
• Fanconi syndrome can present de novo in adults and mimic primary bone disorders, such as osteoporosis or vitamin D deficiency, leading to significant diagnostic delays when musculoskeletal symptoms predominate. • Routine biochemical screening for hypophosphatemia, glucosuria without hyperglycemia, and metabolic acidosis is essential in patients presenting with unexplained or recurrent fractures, as these are key clues to underlying proximal tubular dysfunction. • Interdisciplinary evaluation involving orthopedics, nephrology, and endocrinology is crucial in cases where initial presentation is atypical or a secondary cause cannot be identified. • The timely initiation of alkali therapy and vitamin D supplementation can reduce morbidity by preventing further fractures and improving bone health, even if the specific etiology of Fanconi syndrome remains unidentifiable. • This case demonstrates the need for heightened clinical suspicion and early renal evaluation in patients with metabolic bone disease, particularly when classic renal symptoms are absent and standard osteoporosis treatments fail or are inappropriate.
Dr. Namesh Kamat, Department of Nephrology, Sri Venkateswara Institute of Medical Sciences, Tirupati, India. E-mail: nameshkamat217@gmail.com
Abstract
Introduction: Fanconi syndrome is a disorder characterized by defective proximal renal tubular reabsorption, resulting in the wasting of glucose, phosphate, bicarbonate, amino acids, and uric acid. While most common in childhood and usually secondary to other conditions in adults, idiopathic cases with adult onset are rare. Skeletal complications such as osteomalacia and fractures may result from chronic phosphate loss and can be the initial presentation in adult cases.
Case Report: A 35-year-old previously healthy man presented with chronic back pain and bilateral hip pain, later diagnosed as bilateral femoral neck stress fractures. Laboratory evaluation revealed hypophosphatemia, renal glucosuria with normoglycemia, aminoaciduria, phosphaturia, tubular proteinuria, and proximal renal tubular acidosis. Secondary causes were excluded, and genetic testing was not feasible, leading to a diagnosis of idiopathic adult-onset Fanconi syndrome. The patient was treated with sodium bicarbonate and potassium citrate, resulting in improvement and prevention of further fractures.
Conclusion: This case demonstrates that adult-onset Fanconi syndrome, though rare, can initially present with musculoskeletal symptoms such as stress fractures. Early recognition and interdisciplinary evaluation are essential for timely intervention, which may prevent further complications even in the absence of an identifiable cause.
Keywords: Stress fracture, renal Fanconi syndrome, renal tubular acidosis, glucosuria.
Fanconi syndrome is characterized by defective reabsorption in the proximal renal tubules, leading to urinary loss of glucose, phosphate, bicarbonate, amino acids, and uric acid.[1] While typically encountered in children due to inherited metabolic disorders such as cystinosis or galactosemia, the syndrome in adults is usually secondary to systemic diseases, heavy metal toxicity, or drug exposure.[2] Idiopathic adult-onset Fanconi syndrome remains rare, with limited cases reported in the literature. Skeletal manifestations, including osteomalacia, osteoporosis, and fractures, result from chronic phosphate wasting and metabolic acidosis.[3] Stress fractures may precede the diagnosis of Fanconi syndrome, particularly when renal manifestations are subtle or overlooked. We describe a patient in whom Fanconi syndrome presented late in life with bilateral femoral neck stress fractures, underlining the importance of considering renal tubular disorders in the differential diagnosis of metabolic bone disease.
A 35-year-old man presented to our hospital for the evaluation of stress fracture of neck of the femur. He was previously healthy except for lower back ache which bothered the patient every now and then during the previous 4–5 years. His aches and pain had worsened over the past 1 year, and he even developed pain in the hip while walking for which he was seen in the orthopedic outpatient department and the patient was diagnosed to have osteoporosis with stress fracture of the neck of femur on both sides. During his evaluation for stress fracture, he was found to have hypophosphatemia, and hence, the patient was referred to internal medicine for further evaluation. (Fig. 1)
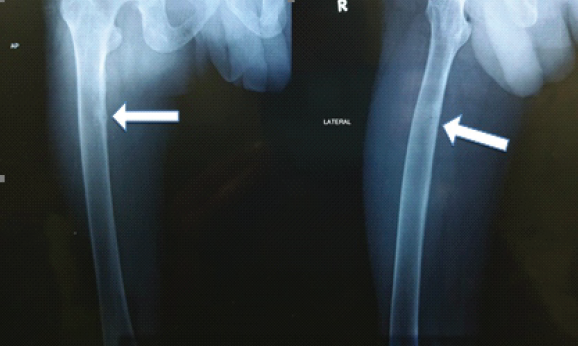
Figure 1: X-ray of right femur showing looser zones (white arrows) indicating pseudo fractures.
On evaluation, his blood pressure was 110/76 mmHg, and physical examination was normal except for slight restriction of the hip joint due to pain. Urine analysis revealed the following: Specific gravity of 1.020, pH 5.5, albumin ++, glucose +++, red blood cell 1–2/HPF, and white blood cell 0–2/HPF. The following laboratory values were obtained: Serum calcium, 8.7 mg/dL; phosphorus, 1.7 mg/dL; uric acid, 1.8 mg/dL; cholesterol, 139 mg/dL; protein, 7 g/dL; albumin, 4.5 g/dL; blood urea nitrogen, 9 mg/dL; creatinine, 0.97 mg/dL; glucose, 91 mg/dL; and HbA1c, 5.30%. His estimated glomerular filtration rate was 101 mL/min/1.73m2, calculated using the Chronic Kidney Disease Epidemiology Collaboration equation. The following values were obtained in 24-h urine monitoring: protein, 1.25 g; potassium, 39.7 mmol; chloride, 329.51 mmol; calcium, 174.68 mg; glucose, 20797 mg; and creatinine, 1.056 g.
Fractional excretions of calcium and phosphorus were 1.84% and 44.1%, respectively. The serum 25(OH) vitamin D level was 30.5 ng/mL. His magnetic resonance imaging and computed tomography scan of both hip joints showed an acute stress fracture of the right femoral neck and findings consistent with pseudo fractures, i.e., Looser’s zone of osteomalacia, which are suggestive of metabolic bone disease.
The serum concentrations of sodium, potassium, chloride, and total CO2 were 138, 3.7, 111, and 27.9 mmol/L, respectively. Arterial blood gas analysis revealed the following values: pH, 7.25; PaCO2, 36 mmHg; PaO2, 105.1 mmHg; and HCO3−, 14 mmol/L. The urine sodium, potassium, chloride, and creatinine concentrations were 63 mmol/L, 10 mmol/L, 63 mmol/L, and 26.6 mg/dL, respectively. Ultrasound of the abdomen was performed for liver echo texture and kidney size, which was found to be normal.
A thorough history was taken about drugs taken and exposure to lead. Plasma cell dyscrasias were ruled out by normal blood smear and bone marrow examination and a normal globulin level and urinary analysis negative for Bence–Jones protein. Slit-lamp examination was negative for KF rings of Wilson’s disease and cystinosis. Genetic analysis for mutations could not be done due to the unavailability of these tests in our center.
Following the above results, the patient was diagnosed with idiopathic Fanconi syndrome and was managed with oral sodium bicarbonate and oral potassium citrate, stress fracture was managed conservatively, and the patient was followed up at regular intervals.
This case demonstrates that Fanconi syndrome, although classically pediatric, can present for the first time in adulthood with orthopedic complaints. The patient’s late presentation with stress fractures reflects the cumulative effects of chronic phosphate and bicarbonate wasting.
Diagnostic challenge:
- The initial presentation was orthopedic (back pain and hip fractures), without overt renal symptoms such as severe polyuria or electrolyte crises
- Musculoskeletal complaints overshadowed renal abnormalities, leading to years of under-recognition
- Stress fractures and osteomalacia are often attributed to primary osteoporosis or vitamin D deficiency, causing a delay in recognizing the renal tubular disorder
- The absence of an identifiable secondary cause (drugs, toxins, and systemic disease) made the diagnosis of idiopathic Fanconi syndrome one of exclusion [4].
Clinical implications:
- Consider renal tubular disorders in bone disease – Patients presenting with recurrent or bilateral stress fractures, particularly at atypical sites, should be screened for phosphate, bicarbonate, and glucose wasting [5].
- Routine biochemical clues are critical – Hypophosphatemia, glucosuria in the absence of hyperglycemia, and metabolic acidosis are red flags that should not be overlooked [6].
- Interdisciplinary evaluation is key – Collaboration between orthopedics, nephrology, and endocrinology can help avoid diagnostic delays [7].
- Therapeutic potential – Early initiation of alkali therapy and vitamin D supplementation may prevent further fractures, improve bone health, and reduce morbidity even when the underlying etiology remains elusive [8,9,10].
Fanconi syndrome can rarely present de novo in adulthood and manifest primarily as orthopedic complications such as stress fractures. This case underscores both the diagnostic challenge and the need for heightened clinical suspicion. Unexplained fractures or osteomalacia should prompt evaluation for renal tubular dysfunction, as timely recognition and treatment can substantially improve patient outcomes.
Adult-onset Fanconi syndrome, though rare, can manifest initially as musculoskeletal complaints such as stress fractures and osteomalacia rather than classic renal symptoms. This case of a 35-year-old man underscores the importance of considering renal tubular disorders in the differential diagnosis of unexplained or atypical bone disease. Early recognition and interdisciplinary collaboration are critical for timely intervention, which may prevent further skeletal complications and improve long-term outcomes, even when the underlying etiology remains idiopathic.
References
- 1. Foreman JW. Fanconi syndrome, a general overview. Pediatr Nephrol 2015;30:171-8. [Google Scholar] [PubMed]
- 2. Izzedine H, Launay-Vacher V, Isnard-Bagnis C, Deray G. Drug-induced Fanconi’s syndrome. Am J Kidney Dis 2003;41:292-309. [Google Scholar] [PubMed]
- 3. Klootwijk ED, Reichold M, Helip-Wooley A, Tolaymat A, Broeker C, Robinette SL, et al. Mistargeting of peroxisomal EHHADH and inherited renal Fanconi’s syndrome. N Engl J Med 2014;370:129-38. [Google Scholar] [PubMed]
- 4. Emma F, Montini G, Parikh SM, Salviati L. Renal Fanconi syndrome: Taking a proximal look at the nephron. Nephrol Dial Transplant 2016;31:375-81. [Google Scholar] [PubMed]
- 5. Fan Y. A Case of fanconi syndrome with multiple fractures and height loss as main symptoms caused by adefovir dipivoxil. Ann Clin Med Case Rep 2025;15:1-5. [Google Scholar] [PubMed]
- 6. Rao M, Dadey L, Glowa T, Veldkamp P. Fanconi syndrome leading to hypophosphatemic osteomalacia related to tenofovir use. Infect Dis Rep 2021;13:448-53. [Google Scholar] [PubMed]
- 7. Lee JH, Byun YS, Cha BS, Nam MS, Song YD, Lim SK, et al. A case of adult fanconi syndrome with hypophosphatemic osteomalacia. Endocrinol Metab 1996;11:93-101. [Google Scholar] [PubMed]
- 8. Hall AM, Bass P, Unwin RJ. Drug-induced renal Fanconi syndrome. QJM 2014;107:261-9. [Google Scholar] [PubMed]
- 9. Harrison HE. The Fanconi syndrome. J Chronic Dis 1958;7:346-55. [Google Scholar] [PubMed]
- 10. Oliveri MB, Cassinelli H, Bergada C, Mautalen CA. Bone mineral density of the spine and radius shaft in children with X-linked hypophosphatemic rickets (XLH). Bone Miner 1991;12:91-100. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Malleolar Stress Fracture as the First Manifestation of Undiagnosed Crohn’s Disease: A Case Report
June 1, 2026 Malleolar Stress Fracture as the First Manifestation of Undiagnosed Crohn’s Disease: A Case Report September 1, 2025 Calcaneus and Traumatic Stress Fracture
September 1, 2025 Calcaneus and Traumatic Stress Fracture July 10, 2024 Return to Sports in Stress Reaction and Stress Fractures in Indian Athletes: A Case Series
July 10, 2024 Return to Sports in Stress Reaction and Stress Fractures in Indian Athletes: A Case Series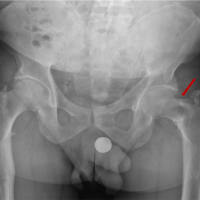 February 10, 2023 Case Report of Femoral Neck Stress Fracture in X-linked Hypophosphatemic Rachitis Patient Treated with Mechanical Axis Correction and a Literature Review
February 10, 2023 Case Report of Femoral Neck Stress Fracture in X-linked Hypophosphatemic Rachitis Patient Treated with Mechanical Axis Correction and a Literature Review