
[box type=”bio”] Learning Point of the Article: [/box]
Appropriate placement and movements of the trocar avoids bleeding complications for BKP.
Case Report | Volume 8 | Issue 6 | JOCR November – December 2018 | Page 74-78 | Valerio Pace, Dimpu Bhagawati, Chang Park, Sean Molloy. DOI: 10.13107/jocr.2250-0685.1266
Authors: Valerio Pace[1], Dimpu Bhagawati[1], Chang Park[1], Sean Molloy[1]
[1]Department of Trauma and Orthopaedics, Royal National Orthopaedic Hospital (Stanmore), S.M. Della Misericordia Hospital (Perugia), Italy.
Address of Correspondence:
Dr. Dr. Valerio Pace,
Via Gallenga 68, 06127, Perugia (PG), Italy.
E-mail: valeriopace@doctors.org.uk
Abstract
Introduction: The Royal National Orthopaedic Hospital (RNOH) is a tertiary referral center and patients with spinal complications from multiple myeloma are managed here in a multidisciplinary approach. Balloon kyphoplasty(BKP) procedures are routinely performed in such patients when clinically indicated with good results and a low complication rate. There are little data reported in the literature about post-BKP hematoma formation and its management. We present the first known reported case delayed post-operative psoas hematoma in a myeloma patient following a BKP.
Case Report: A 40-year-old male patient with diagnosed Ig G lambda multiple myeloma was referred to the spinal unit based at the RNOH. An L5 fracture was deemed to be the cause of significant lower back pain. He underwent an L5BKP with good immediate results and in the absence of any immediate complications. Post-operative, the patient had normal distal neurology and was discharged1day postoperatively. 3 days after surgery, he underwent left hamstrings anterior cruciate ligament reconstruction. 2 days following the latter, he developed significant pain in his left groin and thigh associated with numbness. A pelvicmagnetic resonance imaging scan confirmed a left iliopsoas hematoma. This case was treated conservatively under guidance of the multidisciplinary team.
Conclusion: As psoas hematoma, formation is a rare complication following a BKP. The recommended management of a psoas hematoma is conservative with supportive therapy and regular clinical review. To reduce the risk of a psoas hematoma, the authors recommend that the trocar should be first placed on the transverse process and maneuvred medially to the start point on the pedicle. This would avoid injuries to the artery to the pars as well as structures deep to the intertransverse ligament avoiding this rare complication.
Keywords: Orthopedic, Spine, Tumor, Myeloma, Kyphoplasty.
Introduction
Balloonkyphoplasty (BKP) is a minimally invasive procedure designed to stabilize spinal fractures and the resulting correct vertebral deformities[1]. As a variation of the vertebroplasty first developed in the 1980s, BKP uses a minimally invasive technique using a needle to introduce an inflatable balloon into the cancellous bone of the body of the vertebrae. This balloon is subsequently filled with bone cement in a controlled manner to stabilize the fracture and restores any vertebral deformity [1].The most common bone cement used is poly-methyl methacrylate although more recently biodegradable calcium phosphate-based cements have been utilized to avoid the complications of non-biodegradability, monomer toxicity, and the heat generated from its exothermic reaction [2]. Indications for BKP include traumatic vertebral fractures, fracture non-union, osteolysis, and painful vertebral body collapse caused by multiple myelomas and other tumors. Contraindications include infection of the fractured vertebra, a severe hemorrhagic diathesis, known allergies to the cements, and pregnancy [3]. Results present in the literature show that BKP is an effective and safe treatment for treating vertebral fractures in patients with cancer with low complication rates [4,5].Reported complications include symptomatic or asymptomatic cement leakage, epidural hematoma, lumbar artery pseudoaneurysms, and both temporary and permanent neurological symptoms [6]. Bleeding and hematoma formation is rarely reported in percutaneous vertebroplasty procedures [7]. However, these complications should be kept in mind during consideration of a kyphoplasty, especially in light of the multiple medical comorbidities the patients may have[8, 9, 10]. The Royal National Orthopaedic Hospital (RNOH) is a tertiary referral center for spinal patients and patients with spinal complications from multiple myeloma are managed here in a multidisciplinary approach. BKP procedures are performed in patients with vertebral fractures in patients suffering from multiple myeloma. There are little data reported in the literature about post-BKP hematoma formation and its management. We present the first known reported case delayed post-operative psoas hematoma in a myeloma patient following a BKP.
Case Report
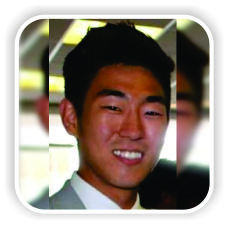
A 40-year-old male patient with diagnosed IgG lambda multiple myeloma was referred to the spinal unit based at the RNOH for specialist advice and transferred to the RNOH for further management. He initially presented to his local hospital with back and rib cage bone pain. He was found to have significant bony involvement of myeloma throughout the skeleton including compression fracture with 40% loss height at L5.For his myeloma, he received two courses of PAD (bortezomib, doxorubicin, and dexamethasone) and four courses of VCD (bortezomib, cyclophosphamide, and dexamethasone)chemotherapyin Poland and London, respectively. Furthermore, he hadmelphalan condition autologous stem cell transplantation in November 2015 and was on maintenance therapy with ixazomib. Investigations in May 2016, including a bone marrow biopsy, highlighted an excellent response to the aforementioned therapy. Despite this, the patient complained of residual lower back pain requiring significant doses of opioids and neuropathic medications. He was also on zoledronic acid infusions and regular Adcal D3 supplements for bone protection. As part of regular follow-up, the patient had amagnetic resonance imaging (MRI) in September 2016 that showed on-going disease process including his lumbar spine and in addition a new central disc bulge at L4-5 level. The patient was consequently referred to the spinal unit at the RNOH for consideration of surgical management of the L5 fracture secondary to the diagnosed myeloma. On presentation to the spinal team at RNOH, he was experiencing residual lower back pain despite excellent response to his treatment, and he was also complaining of sacral pain and pain radiating down into his coccyx. A repeat whole spin and sacrum MRI scan (Fig. 1 and 2) were performed to fully reassess the clinical scenario and this showed:
1. Minor end plate fracture at the level of S1, particularly evident on T1-weighted imaging with no significant changes in appearance compared to the previous scan
2. Confirmed loss of vertebral body height at T5 without involvement of the pedicles
3. Involvement of the left pedicle and posterior elements at the level of L1 unilaterally, particularly evident on T2-weighted imaging and correlating with intermediate signal on T1,stable lesion.
4. In the L5 vertebral body, low signal is noted in both T1 and T2 and fat-saturated images in the anterior vertebral body with what appears to be a low signal fracture line. However, no significant loss of L5 vertebral body height is detected
5. Hemangioma in the anterior vertebral body of T4
6. L4-5 degenerative disc and absence of nerve root or canal compression.
Significant pain was elicited on palpation over the L5 spinous process area during physical examination. Given the clinical and radiological findings and the chronological and anatomical correspondence between onset of symptoms and findings, the new L5 vertebral fracture(described in point number 4) was deemed to be the cause of patient’s symptoms. Given the above results, a BKP was recommended at this stage if no improvement of symptoms in the following weeks. He subsequently had a SPECT computed tomography (CT) scan of the lumbar spine that showed uptake of the superior endplate of the L5 vertebra that was thought likely to be the main pain generator. Furthermore, he had remodeling appearance of the L1 vertebral body and only minor uptake of the S1 vertebral body with no definitive fracture at these levels. Following these results and with no significant further improvement of the symptoms, the decision to proceed with an L5BKP was taken and agreed by all parties to address this as the primary source of pain. The patient was electively admitted to the RNOH on the 13th of August and the procedure was performed on the 14th of August 2017. Routine venous thromboembolisms prophylaxis was provided following the local policy.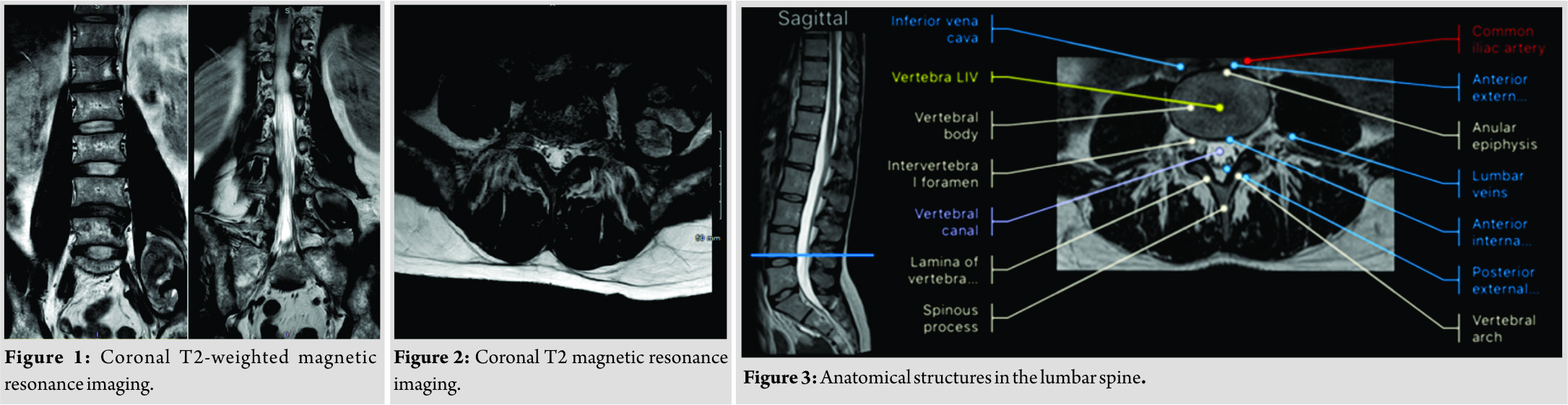
Procedure
The patient was positioned prone on a Jackson table and following standard prepping and draping with the routine who checklist completed. A Jamshidi needle was inserted at the lateral edge of the facet and advanced with a bipedicular approach used as it was difficult to reach the midline. A kyphoplasty balloon was then inflated gently to create the appropriate cavity and cement inserted with the kyphoplasty pump (Medtronic Europe S.A. Route du Molliau CH-1131 Tolochenaz, Switzerland). The procedure was performed under dualimaging intensifier (II) guidance throughout and no immediate complications noted. The wound closure was carried out with monocrylto skin. Postoperatively, the patient was mobilized immediately as pain allowed and following the local kyphoplasty protocol given 48 h of oral co-amoxiclab (625mg 3 times a day). The post-operative review noted that the patient had intact and normal neurology following his procedure and was discharged 1day postoperatively with oral analgesia only. The following day, the patient had a pre-planned elective left anterior cruciate ligament reconstruction with hamstrings harvest and a partial medial meniscectomy. There were no reported intraoperative problems and the patient was subsequently discharged home with no new concerns. Neither issues with regard to the patient’s positioning on the table or the surgical procedure itself were reported. However,5 days following his original kyphoplasty, the patient developed new acute left groin pain radiating to his thigh with new numbness reported in the lateral aspect of his left thigh. Due to the acute onset of these symptoms, he was urgently re-referred to the spinal unit at the RNOH for urgent clinical review and further investigations and management. Clinical examination found some weakness in the left hip flexion but no weakness of dorsiflexion of plantarflexion at the ankle. No other significant clinical findings were found and the rest of distal neurology was intact. There was no clinical, laboratory, or radiological evidence of infection at this time, but a pelvis MRI scan organized on an urgent basis to exclude and new pathology at the lumbar spine and potential operative targets or complications. The MRI showed a well-defined, lobular, encapsulated, and thin-walled soft tissue lesion within the left psoas muscle. The lesion measured 7.8 cm craniocaudally, 4.6 cm from medial to lateral, and 4.2 cm from anterior to posterior. The lesion extended to the level of the iliacus muscle and seemed to represent a hematoma. Satisfactory appearance of the BKP and no cement leakage were noted. No other significant abnormalities or new adjacent fractures were noted. This case was treated with conservative measures given the clinical and radiological findings. Partial weight-bearing with crutches was recommended, and post-operative physiotherapy was also provided. The patient was subsequently followed up 4weeks following surgery whereby the symptoms of pain had significantly improved along with the weakness in hip flexion. At the 3-month follow up period, the patient had a normal neurological examination and had returned to his work as a painter decorator.
Discussion
This report described a pathological L5 fracture in a patient with underlying myeloma who underwent a routine kyphoplasty. Kyphoplasty is proven to be a very safe and effective minimally invasive surgical option to treat the symptoms caused by insufficiency or pathological vertebral fractures. [2, 3, 11]Complications of kyphoplasty include adjacent level fractures and the leakage of cement that may cause neurological complications [5,12, 13, 14, 15, 16]. Cement leakage has been reported to be as high as 14% although only a very small number of these were symptomatic and rate up to 17% of new adjacent fractures [16]. A recent systemic review of kyphoplasty versus vertebroplasty and non-surgical management for the treatment of osteoporotic vertebral compression fractures by Papanastassiou et al. did not identify any cases of post-operative complications of psoas hematoma formation following kyphoplasty although there was one psoas hematoma following vertebroplasty [17]. To the best of our knowledge, this is the first reported case of a symptomatic psoas hematoma following a BKP for a pathological vertebral compression fracture. The patient presented 5 days following his BKP with new-onset weakness in the left hip flexion and the left groin pain suggesting isolated left L2 nerve involvement. As per the literature, the most common complications are cement leakage and adjacent vertebral fractures, and both these should be excluded before the consideration of any rarer post-operative complications. An MRI scan is the recommend image modality following a thorough history and clinical review. The MRI found a hematoma within the left psoas muscle extending to the level of the iliacus muscle. The hematoma was deemed to be caused by a bleed at the time of surgery from the artery of the pars interarticularis (Fig. 3). This likely occurred as the trocar was being positioned before insertion through the cortical bone. We would suggest to avoid this trocar should first be placed on the transverse process and maneuvred medially to the start point on the pedicle. This would avoid injuries to the artery to the pars as well as structures deep to the intertransverse ligament. The authors would advice in the absence of other post-operative complications the recommended management of a psoas hematoma would be conservative management with supportive measures of analgesia, physiotherapy, and regular clinical review to ensure that the neurological deficit improves as the hematoma resorbs in time.
Conclusion
This is a unique case of delayed hemorrhage following kyphoplasty with symptomatic psoas hematoma formation in a patient with multiple myeloma. There are few cases reported in the literature with regard to focal hematomas or lumbar artery pseudoaneurysm [6] following BKP procedures, but there is a paucity of published data with respect to the clinical and radiological pictures and their management and outcomes. Although hematoma complications remaina very rare complications before performing a percutaneous vertebroplasty, patients should be informed about this rare complication and the operating surgeon aware of this being a risk.
Clinical Message
A post-operative psoas hematoma is a rare complication after kyphoplasty, and the more common complications of cement extravasation and new fracture should be excluded first. To avoid this complication, one should commence by positioning the trocar on the transverse process before moving medially to the junction of the transverse process, pars and facet. This avoids any inadvertent injury to the artery of the pars or inadvertently passing deep to the intertransverse ligament.
References
1. Bouza C, López-Cuadrado T, Cediel P, Saz-Parkinson Z, Amate JM. Balloon kyphoplasty in malignant spinal fractures: A systematic review and meta-analysis. BMC Palliat Care 2009;8:12.
2. Filippiadis DK, Marcia S, Masala S, Deschamps F, Kelekis A. Percutaneous vertebroplasty and kyphoplasty: Current status, new developments and old controversies. Cardiovasc Intervent Radiol 2017;40:1815-23.
3. McArthur N, Kasperk C, Baier M, Tanner M, Gritzbach B, Schoierer O, et al1150 kyphoplasties over 7 years: Indications, techniques, and intraoperative complications. Orthopedics 2009;32:90.
4. Garcia-Maroto R, Garcia-Coiradas J, Milano G, Cebrian JL, Marco F, Lopez-Duran L. Safety and efficacy of kyphoplasty in the treatment of tumoral disease of the spine. Revista Española de Cirugía Ortopédica y Traumatología (English Edition) 2015;59:406-12.
5. Robinson Y, Tschöke SK, Stahel PF, Kayser R, Heyde CE. Complications and safety aspects of kyphoplasty for osteoporotic vertebral fractures: A prospective follow-up study in 102 consecutive patients. Patient Saf Surg 2008;2:2.
6. Puri AS, Colen RR, Reddy AS, Groff MW, DiNobile D, Killoran T, et al. Lumbar artery pseudoaneurysm after percutaneous vertebroplasty: A unique vascular complication. J Neurosurg Spine 2011;14:296-9.
7. Jeon CH, Chung NS, Lee JH, Lee HD. Life-threatening paraspinal muscle hematoma after percutaneous vertebroplasty. Indian J Orthop 2016;50:567-70.
8. Yaltirik K, Ashour AM, Reis CR, Özdoğan S, Atalay B. Vertebral augmentation by kyphoplasty and vertebroplasty: 8 years’ experience outcomes and complications. J Craniovertebr Junction Spine 2016;7:153-60.
9. Yaltırık CK, Özdoğan S, Atalay B. Thoracic epidural hematoma complicating vertebroplasty. Am J Case Rep 2017;18:1229-32.
10. Tropeano MP, La Pira B, Pescatori L, Piccirilli M. Vertebroplasty and delayed subdural cauda equina hematoma: Review of literature and case report. World J Clin Cases 2017;5:333-9.
11. Huber FX, McArthur N, Tanner M, Gritzbach B, Schoierer O, Rothfischer W, et al. Kyphoplasty for patients with multiple myeloma is a safe surgical procedure: Results from a large patient cohort. Clin Lymphoma Myeloma 2009;9:375-80.
12. Röllinghoff M, Siewe J, Zarghooni K, Sobottke R, Alparslan Y, Eysel P, et al. Effectiveness, security and height restoration on fresh compression fractures–a comparative prospective study of vertebroplasty and kyphoplasty. Minim Invasive Neurosurg 2009;52:233-7.
13. Grohs JG, Matzner M, Trieb K, Krepler P. Minimal invasive stabilization of osteoporotic vertebral fractures: A prospective nonrandomized comparison of vertebroplasty and balloon kyphoplasty. J Spinal Disord Tech 2005;18:238-42.
14. Movrin I, Vengust R, Komadina R. Adjacent vertebral fractures after percutaneous vertebral augmentation of osteoporotic vertebral compression fracture: A comparison of balloon kyphoplasty and vertebroplasty. Arch Orthop Trauma Surg 2010;130:1157-66.
15. Shi-Ming G, Wen-Juan L, Yun-Mei H, Yin-Sheng W, Mei-Ya H, Yan-Ping L, et al. Percutaneous vertebroplasty and percutaneous balloon kyphoplasty for osteoporotic vertebral compression fracture: Ametaanalysis. Indian J Orthop 2015;49:377-87.
16. Lee MJ, Dumonski M, Cahill P, Stanley T, Park D, Singh K, et al. Percutaneous treatment of vertebral compression fractures: A meta-analysis of complications. Spine (Phila PA 1976) 2009;34:1228-32.
17. Papanastassiou ID, Phillips FM, Van Meirhaeghe J, Berenson JR, Andersson GB, Chung G, et al. Comparing effects of kyphoplasty, vertebroplasty, and non-surgical management in a systematic review of randomized and non-randomized controlled studies. Eur Spine J 2012;21:1826-43.
 |
 |
 |
 |
| Dr. Valerio Pace | Dr. Dimpu Bhagawati | Dr. Chang Park | Dr. Sean Molloy |
| How to Cite This Article: Pace V, Bhagawati D, Park C, Molloy S. Delayed Presentation of a Symptomatic Psoas Hematoma Following Lumbar Vertebral Kyphoplasty for Myeloma: A Case Report. Journal of Orthopaedic Case Reports 2018 Nov-Dec; 8(6): 74-78. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 November 10, 2018 Devising Osteosynthesis for the Reverse Oblique Olecranon Fracture: A Case Report
November 10, 2018 Devising Osteosynthesis for the Reverse Oblique Olecranon Fracture: A Case Report January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty
January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty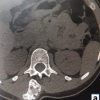 October 1, 2025 Pedunculated Exostosis of the Pedicle of Lumbar Vertebra: A Rare Cause of Lumbar Pain and Swelling
October 1, 2025 Pedunculated Exostosis of the Pedicle of Lumbar Vertebra: A Rare Cause of Lumbar Pain and Swelling October 1, 2025 Glomus Tumour of Sciatic Nerve – A Rare Presentation Mimicking Sciatica
October 1, 2025 Glomus Tumour of Sciatic Nerve – A Rare Presentation Mimicking Sciatica