
[box type=”bio”] What to Learn from this Article?[/box]
How to manage large traumatic bone loss in the femur.
Case Report | Volume 7 | Issue 5 | JOCR Sep – Oct 2017 | Page 50-23| Stephen R Rossman, M Kareem Shaath, Kenneth W Graf. DOI: 10.13107/jocr.2250-0685.892
Authors: Stephen R Rossman[1], M Kareem Shaath[1], Kenneth W Graf[2]
[1]Department of Orthopaedic Surgery, Rutgers-New Jersey Medical School,140 Bergen Street ACC D-1610, Newark, New Jersey 07103, USA, [2]Department of Orthopaedic Surgery, Cooper University Health Care, Three Cooper Plaza Suite 403, Camden, New Jersey 08103, USA.
Address of Correspondence
Dr. Stephen R Rossman, Adult Reconstructive Surgery, Rutgers-New Jersey Medical School, 140 Bergen Street ACC D-1610,Newark, New Jersey 07103, USA.
E-mail: stephen.rossman@rutgers.edu
Abstract
Introduction: Open femoral fractures are relatively uncommon occurrences, with few reports addressing their management. They are caused by high-energy mechanisms, and bone loss is a possible, but infrequent occurrence. We present a case in which two friends, 20- and 21-year-old males, were involved in a motorcycle collision. A large piece of bone was ejected from one patient’s femur as a bony projectile and impaled the other patient’s tibia, resulting in an open tibial plateau fracture. To the best of our knowledge, this is the first case in the English literature to report a case in which a piece of bone was ejected from one patient, causing a fracture in another.
Case Report: Two males, in their mid-twenties, were involved in a head-on motorcycle collision. Both patients sustained open fractures to their lower extremities. A large piece of bone was ejected from one patient’s femur and impaled the other patient’s tibia, causing an open tibial plateau fracture. The patient who provided the bony projectile underwent retrograde intramedullary nail fixation. The segmental piece of bone was not replanted, and he went on to heal without negative sequelae at 2-year follow-up.
Conclusion: To the best of our knowledge, this is the first case documented in the English literature in which an ejected piece of bone from one person caused a fracture in another fracture. Management of extruded bone segments should be considered on a case-by-case basis.
Keywords: Bone extrusion, bone impalement, bone loss, open fracture, reimplantation.
Introduction
Open femoral fractures are relatively uncommon occurrences, with few reports addressing their management [1, 2, 3, 4, 5, 6, 7, 8]. They are caused by high-energy mechanismsand bone loss is a possible, but infrequent occurrence [4]. The bone loss may occur at the time of injury or as a part of surgicaldebridement. We present a case in which two friends, 20 and 21-year-old males, were involved in a motorcycle collision. A large piece of bone was ejected from one patient’s femur as a bony projectile and impaled the other patient’s tibia, resulting in an open tibial plateau fracture.
Case Report
Two patients, aged 21, (Patient A)and 20, (Patient B), were involved in a head-on motorcycle collision. They were transportedthroughhelicopter to the trauma department at our level-1 trauma center. On initial evaluation, patient A was awake, alert, and oriented with an obvious deformity to his left lower extremity with a large wound, measuring 10cm, over the anterior aspect of the knee with exposed bone (Fig. 1). He was neurovascularly intact with an ankle-brachial index of 1.0.On radiographic examination, the patient was found to have a transverse distal-third femoral-shaft fracture and an open Type IIIA Schatzker VI tibial plateau fracture [9, 10, 11]. Due to the increased risk of vascular injury in patients sustaining ipsilateral femur and tibia fractures, the patient underwent a computed tomography (CT) angiogram, which revealed no abnormalities (Fig. 2). On closer investigation of the radiographs, theproximal tibia was found to be impaled by a large piece of cortical bone. The origin of this bone was initially unknown. The patient was given the appropriate intravenous antibiotics and a tetanus vaccine. His open wound was irrigated and placed in a long leg posterior splint.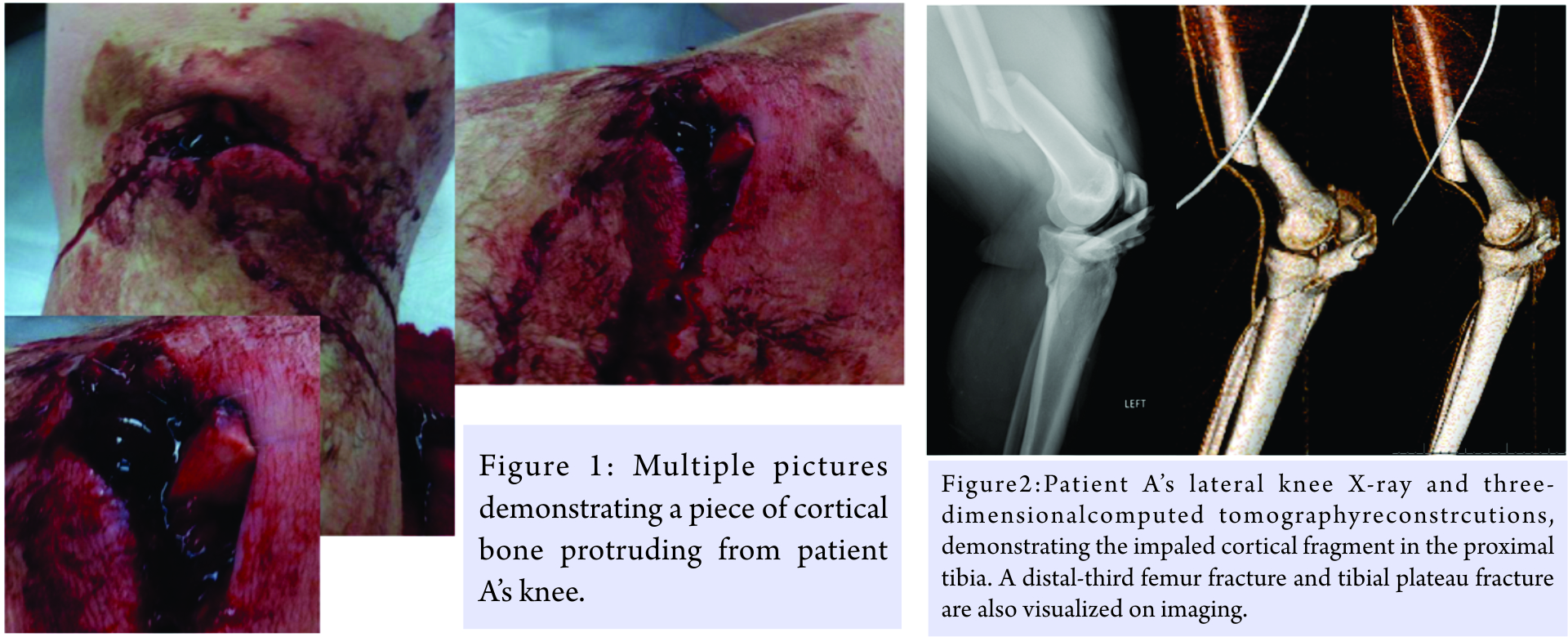
Attention was then turned to patient B. He was also awake and neurovascularlyintact. He was found to have a 6 cm wound to his left thigh. Radiographs and CT angiogram were performed, and the patient was found to have an open, comminuted, mid-shaft femur fracture with a missing piece of cortical bone and no vascular injury(Fig. 3). He was also found to have a fracture of the lateral pole of the patella as well as a coronal split of the lateral femoral condyleon the ipsilateral extremity. His wound was irrigated in the trauma bay, and he was placed in 20 pounds of proximal tibial skeletal traction. Post-traction radiographs further revealed cortical bone loss of the femoral shaft(Fig. 4).On further evaluation of both patients’ imaging studies, the missing cortical fragment from patient B’s femur was ejected and impaled patient A’s proximal tibia.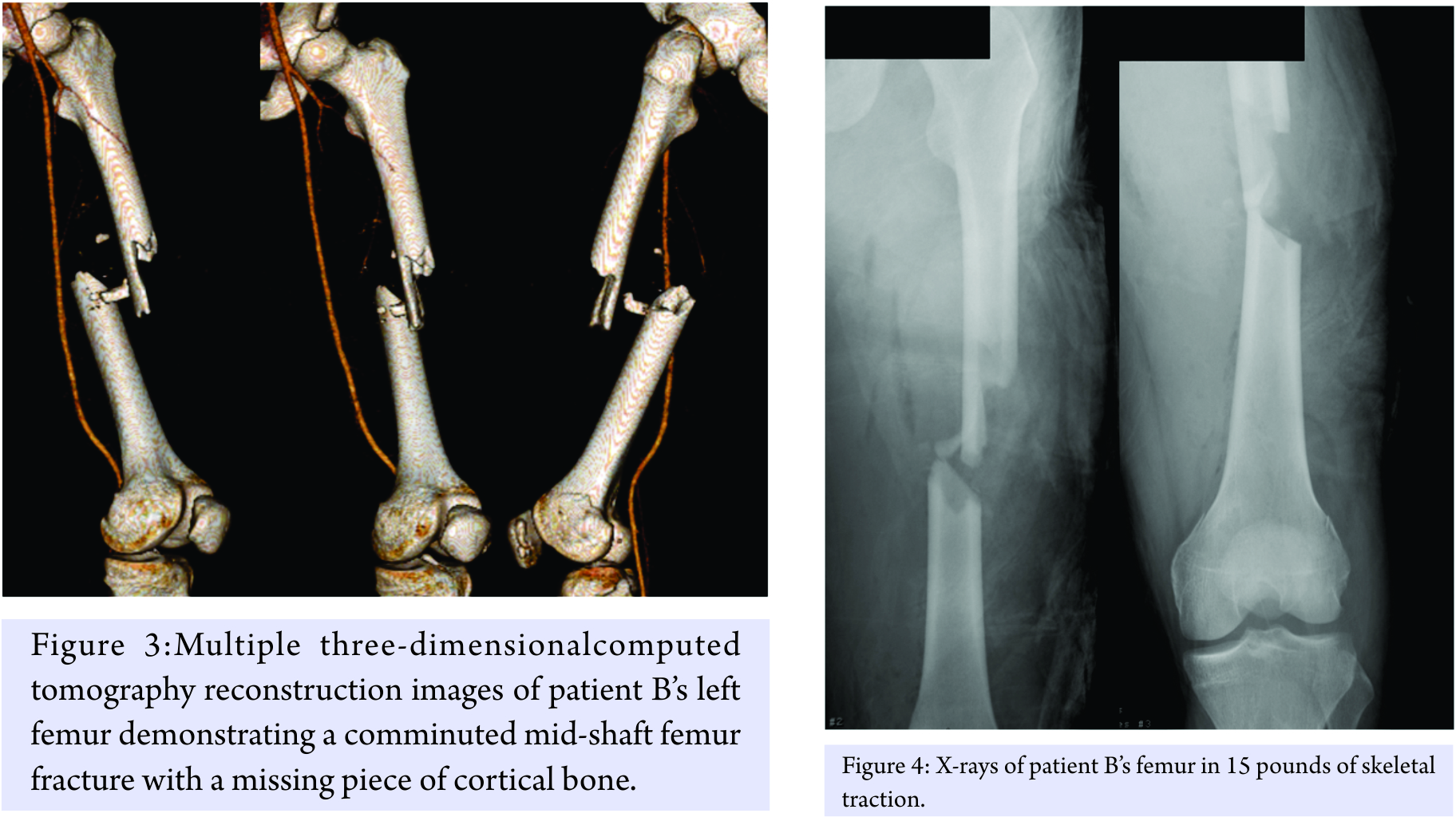
The decision was made to treat both patients operatively. First, patient A was taken to the operating room for an exploration and debridement of the left knee with there moval of the cortical piece of bone, followed by a retrograde intramedullary femoral nail. A spanning knee external fixator was placed to stabilize his tibial plateau fracture. The removed cortical fragment was identified as the missing piece of bone from the other patient’s femur (Fig. 5 and 6).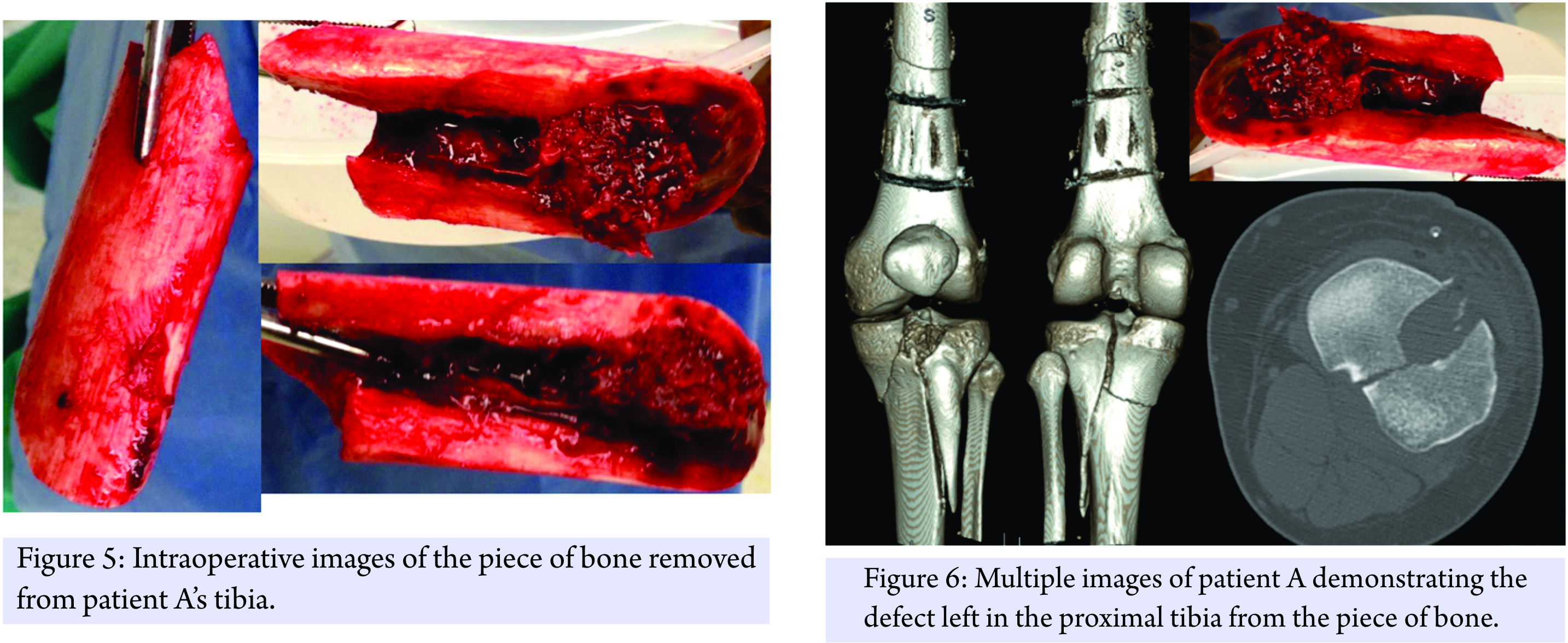
Patient B was then taken to the operating room for an irrigation and debridement of his left thigh and retrograde intramedullay nailing of his femur. The patella and femoral condyle fractures did not meet operative criteria. A long discussion was had with the patient and his family about how to best treat the bone loss from the femur. Due to the possibility of disease transmission, infection, and the fact that it was not involving the articular surface, the free piece of cortical bone was discarded. Since the patient was a young, healthy male with 50% apposition of intact femur, we decided to proceed with operative fixation of the femur without graft augmentation. A locked, retrograde femoral nail was used to stabilize the fracture (Fig. 7). Fig. 8 shows a side by side comparison of the extruded bone. He was made weight bearing as tolerated and was discharged home on post-operative day number 3.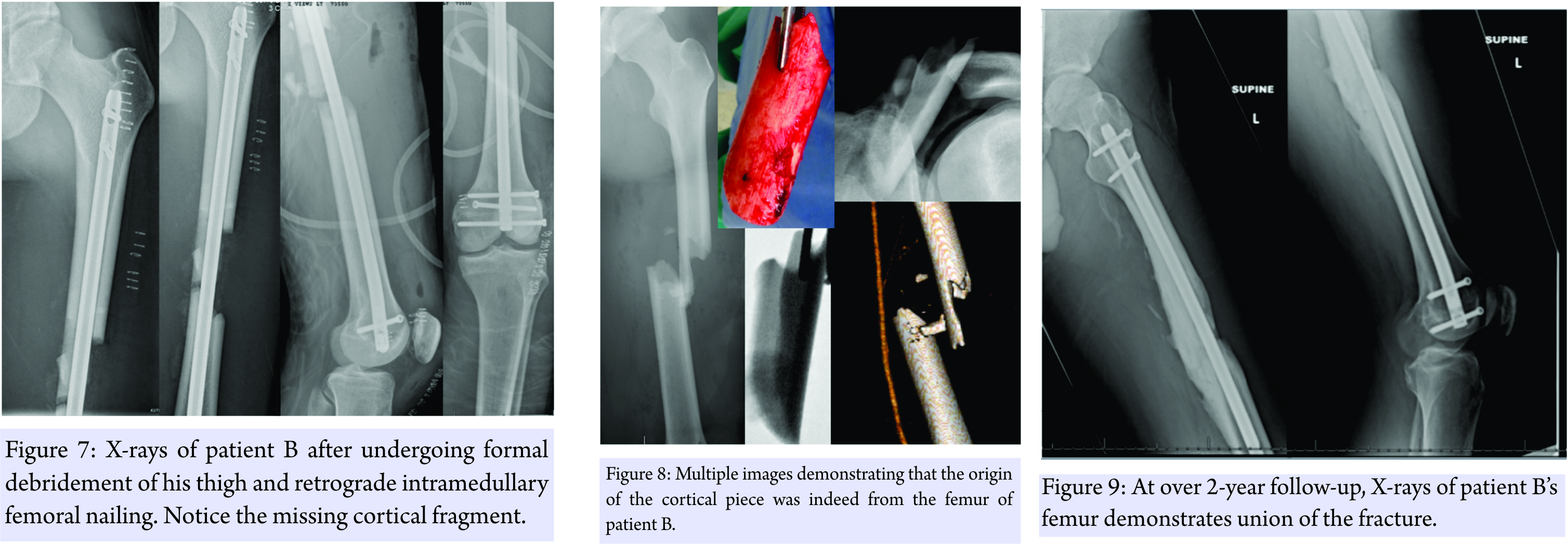
Patient A required an additional 8 days of soft tissue rest before definitive tibial fixation of his tibia. He was made non-weight bearing on his left lower extremity and was immediately started on a continuous passive motion machine for knee range of motion. He remained hospitalized for an additional week, pain control, and mobilization, before being discharged home.
At over 2-year follow-up, patient B had union of his fracture with no negative sequelae (Fig. 9). He was able to return to his profession full-time, as an electrician.
Discussion
Through an extensive search of the literature, this is the first case, to the best of our knowledge, in the English literature, in which apiece of bone was ejected from one patient, causing a fracture in another.
Treatment of bone loss following an open fracture can be a daunting task. Options include amputation, free fibula grafts, or bone transport [12].Multiple authors have described successful reimplantation of extruded bone fragments that were found in the field [13, 14]. This is not commonly performed, due to the high risk of infection, nonunion, and the need for subsequent procedures. Multiple methods of sterilization have been described [14,15, 16, 17]. Rouvillain et al. used an autoclave to sterilize an extruded 11 cm meta-diaphyseal femur fragment before reimplantation. They autoclaved the bone segment at 1218°C under 1.3 bars for 20 min [16]. Mazurek et al. successfully reimplanted an extruded 13 cm meta-diaphyseal femoral fragment in a 15-year-old boy after chemical sterilization with a solution made of 4% chlorhexidine for a total of 270 min [18]. Moosazadeh reimplanted an extruded 13.5 cm fragment of distal femur that was prepared by debridement, jet lavage irrigation with heated saline, and immersed in a solution of diluted gentamicin for 20 min [17].Finally, Aizah et al. used gamma sterilization before reimplanting an extruded 8 cm metaphyseal fragment of femur in a 14-year-old boy [15].
Mitchell et al. found that femoral shaft defects of <6 cm had a relatively a good prognosis with shorter mean times to union and no requirements for further procedures after primary intramedullary nailing. Fractures with diaphyseal defects of >6 cm were found to have a higher time to union and greater requirement for further procedures such as exchange nailing and bone grafting [4].
Along with contamination from the environment, a concern specific to this case was the potential for disease transmission between patients. Due to the rarity of this injury, the rate of disease transmission cannot be determined. The estimated risks of hepatitis C and HIV transmission from blood transfusions are 1 in 1.6 million and 1 in 1.8 million, respectively [16].The risk of disease transmission from bone allograft for hepatitis C and HIV is0.012% and 0.03%, respectively [19].
Conclusion
To the best of our knowledge, this is the first case documented in the English literature in which an ejected piece of bone from one person caused a fracture in another fracture. Management of extruded bone segments should be considered on a case-by-case basis. Bone loss <6cm of the femoral diaphysis can likely be treated successfully without any further bone graft or procedures. It is unknown what the risk of disease transmission would be in reimplanted bone. At current follow-up of over 2 years, both patients have fully recovered without any complications.
Clinical Message
We present a rare case where an ejected piece of bone from one patient caused a fracture in another.Specific concerns to this situation include therisk of disease transmission and management of bone loss in fracture care.Management of extruded bone segments should be considered on a case-by-case basis, and there is currently no consensus on how to manage these cases.
References
1. Williams MM, Askins V, Hinkes EW, Zych GA. Primary reamed intramedullary nailing of open femoral shaft fractures. Clin Orthop Relat Res 1995;318:182-90.
2. Rütter JE, de Vries LS, van der Werken C. Intramedullary nailing of open femoral shaft fractures. Injury 1994;25:419-22.
3. O’Brien PJ, Meek RN, Powell JN, Blachut PA. Primary intramedullary nailing of open femoral shaft fractures. J Trauma 1991;31:113-6.
4. Mitchell SE, Keating JF, Robinson CM. The treatment of open femoral fractures with bone loss. J Bone Joint Surg Br 2010;92:1678-84.
5. Lhowe DW, Hansen ST. Immediate nailing of open fractures of the femoral shaft. J Bone Joint Surg Am 1988;70:812-20.
6. Grosse A, Christie J, Taglang G, McQueen M. Open adult femoral shaft fracture treated by early intramedullary nailing. J Bone Joint Surg Br 1993;75:562-5.
7. Brumback RJ, Ellison PS Jr, Poka A, Lakatos R, Bathon GH, Burgess AR. Intramedullary nailing of open fractures of the femoral shaft. J Bone Joint Surg Am 1989;71:1324-31.
8. Baixauli F, Baixauli EJ, Sanchez-Alepuz E, Baixauli Jr F. FInterlocked intramedullary nailing for treatment of open femoral shaft fractures. Clin Orthop Relat Res1998;350:67-73.
9. Schatzker J, McBroom R, Bruce D. The tibial plateau fracture. The Toronto experience 1968–1975. Clin Orthop Relat Res 1979;138:94-104.
10. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: Retrospective and prospective analyses. J Bone Joint Surg Am 1976;58:453-8.
11. Paul GR, Sawka MW, Whitelaw GP. Fractures of the ipsilateral femur and tibia: Emphasis on intra-articular and soft tissue injury. J Orthop Trauma 1990;4:309-14.
12. DeCoster TA, Gehlert RJ, Mikola EA, Pirela-Cruz MA. Management of posttraumatic segmental bone defects. J Am Acad Orthop Surg 2004;12:28-38.
13. Shanmuganathan R, Agraharam D, Perumal R, Jayaramaraju D, Kulkarni S.Successful reimplantation of extruded long bone segments in open fractures of lower limb–a report of 3 cases. Injury 2015;46:1389-92.
14. Rouvillain JL, Navarre T, Noseda O, Garron E. Traumatic femoral bone defect reconstruction with an autoclaved autologous femoral segment. A 10-year follow-up. Acta Orthop Belg 2006;72:229-33.
15. Aizah N, Su Y, Shaifulnizam CW, Mros MA. Reimplantation of an extruded femoral segment after gamma sterilization in a Type IIIA Supracondylar femur fracture: A case report. Malays Orthop J 2014;8:66-8.
16. Busch MP, Kleinman SH, Nemo GJ. Current and emerging infectious risks of blood transfusions. JAMA 2003;289:959-62.
17. Moosazadeh K. Successful reimplantation of retrieved large segment of open femoral fracture: Case report. J Trauma 2002;53:133-8.
18. Mazurek MT, Pennington SE, Mills WJ. Successful reimplantation of a large segment of femoral shaft in a Type IIIA open femur fracture: A case report. J Orthop Trauma 2003;17:295-9.
19. Zou S, Dodd RY, Stramer SL, Strong DM. Probability of viremia with HBV, HCV, HIV, and HTLV among tissue donors in the United States. N Engl J Med 2004;351:751-9.
 |
 |
 |
| Dr. Stephen R Rossman |
Dr. M Kareem Shaath |
Dr. Kenneth W Graf |
| How to Cite This Article: Rossman SR, Shaath MK, Graf KW. Head-On Allograft Transplantation: A Unique Case Report Where a Large Piece of Femoral Bone was Extruded from One Patient’s Body and Impaled Another Patient’s Tibia. Journal of Orthopaedic Case Reports 2017 Sep-Oct;7(5):50-53 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Humerus Non-union with Segmental Bone Loss Treated with 3D-printed Prosthesis: A Case Report
February 1, 2026 Humerus Non-union with Segmental Bone Loss Treated with 3D-printed Prosthesis: A Case Report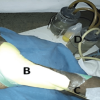 January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial
January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre
November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre January 1, 2025 Outcome of a Nail-plate Fixation Combination for a Distal Femur Fracture in a 99-year-old Patient
January 1, 2025 Outcome of a Nail-plate Fixation Combination for a Distal Femur Fracture in a 99-year-old Patient