
[box type=”bio”] Learning Point for the Article: [/box]
Patellar stress fractures, even with clearly visible minimally displaced fracture line, can successfully be treated conservatively with non-operative management.
Case Report | Volume 8 | Issue 4 | JOCR July – August 2018 | Page 45-48| Steven Baker, Jacob Seales, Scotty Newcomer, Jeremy Bruce. DOI: 10.13107/jocr.2250-0685.1154
Authors: Steven Baker[1], Jacob Seales[1], Scotty Newcomer[1], Jeremy Bruce[1]
[1]Department of Orthopaedic Surgery, University of Tennessee College of Medicine Chattanooga, Erlanger Health System, United States.
Address of Correspondence:
Dr. Steven Baker,
Department of Orthopaedic Surgery, 975 East Third Street, Hospital Box 287, Chattanooga, TN 37403, USA.
E-mail: Steven.Baker@erlanger.org
Abstract
Introduction: The overuse and repetitive loading of a bone cause a stress fracture, commonly occurring in the weight-bearing structures of the lower extremities of athletes, but rarely the patella. Patella stress fractures are an extremely rare occurrence. Müller first described a patella stress fracture in 1943; however, we could find <15 reported cases in literature since that time. Thus, some uncertainty exists as to the proper treatment of this very rare condition.
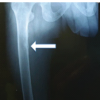
Case Report: A female collegiate gymnast presented with 2–3 months of anterior knee pain, and initial radiographs revealed a non-displaced patella stress fracture. An magnetic resonance imaging (MRI)was obtained which confirmed the diagnosis and ruled out any patellar tendon or intra-articular pathology. The patient was treated with immobilization, vitamin supplementation, and low-intensity pulsed ultrasound therapy. At 3 months, the patient had complete healing of her fracture and returned to full competition in her sport. After approximately 1year of returning to sport, she unfortunately developed a patella stress fracture in her contralateral knee confirmed by radiographs and MRI. She received the same conservative management plan as before, and at 3 months, she was pain free and returned to full competition in her sport. She is now 3 years from injury on the right knee and 2 years from injury on the left knee and continues to compete at the Division I collegiate level without pain.
Conclusion: This case report illustrates how patella stress fractures may be successfully treated conservatively, even when presenting with a radiographic fracture line. This varies from other forms of stress fractures where surgical fixation is recommended once radiographic fracture line is noted. This is likely due to the abundant blood supply in the region, which allows for healing.
Keywords: Patella stress fracture, stress fracture, patella.
Introduction
The overuse and repetitive loading of a bone causes a stress fracture, commonly occurring in the weight-bearing structures of the lower extremities of athletes, but rarely the patella. Patella stress fractures are an extremely rare occurrence. Müller first described a patella stress fracture in 1943 (1); however, we could find <15 reported cases in literature since that time [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12]. The patella is a sesamoid bone embedded within the extensor mechanism of the knee. The joint reactive forces of the patellofemoral joint can be as much as 7 times a person’s body weight [13]. The patella has a profound blood supply that receives its contribution from six different vessels about the knee [14]. This network of vessels forms a vascular ring around the patella with the overall blood flow running from distal to proximal, which likely help explains the rarity of patella stress fractures [15]. Patients with a patella stress fracture usually present with anterior knee pain. Anterior knee pain is a very common complaint in the general population with a wide etiology, of which patella stress fracture is very low on the differential diagnosis. Thus, a thorough history and examination as well as appropriate imaging are required to reveal the diagnosis. Once the diagnosis is made, some uncertainty exists as to the course of treatment, as this is a very rare condition that has not been extensively studied. The goal of treatment is to obtain healing of the stress fracture while avoiding displacement. Conservative management includes immobilization in a cast or brace, locked in extension, with partial or non-weight bearing for 4–6weeks.Low-intensity pulsed ultrasound (LIPUS) has shown some promise in aiding in healing fractures with delayed union [16, 17, 18, 19]. Vitamin D and calcium supplementation are recommended. Serial radiographs should be taken to monitor healing. If the patient fails a trial of non-operative management or significant displacement occurs, then surgical fixation with or without bone grafting/biological augmentation would be recommended.
Case Report
A 17-year-old female high school senior gymnast, who had signed a full scholarship offer for Division I collegiate gymnastics, initially presented to our office after 3 months of anterior knee pain. Her pain had gradually worsened in severity over this time period and was, especially, painful with dismounts and jumping activities. She had previously sought treatment with her primary care physician who had diagnosed her with patellar tendonitis and was being managed conservatively with the help of the school’s athletic trainer. She denied any history of amenorrhea, eating disorders, or previous stress fractures. Initial radiographs obtained in our office revealed what appeared to be a non-displaced transverse fracture of the inferior pole of the patella (Fig. 1).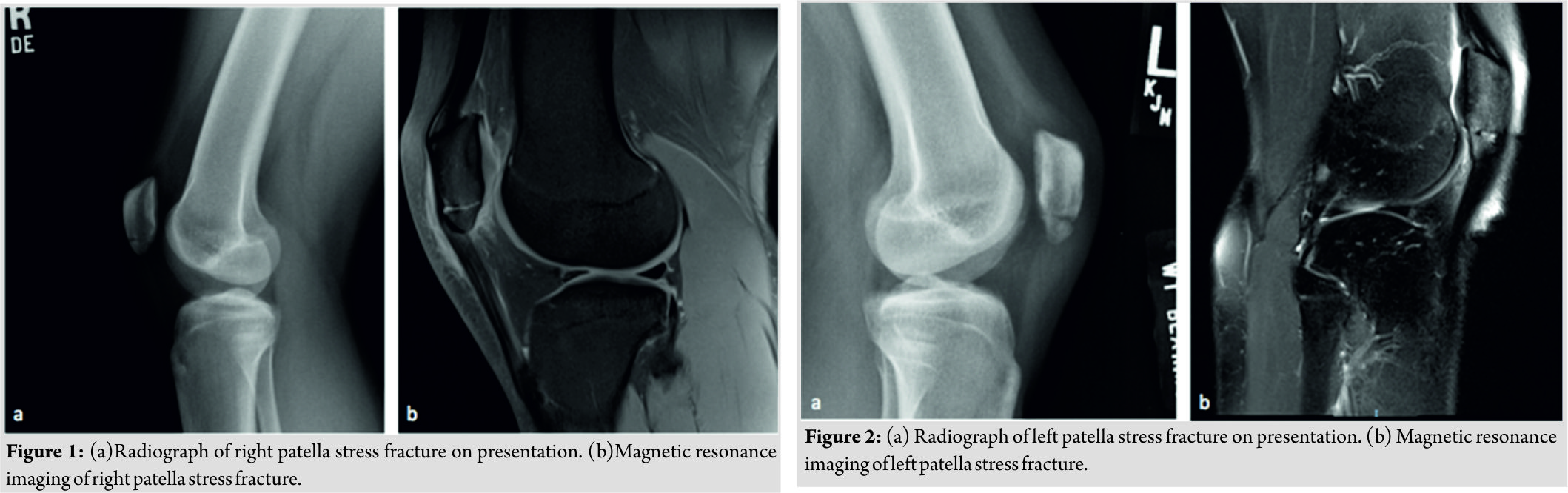 An MRI was obtained that confirmed the diagnosis of a patellar stress fracture and ruled out any patella tendon or intra-articular pathology (Fig. 1). The patient was immobilized in a hinged knee brace, locked in extension. She was also prescribed Vitamin D and calcium supplementation as well as daily use of an Exogen® LIPUS system(Bioventus LLC, Durham, NC, USA). It was discussed with the patient that since the injury was 2–3 months’ old, she was at a higher risk for failing conservative treatment, which would require operative fixation. At 1month follow-up, radiographs were obtained that showed early callus formation, and her examination revealed a clinical decrease in her pain. She was then progressed to weight bearing as tolerated with gradual increase in her range of motion guided by physical therapy. At 2 months, radiographs showed fracture healing, and we began gradual reintegration of gymnastics with limitations on tumbling/dismounting/jumping activities. At 3 months, she was allowed to return to full competition. After approximately 1year of returning to sport and competing as a collegiate gymnast, she unfortunately began to develop similar symptoms as before, now in her contralateral knee. She presented back to our office where we confirmed the diagnosis of a stress fracture of the inferior pole of the contralateral patella, similar to her previous injury (Fig. 2). At that visit, radiographs revealed complete healing of her prior stress fracture from 1year ago. She was given the same conservative management plan of a period of immobilization in a hinged knee brace locked in extension, Vitamin D and Calcium supplementation, daily use of LIPUS, and later progressed to physical therapy with guided return to gymnastic activities. At 3 months, she was pain free, and a Knee Injury and Osteoarthritis Outcome Score (KOOS) survey was obtained [Graph1][20]. With the KOOS showing favorable results, in addition to being pain free, the patient was allowed a full return to competition(Fig. 3). She is now 3 years from injury on the right knee and 2years from injury on the left knee and continues to compete at the Division I collegiate level without pain(Fig. 4).
An MRI was obtained that confirmed the diagnosis of a patellar stress fracture and ruled out any patella tendon or intra-articular pathology (Fig. 1). The patient was immobilized in a hinged knee brace, locked in extension. She was also prescribed Vitamin D and calcium supplementation as well as daily use of an Exogen® LIPUS system(Bioventus LLC, Durham, NC, USA). It was discussed with the patient that since the injury was 2–3 months’ old, she was at a higher risk for failing conservative treatment, which would require operative fixation. At 1month follow-up, radiographs were obtained that showed early callus formation, and her examination revealed a clinical decrease in her pain. She was then progressed to weight bearing as tolerated with gradual increase in her range of motion guided by physical therapy. At 2 months, radiographs showed fracture healing, and we began gradual reintegration of gymnastics with limitations on tumbling/dismounting/jumping activities. At 3 months, she was allowed to return to full competition. After approximately 1year of returning to sport and competing as a collegiate gymnast, she unfortunately began to develop similar symptoms as before, now in her contralateral knee. She presented back to our office where we confirmed the diagnosis of a stress fracture of the inferior pole of the contralateral patella, similar to her previous injury (Fig. 2). At that visit, radiographs revealed complete healing of her prior stress fracture from 1year ago. She was given the same conservative management plan of a period of immobilization in a hinged knee brace locked in extension, Vitamin D and Calcium supplementation, daily use of LIPUS, and later progressed to physical therapy with guided return to gymnastic activities. At 3 months, she was pain free, and a Knee Injury and Osteoarthritis Outcome Score (KOOS) survey was obtained [Graph1][20]. With the KOOS showing favorable results, in addition to being pain free, the patient was allowed a full return to competition(Fig. 3). She is now 3 years from injury on the right knee and 2years from injury on the left knee and continues to compete at the Division I collegiate level without pain(Fig. 4).
Discussion
Patella stress fractures are a rare injury encountered by orthopedic surgeons. This case is particularly interesting as the patient had been symptomatic for approximately 3months. Given the chronicity of the injury at presentation, the patient is at high risk of failing conservative non-operative management, and it could be argued that one should proceed with surgical fixation. Due to the rare nature of this type of stress fracture, there is not much evidence to support treatment guidelines. In other stress fractures of the lower extremities that are chronic and have a visible fracture line, such as anterior tibia shaft and femoral neck fractures, surgical fixation is the recommended treatment. However, we feel that the patella is unique in that it has an adequate blood supply to allow healing, even when presenting late and having radiographic changes. This abundant blood supply may also explain why it is such a rare location for a stress fracture, further supporting an initial trial of conservative management. In addition, most cases will involve athletes that place high loads on their patellofemoral joint where screws/implants at the patella and patella tendon can have detrimental effects on performance. This case report supports a trial of non-operative care for patella stress fracture even with a visible fracture line on radiographs.
Conclusion
Patella stress fractures are a very rare condition, as such there are limited data to support treatment guidelines. For other stress fractures of the lower extremities, surgical fixation is recommended once a radiographic fracture line is noted. However, patella stress fractures may be successfully treated conservatively, even when presenting with a radiographic fracture line. This is likely due to the abundant blood supply in the region, which allows for healing.
Clinical Message
Patella stress fractures may be successfully treated conservatively, even when presenting with a radiographic fracture line with or without mild displacement.
References
1. Müller W. Der militärischeabrissermüdungsschaden. DtschMilitararzt 1943;8:283-6.
2. Devas MB. Stress fractures of the patella. J Bone Joint Surg 1960;42B:71-4.
3. Rockett JF, Freeman BL. Stress fracture of the patella: Confirmation by triple-phase bone imaging. Clin Nucl Med 1990;15:873-5.
4. Piétu G, Hauet P. Stress fracture of the patella. Acta OrthopScand 1995;66:481-2.
5. Mata SG, Grande MM, Ovejero AH. Transverse stress fracture of the patella: A case report. Clin J Sport Med 1996;6:259-61.
6. Teitz CC, Harrington EM. Patellar stress fracture. Am J Sports Med 1992;20:761-6.
7. Crane TP, Spalding JW. The management of patella stress fractures and the symptomatic bipartite patella. Oper Tech Sports Med 2009;17:100-5.
8. Sillanpää PJ, Paakkala A, Paakkala T, Mäenpää H, Toivanen J. Displaced longitudinal stress fracture of the patella: A case report. J Bone Joint Surg Am 2010;92:2344-7.
9. Schranz PJ. Stress fracture of the patella. Br J Sports Med 1988;22:169.
10. Keeley A, Bloomfield P, Cairns P, Molnar R. Iliotibial band release as an adjunct to the surgical management of patellar stress fracture in the athlete: A case report and review of the literature. Sports Med ArthroscRehabilTherTechnol 2009;1:15.
11. Brogle PJ, Eswar S, Denton JR. Propagation of a patellar stress fracture in a basketball player. Am J Orthop 1997;26:782-4.
12. Crowther MA, Mandal A, Sarangi PP. Propagation of stress fracture of the patella. Br J Sports Med 2005;39:e6.
13. Griesser MJ, Hussain WM, McCoy BW, Parker RD. Extensor mechanism injuries of the knee. In: Miller MD, editor. Delee&Drez’sOrthopaedic Sports Medicine: Principles and Practice. 4th ed. Vol. 1. Philadelphia, PA: Saunders; 2015. p. 1272-12.
14. Scapinelli R. Blood supply of the human patella: Its relation to ischaemic necrosis after fracture. J Bone Joint Surg Br 1967;49:563-70.
15. Lazaro LE, Wellman DS, Klinger CE, Dyke JP, Pardee NC, Sculco PK, et al. Quantitative and qualitative assessment of bone perfusion and arterial contributions in a patellar fracture model using gadolinium-enhanced magnetic resonance imaging: A cadaveric study. J Bone Joint Surg Am 2013;95:e1401-7.
16. Yoshinobo W, Takashi M, Mohit B, Zdero R, Schemitsch E. Ultrasound for fracture healing: Current evidence. J Orthop Trauma 2010;24:56-61.
17. Li J, Waugh LJ, Hui SL, Burr DB, Warden SJ. Low-intensity pulsed ultrasound and nonsteroidal anti-inflammatory drugs have opposing effects during stress fracture repair. J Orthop Res 2007;25:1559-67.
18. Uchiyama Y, Nakamura Y, Mochida J, Tamaki T. Effect of low-intensity pulsed ultrasound treatment for delayed and non-union stress fractures of the anterior mid-tibia in five athletes. Tokai J ExpClin Med 2007;32:121-5.
19. Mayr E, Frankel V, Rüter A. Ultrasound–an alternative healing method for nonunions? Arch Orthop Trauma Surg 2000;120:1-8.
20. Roos EM, Lohmander LS. The knee injury osteoarthritis outcome score (KOOS): From joint injury to osteoarthritis. Health Qual Life Outcomes 2003;1:64.
 |
 |
 |
 |
| Dr. Steven Baker | Dr. Jacob Seales | Dr. Scotty Newcomer | Dr. Jeremy Bruce |
| How to Cite This Article: Baker S, Seales J, Newcomer S, Bruce J. A Case Report: Bilateral Patella Stress Fractures in a Collegiate Gymnast. Journal of Orthopaedic Case Reports 2018 Jul-Aug; 8(4): 45-48. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Adult-Onset Fanconi Syndrome Presenting as Stress Fractures: A Case Report
December 1, 2025 Adult-Onset Fanconi Syndrome Presenting as Stress Fractures: A Case Report September 1, 2025 Calcaneus and Traumatic Stress Fracture
September 1, 2025 Calcaneus and Traumatic Stress Fracture May 1, 2025 Patellar Osteoid Osteoma: A Rare Cause for Anterior Knee Pain
May 1, 2025 Patellar Osteoid Osteoma: A Rare Cause for Anterior Knee Pain March 1, 2025 Simultaneous Bilateral Knee Extensor Mechanism Injury in a Young Male: A Clinical Diagnosis and Literature Review
March 1, 2025 Simultaneous Bilateral Knee Extensor Mechanism Injury in a Young Male: A Clinical Diagnosis and Literature Review