
[box type=”bio”] Learning Point of the Article: [/box]
Insufficiency fractures in paraplegics can occur innocuously during physiotherapy sessions and due vigilance is a necessity in the rehabilitation, to prevent major repercussions.
Case Report | Volume 9 | Issue 2 | JOCR March – April 2019 | Page 26-29 | Prasoon Kumar, Sameer Aggarwal, Saurabh Agarwal, Karan Jindal. DOI: 10.13107/jocr.2250-0685.1354
Authors: Prasoon Kumar[1], Sameer Aggarwal[1], Saurabh Agarwal[1], Karan Jindal[1]
[1]Department of Orthopaedics, Post Graduate Institute of Medical Education and Research, Chandigarh, Punjab, India.
Address of Correspondence:
Dr. Karan Jindal,
Department of Orthopaedics, Post Graduate Institute of Medical Education and Research, Chandigarh – 160 012, Punjab, India.
E-mail: karan.121@hotmail.com
Abstract
Introduction: In paraplegic patients, chances of fragility fractures increase in view of disuse osteopenia. Theoretically, if a non-optimal force or torque is applied during passive manipulation or physiotherapy, fractures can occur in such patients. We present such a curious case of a pathological fracture of proximal femur wherein the patient heard a click during his daily routine of passive joint mobilization.
Case Report: A 31-years-old paraplegic male suffered a subtrochanteric femur fracture as an innocuous injury during his physiotherapy and range of motion (ROM) exercises. He had osteopenia that resulted in this fragility fracture. He was managed with an intramedullary nail, and medical management was done for osteopenia.
Conclusion: Fragility fractures can occur during passive ROM exercises that require vigilance on the part of the physiotherapists and attendants. Unnecessary forceful movements should be avoided.
Keywords: Femur fracture, Fragility fracture, Paraplegics, Physiotherapy exercises, Spinal cord injury.
Introduction
Motor weakness, especially of the lower limbs, associated with spinal cord injury (SCI) is associated with a decrease in bone mineral density, as a long-term complication due to disuse of the affected muscles [1]. This could be complicated by the incidence of fragility fractures in the weakened bones, that would be further detrimental for the rehabilitation of the paraplegics; these patients are vulnerable to such fractures even after subtle or no obvious trauma. After SCI, the bone loss in these patients is higher in the first 6 months and stabilises between 12 and 16 months, with about 30% loss of bone mass. Gradual bone loss further continues with 50% loss seen over 10 years [2]. The historical incidence of fractures in the population with SCI has been 1.45–6% , while the prevalence of fractures is reported to be 25–46% [3]. The sites of most severe osteoporosis are in the distal femur and the tibia followed by proximal femur and spine [4, 5]. In paraplegics, due to the higher requirement of passive intervention that they have, with regard to the mobility and participation in physical activities, chances of fragility fractures are obvious [6, 7, 8]. Physiotherapy and rehabilitation are of paramount importance in SCI patients with motor weakness. Continuous passive joint mobilization is crucial to prevent long-term muscular atrophy and contractures, as well as other immobilization-related complications, such as bed sores [7]. A standard protocol of such passive range of motion (ROM) exercises includes assistance from a trained physiotherapist or the patient’s attendants. Trivial falls or minor external impact is documented to be the causative factors of such fractures. In bedridden paraplegic patients with osteopenia, lesser torque is needed to produce failures in already weakened bone. Hence, theoretically if such a force is applied during passive manipulation or physiotherapy, fractures can occur. We present such a curious case of fragility proximal femur fracture in a paraplegic that occurred during his routine passive movements of knee and hip.
Case Report
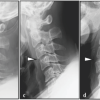
A 31-years-old paraplegic, male patient presented to the outpatient department of our institute with complaint of a sudden audible click from his right proximal thigh, during passive ROM exercises, as a part of his rehabilitation protocol. He had an alleged history of fall from height 2 years back, resulting in fracture of the first lumbar vertebra, with paraplegia. The patient was operated with pedicle screw fixation and posterior decompression (Fig. 1). 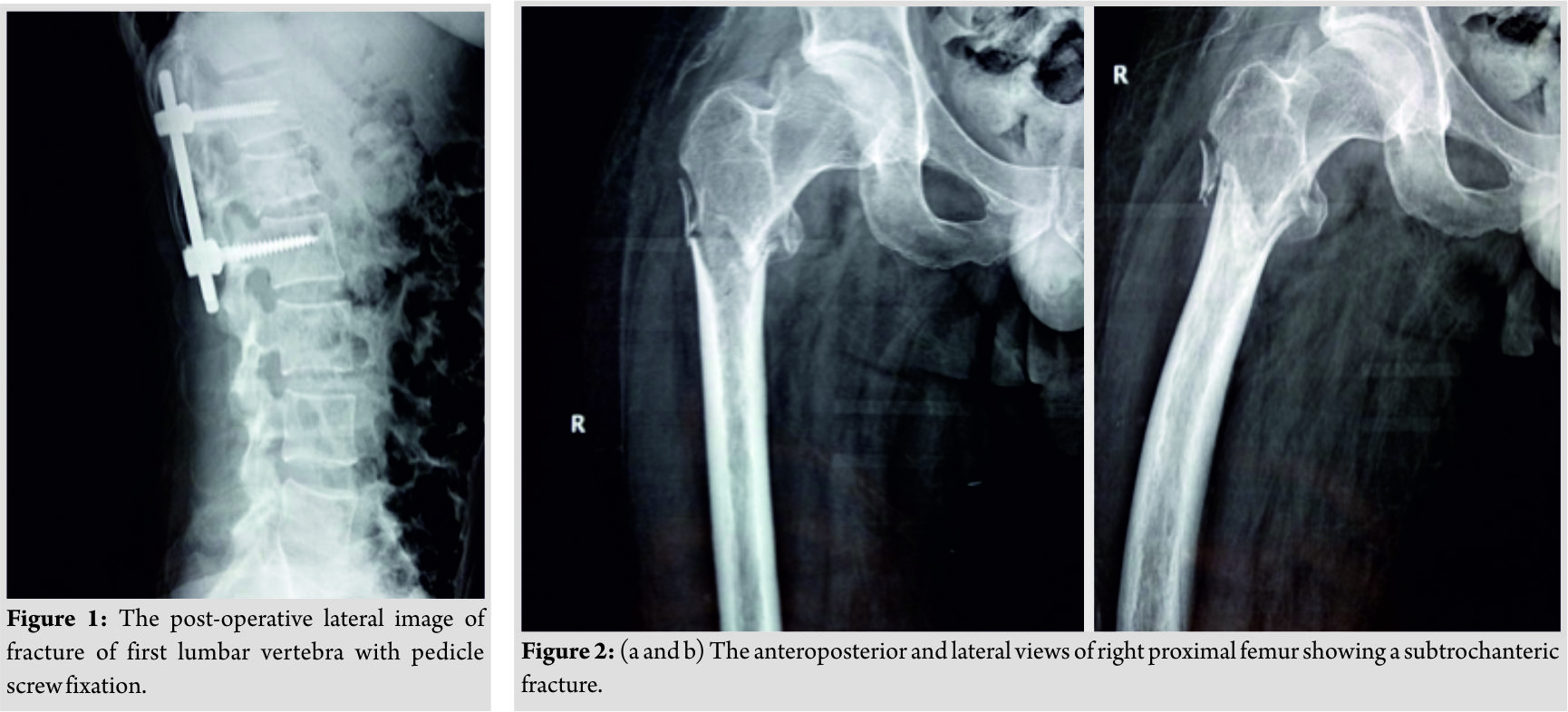 There was no improvement in the neurological status in the post-operative period, and the patient was on regular physiotherapy and rehabilitation. Plain radiology showed a fracture of the right subtrochanteric femur (Fig. 2). The patient biochemical profile was evaluated, which showed normal Vitamin D3 (23.79 ng/ml) and parathyroid hormone (PTH) levels (33.25 pg/ml). The dual-energy X-ray absorptiometry (DEXA) scan revealed osteopenia of the proximal femur (T score = −1.5). The patient was operated and closed proximal femur nailing was done to fix the fracture (Fig. 3). The patient had no intraoperative or post-operative complications. Early ROM exercises were initiated along with wheel chair mobilization. The patient was started on subcutaneous teriparatide with calcium and Vitamin D supplementation. At the last follow-up, he had supple joints and was kept under a home-based rehabilitation program.
There was no improvement in the neurological status in the post-operative period, and the patient was on regular physiotherapy and rehabilitation. Plain radiology showed a fracture of the right subtrochanteric femur (Fig. 2). The patient biochemical profile was evaluated, which showed normal Vitamin D3 (23.79 ng/ml) and parathyroid hormone (PTH) levels (33.25 pg/ml). The dual-energy X-ray absorptiometry (DEXA) scan revealed osteopenia of the proximal femur (T score = −1.5). The patient was operated and closed proximal femur nailing was done to fix the fracture (Fig. 3). The patient had no intraoperative or post-operative complications. Early ROM exercises were initiated along with wheel chair mobilization. The patient was started on subcutaneous teriparatide with calcium and Vitamin D supplementation. At the last follow-up, he had supple joints and was kept under a home-based rehabilitation program.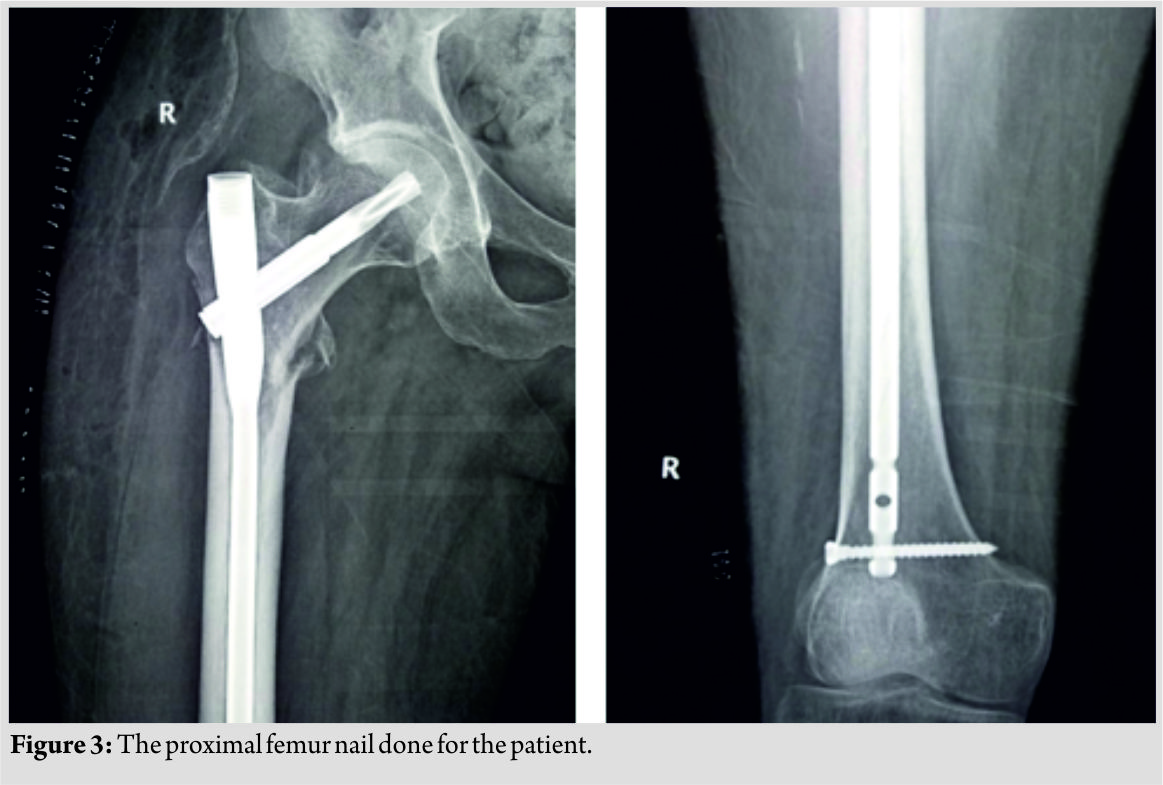
Discussion
Spinal cord injuries are associated with osteoporosis which renders a patient highly susceptible to fractures from minor trauma, that can occur during innocuous activities such as wheelchair mobilization or transfer to bed [1]. This bone loss occurs due to an increase in osteoclastic number and activity which enhances bone resorption. This increased activity is most commonly due to decreased physical activity, but other factors such as Vitamin D deficiency, altered calcium metabolism, smoking, genetics, and infections may play a role [9]. Lower limb fragility fractures are commonly encountered in these patients and vigilance is important on the part of the clinicians as well as attendants of these patients as they cannot give symptoms of pain or loss of function. Frotzler et al. reported a total of 156 such fractures in 107 patients of SCI, with femur fractures being the most common (60.9%) [10]. However, the peculiar and rare point regarding the present case was the mode of the fragility fracture. The patient developed a fracture during the course of his physiotherapy exercises. In SCI, physiotherapy is an essential component which prevents the formation of contractures, and there needs to be awareness of this rare complication. Torsional or twisting forces should not be applied and only the optimal force with soft grips should be used while dealing with these patients, who themselves need to be counselled regarding the subtle signs of such an injury. In our patient, it was him who picked up the audible click and could get early medical attention. One can suspect such fractures in cases of history of audible clicks, abundant callus in case of delayed presentation, or general signs such as an increase in spasticity or sweating [11]. These insufficiency fractures generally show an excellent healing response and were, thus, earlier managed conservatively in view of osteoporotic bones and high risk of complications [12]. However, similar complication rates have been shown with both conservative and surgical managements, and therefore, internal fixation is being routinely done nowadays, with intramedullary devices or plates with screws [9]. Operative treatment aids in initiating careful early ROM exercises to prevent joint contractures, which could be a cause of further disability in the paraplegics and a burden on their health-care providers [13]. Treatment of osteoporosis and prevention of fragility fractures in these patients require medical management. The commonly available modalities are calcium supplements, Vitamin D, bisphosphonates, and teriparatide which have been shown to improve the bone marrow density by 10% after therapy of 18 months by Hashimoto et al. [14]. It is a recombinant terminal peptide of the human PTH and has been shown to reduce the incidence of fragility fractures [14, 15]. The role of functional electrical stimulation has been recommended to increase bone strength, but its efficacy is largely unproven [16]. The present case is a peculiar one, solely due to the mode of the injury. A seemingly innocuous physiotherapy session led to a major long bone fracture and the fact that such a rare possibility does exist, makes this case an important learning point. Spinal cord injuries leading to osteoporosis, which, in turn, leading to fragility fractures, is a known phenomenon; however, the risk tends to be overlooked which could have disastrous repercussions for the patient, adding to his disability. Proper counselling regarding the time, force, and repetitions during the physiotherapy sessions must be given to the attendants to avoid any untoward incidences.
Conclusion
Paraplegia is commonly associated with osteoporosis and fractures can even occur with innocuous injuries such as force of passive ROM of the joints. Thus, the surgeon, physiotherapists and patients’ attendants should be aware of this complication and should never perform any forceful movements.
Clinical Message
Due vigilance on the part of health-care providers is a necessity in paraplegic rehabilitation where even minimal passive forces can have major repercussions.
References
1. NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA 2001;285:785-95.
2. Demirel G, Yilmaz H, Paker N, Onel S. Osteoporosis after spinal cord injury. Spinal Cord 1998;36:822-5.
3. Kiratli BJ, Perkash I, O’Mara G, Sims G. Fractures with chronic spinal cord injury: Epidemiology, morphology, and healing outcomes. J Bone Mineral Res 2001;16:S15.
4. Garland DE, Maric Z. Bone mineral density about the knee in spinal cord injured patients with pathologic fractures. Contemp Orthop 1993;26:375-9.
5. Garland DE, Adkins RH, Kushwaha V, Stewart C. Risk factors for osteoporosis at the knee in the spinal cord injury population. J Spinal Cord Med 2004;27:202-6.
6. Ziyad A, Badawi F, Vasile AT, Arzaga D, Cassedy A, Craven C. Dual diagnosis: Spinal cord injury and brain injury. In: Lin V, Diana D, editors. Spinal Cord Medicine: Principles and Practice. New York: Demos; 2003.
7. Charmetant C, Phaner V, Condemine A, Calmels P. Diagnosis and treatment of osteoporosis in spinal cord injury patients: A literature review. Ann Phys Rehabil Med 2010;53:655-68.
8. Fattal C, Mariano-Goulart D, Thomas E, Rouays-Mabit H, Verollet C, Maimoun L, et al. Osteoporosis in persons with spinal cord injury: The need for a targeted therapeutic education. Arch Phys Med Rehabil 2011;92:59-67.
9. NIH consensus development panel on osteoporosis prevention, diagnosis, and therapy, march 7-29, 2000: Highlights of the conference. South Med J 2001;94:569-73.
10. Frotzler A, Cheikh-Sarraf B, Pourtehrani M, Krebs J, Lippuner K. Long-bone fractures in persons with spinal cord injury. Spinal Cord 2015;53:701-4.
11. Keating J, Kerr M, Delargy M. Minimal trauma causing fractures in patients with spinal cord injury. Disabil Rehabil 1992;14:108-9.
12. Morse LR, Battaglino RA, Stolzmann KL, Hallett LD, Waddimba A, Gagnon D, et al. Osteoporotic fractures and hospitalization risk in chronic spinal cord injury. Osteoporos Int 2009;20:385-92.
13. Ragnarsson KT, Sell GH. Lower extremity fractures after spinal cord injury: A retrospective study. Arch Phys Med Rehabil 1981;62:418-23.
14. Hashimoto Y, Wakayama N, Miyauchi A. Therapeutic agents for disorders of bone and calcium metabolismteriparatide, parathyroid hormone (1-34) as a daily subcutaneous injection. Clin Calcium 2007;17:48-55.
15. Sethi BK, Chadha M, Modi KD, Kumar KM, Mehrotra R, Sriram U, et al. Efficacy of teriparatide in increasing bone mineral density in postmenopausal women with osteoporosisan Indian experience. J Assoc Physicians India 2008;56:418-24.
16. Hangartner TN, Rodgers MM, Glaser RM, Barre PS. Tibial bone density loss in spinal cord injured patients: Effects of FES exercise. J Rehabil Res Dev 1994;31:50-61.
 |
 |
 |
 |
| Dr. Prasoon Kumar | Dr. Sameer Aggarwal | Dr. Saurabh Agarwal | Dr. Karan Jindal |
| How to Cite This Article: Kumar P, Aggarwal S, Agarwal S, Jindal K. Fragility Fracture of Proximal Femur in a Paraplegic Patient during Passive Joint Movements. Journal of Orthopaedic Case Reports 2019 Mar-Apr; 9(2): 26-29. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Virtual reality rehabilitation to enhance functional recovery initiated from the acute phase following cervical cord injury: A case report
February 1, 2026 Virtual reality rehabilitation to enhance functional recovery initiated from the acute phase following cervical cord injury: A case report December 1, 2025 Management of a Case of Adult Mid-Shaft Femur Fracture in Osteogenesis Imperfecta by Long Proximal Femoral Nail: A Case report
December 1, 2025 Management of a Case of Adult Mid-Shaft Femur Fracture in Osteogenesis Imperfecta by Long Proximal Femoral Nail: A Case report September 1, 2025 Treatment of Bilateral Distal Femoral Shaft Fractures in a Paraplegic Patient with Intramedullary Nailing: A Case Report
September 1, 2025 Treatment of Bilateral Distal Femoral Shaft Fractures in a Paraplegic Patient with Intramedullary Nailing: A Case Report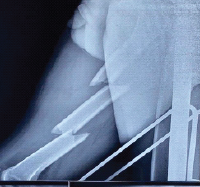 September 1, 2025 Innovative Management of Double Segmental Femur Fracture without Fracture Table: A Case Report
September 1, 2025 Innovative Management of Double Segmental Femur Fracture without Fracture Table: A Case Report