
[box type=”bio”] Learning Point for the Article: [/box]
This report provides an insight into an atypical presentation of Giant cell tumours in a 15-year-old girl which otherwise usually occurs in the fourth decade of life.
Case Report | Volume 8 | Issue 3 | JOCR May – June 2018 | Page 10-13| Vijay C, Supreeth Nekkanti, RaviShankar R, ShashiKiran R, Sunila R. DOI: 10.13107/jocr.2250-0685.1086
Authors: Vijay C[1], Supreeth Nekkanti[1], RaviShankar R[1], ShashiKiran R[1], Sunila R[2]
[1]Department of Orthopaedics, JSS Medical College and Hospital, Mysore, Karnataka, India.
[2]Department of Pathology, JSS Medical College and Hospital, Mysore, Karnataka, India.
Address of Correspondence:
Dr. Supreeth Nekkanti,
No 160, 11thCross, 5th main, 1stStage, NGEF Layout,Nrupatunganagar, Nagarbhavi, Bengaluru-560072, Karnataka, India.
E-mail: drsupreethn@gmail.com
Abstract
Introduction: Giant cell tumors (GCTs) are locally aggressive tumors that principally affect the epiphysis of long bones. Histologically, these tumors consist of three types of cells: Osteoclast-like multinucleated giant cells, round mononuclear cells resembling mononucleocytes, and spindle-shaped round fibroblast-like stromal cells. Radiographically, the tumors appear osteolytic and radiolucent without a sclerotic border. The tumor rarely occurs in pediatric age group. Its incidence in pediatric patients varies from 1.8 to 7.5%.
Case Report: A 15-year-old girl presented to us with the complaints of pain in the left knee of 3months’ duration and inability to squat. Radiographic imaging was done which showed lytic lesion involving the proximal tibia and showing cortical destruction. The lesion was graded as a Campanacci Grade 3 tumor. The patient was taken up for surgery and an extended curettage was performed, and the cavity was packed with bone cement. The patient was asymptomatic at the end of 18-month follow-up and was continuing her normal daily activities.
Conclusion: GCT of the bone is extremely rare in skeletally immature patients. This particular case highlights the need for keeping the diagnosis of GCT at the periphery of one’s vision when dealing with pediatric patients presenting with osteolytic lesion at the epimetaphysis of long bones.
Keywords: Giant cell tumor, curettage, Campanacci grading, immature skeleton.
Introduction
Giant cell tumor (GCT) is a benign aggressive tumor usually affecting the ends of long bones. GCT accounts for 5% of all bone tumors and 20% of all benign tumors [1, 2, 3]. It is commonly understood by orthopedic surgeons to present in individuals in their third decade of life after closure of the physis [1]. We report our patient who was diagnosed with CGT at an unusual age of 15 years. The tumor rarely occurs in people aged below 18 years. Its incidence in pediatric patients has been reported to vary between 1.8 and 7.5% [4]. Curettage and wide resection are accepted methods of treatment of GCT of bone. The success rate with curettage in different reports varies widely.
Case Report
A 15-year-old girl presented to us with a dull pain in the left knee for 3 months and difficulty in squatting. On clinical examination of her left knee joint, there was no mass palpable. The terminal range of movement at the knee joint was restricted. There were no signs of inflammation. Laboratory investigations revealed C-reactive protein to be raised to 7.1 mg/dl, a normal alkaline phosphatase of 363U/L, and a raise derythrocyte sedimentation rate of 40. Radiographs of the knee joint showed an eccentric epiphyseal metaphysealosteolytic lesion of the left proximal tibia with anterolateralcortical breach. This lesion was graded as a Campanacci Grade 3 tumor (Fig. 1). Magnetic resonance imaging (MRI)showsa well-defined fairly homogenous hypointense lesion involving the proximal tibia with infiltration into surrounding soft tissue. Heterogeneously enhancing lesion with central non-enhancing hypointense areas was observed on T1W. A few central hyperintensities may represent cystic/hemorrhagic areas(Fig. 2).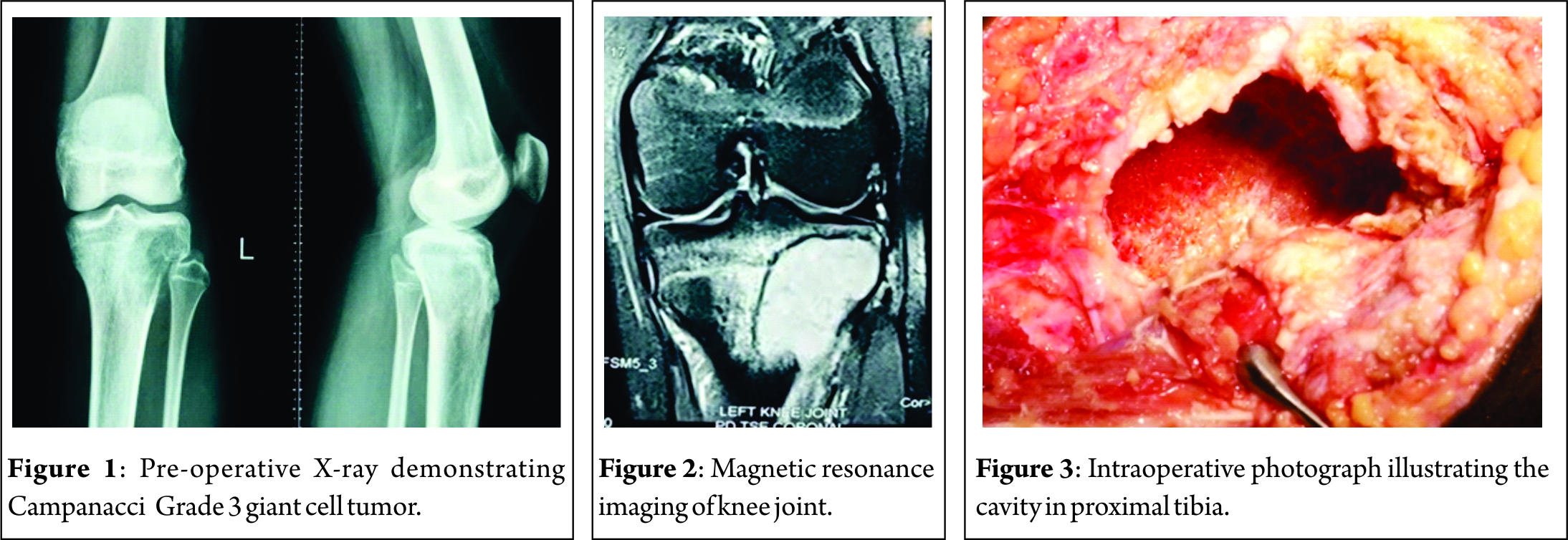
Surgical technique
An anterolateral approach to the proximal tibia was chosen for this patient keeping the possibility of knee joint involvement in mind. The iliotibial band was incised, and the proximal tibia explored to delineate the boundaries of the lesion. The lateral cortex of the proximal tibia was nibbled out to enter the cavity (Fig. 3). A thorough curettage was done using a bone gouge. The cavity was washed with hydrogen peroxide repeatedly to induce thermal necrosis of the remnant tumor cells. A final curettage of the inner margins was done using a burr. Subchondral bone was observed to be normal, and hence, joint was preserved. The cavity was washed again with hydrogen peroxide, and antibiotic-coated bone cement was used to fill up the entire dead space in the cavity. Once the cement was set, a local wound wash was given at the incision site and wound closed in layers. The curetted material was sent for histopathological studies(Fig. 4).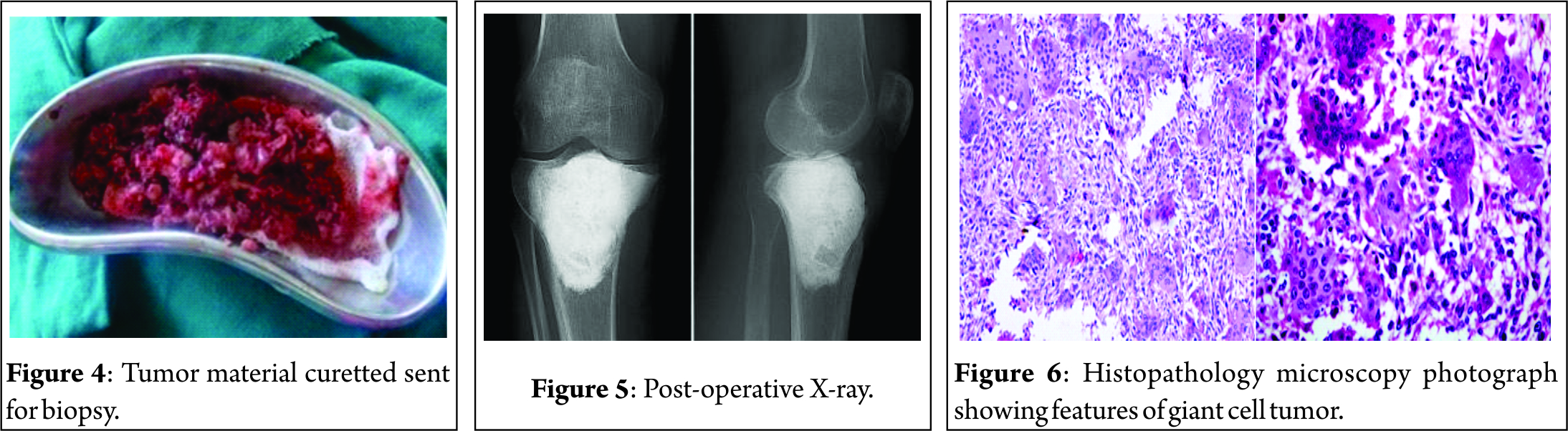
Post-operative radiographs confirmed that the cavity had been completely packed with cement and no dead space was evident (Fig. 5). The post-operative period was uneventful. Weight-bearing was initiated 10 days after surgery. She achieved full range of motion of her knee joint in 3 weeks.
Histopathology
Multiple sections showed many multinucleated osteoclast-like giant cells, uniformly distributed in sheets of spindle to polygonal cells. There was no cellular atypia. Spindle-shaped tumor cells were seen having elongated ovoid nuclei with bland nuclear chromatin and scant to moderate amount of amphophilic cytoplasm. Features were strongly suggestive of GCT (Fig. 6).
Discussion
GCT is a benign aggressive tumor usually affecting the ends of long bones. GCT accounts for 5% of all bone tumors and 20% of all benign tumors [1, 2, 3]. It is commonly understood by orthopedic surgeons to present in individuals in their third decade of life after the closure of the physis [1]. We report our patient who was diagnosed with CGT at an unusual age of 15 years. The incidence of GCT in pediatric patients ranges from 1.8% to 7.5% [4]. GCT does not behave in a predictable fashion. The severity of symptoms rarely corresponds to the radiographic or histological grade of the tumor [2]. This presents an on-going debate on how to diagnose this tumor at the earliest. A patient with GCT usually presents to the treating surgeon with pain, restriction of movements of the corresponding joint, and a thickened irregular bone with a palpable “eggshell crackling” cortex. Pathological fracture is the first sign in 15% of the cases [3, 5]. However, our patient presented to us only with vague pain around the knee joint and difficulty in squatting. Diagnosis is usually made by X-rays. These tumors are typically epimetaphyseal in location. They primarily occur in the metaphysic and gradually progress to epimetaphyse allocation once the physis closes[6, 7]. An open physis is believed to restrict the GCT to a metaphyseal location[6, 8]. In our patient, it was epimetaphyseal in site as the physis of the proximal tibia had fused. A further understanding of the lesion with respect to its anatomy, extent, and the plan of surgical approach can be achieved by MRI or computed tomography scans. A confirmation can only be achieved by excision biopsy. The treatment of this tumor should be aimed at local control of the disease and maintain adequate function of the corresponding joint [2]. Tumor control can be achieved by wide surgical excision in most cases. After en bloc surgery, the rate of recurrence has been reported to be 0–5% [3, 9, 10, 11, 12, 13]. This would automatically be preferred choice of treatment by most surgeons. However, wide excision can be performed only in sites such as distal ulna, proximal fibula, or distal radius where function of the limb would not be severely compromised. GCT has been studied to occur in the epiphysis of long bones and hence has a predisposition to affect subchondral bone. In these cases, articular cartilage would have to be sacrificed in en bloc resection surgery and complex reconstruction surgeries necessitated. This could lead to severe loss in function and decrease in quality of life of the patient. The authors therefore recommend extended curettage of primary lesions and wide excision with reconstruction surgeries for recurrent lesions. Curettage is an effective treatment modality. However, recurrences have been reported to be 30–50% [3, 14, 15]. This warrants the use of adjuvant therapy which presumably removes remnant tumor cells after curettage by their chemical (phenol, hydrogen peroxide, and alcohol) or thermal properties (liquid nitrogen and methylmethacrylate). However, the authors have studied that the most predictive factor for a successful surgical outcome in terms of local recurrence is adequate and thorough curettage[6, 16]. Bone cement has been widely used due to the fact that it is cheap and allows immediate weight bearing. It also allows the treating surgeon to detect recurrences very early by radiographs or MRI images [3, 17, 18]. We adopted this treatment and had excellent results. The patient had a knee society score of 93 at the end of 18 months follow-up. She had no restrictions in using her knee joint. Radiographs confirmed no local recurrence.
Conclusion
GCT of the bone is extremely rare in skeletally immature patients. This particular case highlights the need for keeping the diagnosis of GCT at the periphery of one’s vision when dealing with pediatric patients presenting with osteolytic lesion at the epimetaphysis of long bones. Campanacci Grade 3 lesions have six-fold increase in the risk of pulmonary metastasis, and hence, a minimum of 5 years follow-up is recommended by the authors to rule out pulmonary metastasis [1,19].
Clinical Message
Giant cell continues to present as patients with dull pain near the knee, however, keeping the diagnosis, as one of the probable causes in the younger patients will go a long way in establishing the diagnosis early. Prompt diagnosis and early intervention may help stop the recurrence.
References
1. Turcotte RE. Giant cell tumor of bone. Orthop Clin North Am 2006;37:35-51.
2. Campannaci M, Baldini N, Boriani S, Sudanese A. Giant cell tumor of bone. JBone Joint Surg Am 1987;69:105-44.
3. Szendroi M. Giant cell tumour of bone. J Bone Joint Surg [Br] 2004;86-B:5-12.
4. Puri A, Agarwal MG, Shah M, Jambhekar NA, Anchan C, Behle S, et al. Giant cell tumor of bone in children and adolescents. J Pediatr Orthop 2007;27:635-9.
5. Dreinfhöfer KE, Rydholm A, Bauer HC, Kreicbergs A. Giant-cell tumors with fracture at diagnosis. J Bone Joint Surg [Br] 1995;77-B:189-93.
6. Sharma V, Sharma S, Mistry KA, Awasthi B, Verma L, Singh U, et al. Giant cell tumor of bone in skeletally immature patients-A clinical perspective. J Orthop Case Rep 2015;5:57-60.
7. Rietveld LA, Mulder JD, Brûtel de la Rivière G, van Rijssel TG. Giant cell tumour: Metaphyseal or epiphyseal origin? Diagn Imaging 1981;50:289-93.
8. Jundt G. Pathologic-anatomic characteristics of benign bone tumors. Orthopade 1995;24:2-14.
9. Gitelis S, Mallin BA, Piasecki P, Turner F. Intralesional excision compared with en bloc resection for giant-cell tumors of bone. J Bone Joint Surg Am 1993;75:1648-55.
10. Kumta SM, Leung PC, Yip K, Hung LK, Panozzo A, Kew J, et al. Vascularized bone grafts in the treatment of juxta-articular giant-cell tumors of the bone. J Reconstr Microsurg 1998;14:185-90.
11. Labs K, Perka C, Schmidt RG. Treatment of stages 2 and 3 giant-cell tumor. Arch Orthop Trauma Surg 2001;121:83-6.
12. O’Donnell RJ, Springfield DS, Motwani HK, Ready JE, Gebhardt MC, Mankin HJ, et al. Recurrence of giant-cell tumors of the long bones after curettage and packing with cement. J Bone Joint Surg Am 1994;76:1827-33.
13. Yip KM, Leung PC, Kumita SM. Giant cell tumor of bone. Clin Orthop 1996;323:60-4.
14. Campannaci M, Giunti A, Olmi R. Giant-cell tumours of bone: A study of 209 cases withlong term follow up in 130. Ital J Orthop Traumatol 1975;1:249-77.
15. Goldengerg RK, Campbell CJ, Bonfiglio M. Giant cell tumor of bone: An analysis of two hundred and eighteen cases. J Bone Joint Surg [Am] 1970;52-A:619-64.
16. Prosser GH, Baloch KG, Tillman RM, Carter SR, Grimer RJ. Does curettage without adjuvant therapy provide low recurrence rates in giant-cell tumors of bone? Clin Orthop Relat Res 2005;435:211-8.
17. Szendröi M. Adjuvant therapy (phenol, bone cement) in giant cell tumor. Z Orthop1992;130:95-9.
18. Bertoni F, Present D, Enneking WF. Giant-cell tumor of bone with pulmonary metastases. J Bone Joint Surg [Am] 1985;67-A:890-900.
19. Rock MG, Pritchard DJ, Unni KK. Metastases from histologically benign giant-cell tumor of bone. JBoneJoint Surg[Am] 1984;66:269-74.
 |
 |
 |
 |
 |
| Dr. Vijay C | Dr. Supreeth Nekkanti | Dr. Ravi Shankar | Dr. ShashiKiran R | Dr. Sunila |
| How to Cite This Article: VijayC, NekkantiS, RaviShankar R, ShashiKiran R, Sunila R. An Unusual Presentation of Giant Cell Tumor of the Tibia in a Skeletally Immature Patient. Journal of Orthopaedic Case Reports 2018. May- June; 8(3): 10-13. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 October 10, 2022 Giant Cell Tumor of Talus – A Case Report
October 10, 2022 Giant Cell Tumor of Talus – A Case Report- November 10, 2020 A Case Report of Giant Cell Tumor in the Thumb Distal Phalanx
 December 1, 2025 Recurrent Giant Cell Tumor of the Carpal Bones in an Adult Male Managed by En-bloc Excision, Extended Curettage, Bone Grafting, and all-Kirschner Wire Fixation: A Rare Case Report and Literature Review
December 1, 2025 Recurrent Giant Cell Tumor of the Carpal Bones in an Adult Male Managed by En-bloc Excision, Extended Curettage, Bone Grafting, and all-Kirschner Wire Fixation: A Rare Case Report and Literature Review December 1, 2025 Tuberculous Dactylitis (Bilateral Spina Ventosa) of Proximal Phalanx in a 6-Year-Old Girl: A Case Report
December 1, 2025 Tuberculous Dactylitis (Bilateral Spina Ventosa) of Proximal Phalanx in a 6-Year-Old Girl: A Case Report