, but there is a paucity of the literature toward the management of atrophic non-unions of forearm bones with gaps. Nicoll described a method to deal with the problem of gap non-union, by filling the defect left after the excision of the dead bone, with cancellous bone from the anterior iliac crest and fixing the graft by compression plate. There are very few published reports on Nicoll’s technique. This simple technique has not gained it is popularity and is not being practiced by many as a standard orthopedic procedure for the management of gap non-unions of single or both bones of the forearm. The present study was undertaken to treat non-unions with a gap in forearm bones by modified Nicoll’s technique. The clinical and experimental evidence has proved that a fresh autogenous cancellous bone graft is always better than any other modality of treatment. For physical reasons, corticocancellous graft gives a more rapid union and less fibroblastic reactions than chips or slices [5, 10]. The sclerotic ends of bone are devoid of blood supply and lose the osteogenic potential. Siffert [11] regarded the freshened bone ends as the most important single source of osteogenesis. This technique of grafting is simple and provides stability to fracture as well as bone graft. The presence of cortical bones on three sides provides adequate strength with optimal compression at host-graft junction until the cancellous bone is involved in the formation of new bone due to creeping substitution and also allows for the early invasion of the periosteal circulation [12]. The abundance of the cancellous bone decreases the time of graft incorporation and filling up the gaps in the process of union. Thus, the procedure serves in three ways, i.e., internal fixation, defect bridging, and osteogenesis promoter.
Conclusion
The Nicoll’s bone graft which if modified with tricorticocancellous strut bone graft under optimal compression with the help of compression plate provides a high union rate for difficult problem of atrophic gap non-union of both bone forearms.
Clinical Message
Gap non-union can be challenging to treat. Many options are available with their own complications and prognosis. Nicoll’s graft provides an excellent option with minimal intervention and early union. With almost 3 cm of gap non-union, this case report provides an excellent example of the use of Nicoll’s graft.
References
1. Lloyd-Roberts GC. Experiences with boilded cadaveric bone. J Bone Joint Surg Br 1952;34-B(3):428-432.
2. Boyd HB. The Treatment of difficult and unusal non-union. J Bone Joint Surg 1943;25:535
3. Miller RC, Phalen GS. The repair of defects of the radius with fibular bone grafts. J Bone Joint Surg Am 1947;29(3):629-636.
4. Spira E. Bridging of bone defects in the forearm with iliac graft combined with intramedullary nailing. J Bone Joint Surg Br 1954;36-B(4):642-646.
5. Nicoll EA. The treatment of gaps in long bones by cancellous insert grafts. J Bone Joint Surg Br 1956;38-B(1):70-82.
6. Dabezies EJ, Stewart WE, Goodman FG, Deffer PA. Management of segmental defects of the radius and ulna. J Trauma 1971;11(9):778-788.
7. Tetsworth K, Krome J, Paley D. Lengthening and deformity correction of the upper extremity by the Ilizarov technique. Orthop Clin North Am 1991;22(4):689-713.
8. Moroni A, Rollo G, Guzzardella M, Zinghi G. Surgical treatment of isolated forearm non-union with segmental bone loss. Injury 1997;28(8):497-504.
9. Jupiter JB, Gerhard HJ, Guerrero J, Nunley JA, Levin LS. Treatment of segmental defects of the radius with use of the vascularized osteoseptocutaneous fibular autogenous graft. J Bone Joint Surg Am 1997;79(4):542-550.
10. Abbott LC, Schottstaedt ER, Saunders JB, De CM, Bost FC. The evaluation of cortical and cancellous bone as grafting material; A clinical and experimental study. J Bone Joint Surg Am 1947;29(2):381-414.
11. Siffert RS. Experimental bone transplants. J Bone Joint Surg Am 1955;37-A(4):742-758.
12. Gomez EA. Treatment of forearm non union with iliac graft and a Hunec nail. Acta Ortop Maxicana 2005;19:S28-S33.
 |
 |
 |
| Dr. Chaitanya Krishna | Dr. Jayanta Mondal | Dr. Anirudhha Sengupta |
| How to Cite This Article: Krishna C, Mondal J, Sengupta A. Modified Nicoll’s Graft for Treatment of Gap Non-union of Ulna: A Rare Case Report. Journal of Orthopaedic Case Reports 2017 Mar-Apr;7(2):17-20 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2024 Alternative Management Approach for Infected Gap Non-Union of Both Bone Forearms – A Case Report
December 1, 2024 Alternative Management Approach for Infected Gap Non-Union of Both Bone Forearms – A Case Report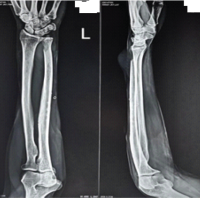 December 1, 2024 Primary Leiomyosarcoma of the Distal Ulna: A Case Report
December 1, 2024 Primary Leiomyosarcoma of the Distal Ulna: A Case Report October 1, 2024 Non-union Patella Fracture – Extensor Mechanism Repair with Quadriceps Release: A Case Report
October 1, 2024 Non-union Patella Fracture – Extensor Mechanism Repair with Quadriceps Release: A Case Report August 6, 2024 Management of Infected Gap Non-union of Distal Femur with Induced Membrane Technique using Limb Reconstruction System Followed by Augmentation Plating and Bone Grafting: A Case Report
August 6, 2024 Management of Infected Gap Non-union of Distal Femur with Induced Membrane Technique using Limb Reconstruction System Followed by Augmentation Plating and Bone Grafting: A Case Report