
[box type=”bio”] Learning Point of the Article: [/box]
This article will demonstrate the biomechanics of stress fractures due to implant stress shielding.
Case Report | Volume 9 | Issue 2 | JOCR March – April 2019 | Page 3-6 | David N Kugelman, Victor H Frankel, Arthur Baker, Kenneth Egol. DOI: 10.13107/jocr.2250-0685.1342
Authors: David N Kugelman[1], Victor H Frankel[1], Arthur Baker[1], Kenneth Egol[1]
[1]Department of Orthopaedics, NYULMC Hospital for Joint Diseases, New York, United States.
Address of Correspondence:
Dr. David N Kugelman,
B.S 301 E 17th Street, New York, NY 10003.
E-mail: Dkugelman@tcmc.edu
Abstract
Introduction: Non-traumatic stress fractures of the humerus are often related to a throwing motion. This type of humeral fracture is often due to uncoordinated muscular activity on the humeral shaft. These forces over time may contribute to mid-shaft humeral stress fractures, an injury often referred to as a “throwers fracture.” The ultimate strength of bone is decreased when a screw hole is created, as in open reduction and internal fixation repairs (ORIF).
Case Report: This case study discusses a patient who underwent plate and screw fixation of a previous stress fracture of the humerus. He continued to remain active and competitive in collegiate baseball, playing the catcher position which leads to a recurrent stress fracture. A combination of low Vitamin D and stress-shielded bone likely resulted in the reinjury. Physicians treating patients with these injuries should be aware of the possibility of refracture if inciting factors are not modified. This case of a non-traumatic humeral shaft stress refracture, following ORIF, has not been described in the literature.
Conclusion: The unusual case of a humeral stress refracture following ORIF is presented. A combination of low Vitamin D and stress-shielded bone likely resulted in the reinjury. Physicians treating patients with these injuries should be aware of the possibility of refracture if inciting factors are not modified.
Keywords: Humerus stress fracture, plate and screw biomechanics, thrower’s fracture.
Introduction
The majority of humeral shaft fractures occur following a traumatic incident. Humeral shaft fractures are a common injury that represents 3–5% of all fractures. Non-traumatic stress fractures of the humerus, while an uncommon event, have been described in literature. These are often related to a throwing motion, especially in the competitive thrower [1, 2]. This type of humeral fracture is often due to uncoordinated muscular activity on the humeral shaft [1, 2]. First described in 1905 by Ashhurst [1], these injuries occur most commonly in men who are in their third decade of life. During the act of throwing, kinematic changes occur at the shoulder and elbow, which in effect leads to torsional forcesacting on the humerus [3]. These forces over time may, therefore, contribute to mid-shaft humeral stress fractures, often referred to as a “throwers fracture.” Stress fractures are secondary to the concentration of repeated stress, external forces, and chronic rapid effects of muscle contraction on bone [4]. The ultimate strength of bone is decreased when a screw hole is created, a phenomenon that occurs following open reduction and internal fixation (ORIF) repairs. Screw holes concentrate the stress of bending and torsional loading on bone, which, therefore, makes the bone weaker [5, 6]. It has been demonstrated that a defect in the bony tubular structure may lead to a decreased strength necessary for a break due to a bending force [5].
Case Report
A 20-year-old male athlete who had been complaining of a dull achy pain in his right deltoid region sustained a displaced closed right humeral shaft fracture following a throw in a baseball game (Fig. 1). He was seen at a local hospital after the injury and was placed in a coaptation splint. On initial examination, gross motor and sensation were intact. To rule out malignancy, an magnetic resonance imaging was obtained which did not demonstrate any pathological lesions. In an effort to speed recovery and maintain maximal function, he underwent ORIF. An anterolateral approach to the humerus was made, and the fracture was reduced and compressed using a large fragment plate and screw construct (Fig. 2).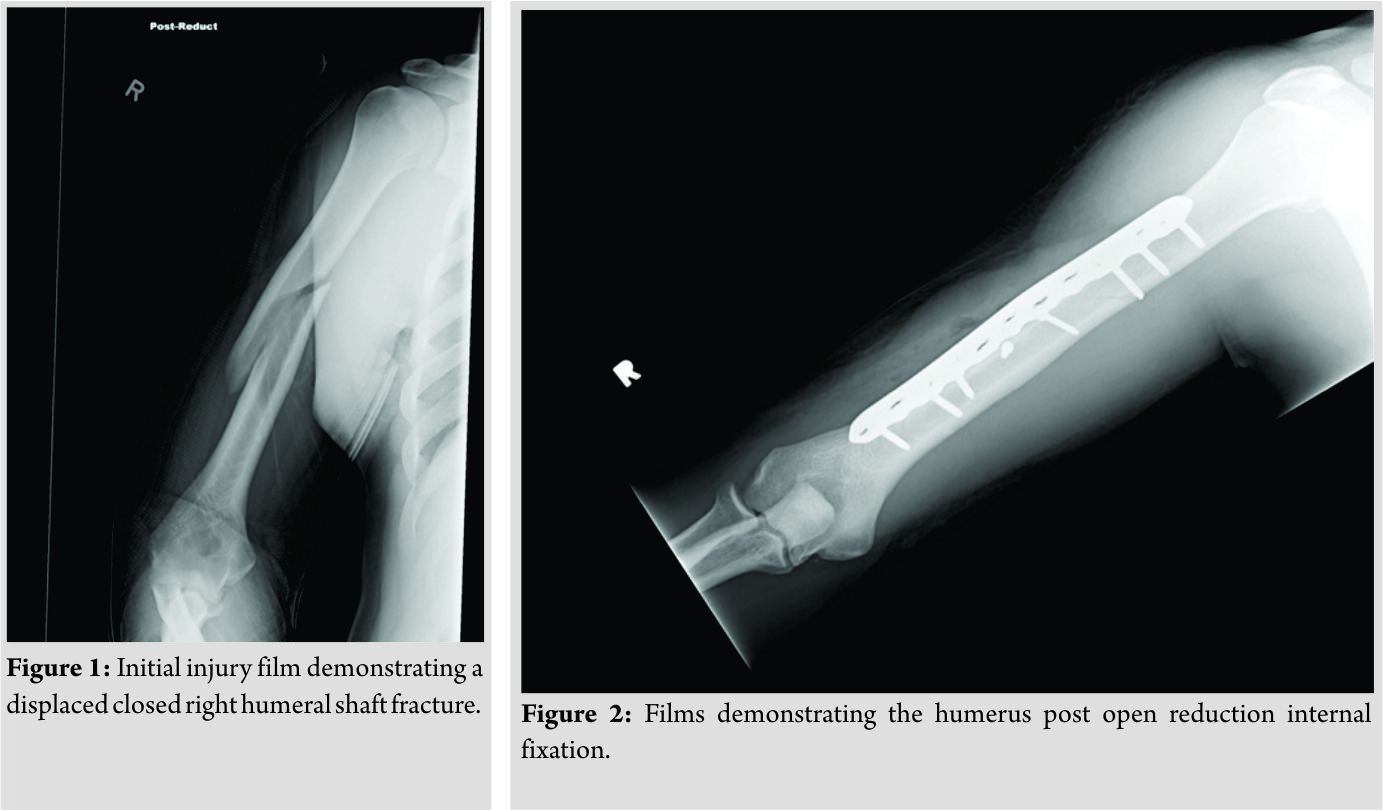
Six weeks following the surgery, the patient began to jog and lightly throw a baseball. He began light weight lifting and continued home PT to strengthen the elbow and shoulder. By 3 months’ post-operative, the fracture had united. The patient returned to college baseball 6 months postoperatively. Eleven months following the fracture repair and 5 months following return to baseball, the patient felt a “pop” with immediate pain in the posterolateral aspect of his right arm following a throw. Radiographs of the right humerus revealed two new fracture lines. A computed tomography scan confirmed anew spiral fracture of the midshaft of the humerus extending from the second proximal screw to the lag screw. The hardware remains intact, and there is no evidence of hardware failure or loosening (Fig. 3). Vitamin D levels were obtained and were found to be low. The patient’s 25-OH Vitamin D level was found to be 24.3 ng/mL, while the reference range was 32.0–100.0 ng/mL. His serum calcium was within normal limits, at 9.5 ng/mL. In addition, a thyroid function panel was within normal limits. The thyroid panel was obtained, to rule out hyperthyroidism, as this can lead to secondary osteoporosis. The patient was, therefore, started on Vitamin D, given a one-time dose of 50,000 U followed by 2000 U daily. The patient was placed in a sling, for 1 month, following refracture. The patient began physical therapy 3 weeks following the refracture. Initial therapy consisted of numerous stretching activities in addition to using resistance bands for shoulder and elbow range of motion exercises. Throughout the recovery process, he attended therapy 3 times a week. The patient had full shoulder and elbow range of motion at 4 weeks’post-refracture. At 3 months’post-reinjury, the fracture appeared to be healed (Fig. 4). He was cleared for light sporting activities at 3-month post-reinjury. At this time point, the patient began throwing exercises at this time with the collegiate baseball athletic trainer. He began performing four sets of 10 throws, from a distance of 60 feet. The intensity of throwing at this time was 50% of full strength. He performed throwing exercises 3 days a week. After 2 weeks of these throwing exercises, he began six sets of 10 throws with each set having an increase of intensity by 5–10%, where he had perform his last set at 85% of maximum throwing strength. 2 weeks into his therapy, he also began to perform the following weight training, in three sets of 10 repetitions: Seated rows, lat pull downs, and tricep extensions. The patient continued to exercise and work with the college’s athletic trainer. After 3 months of working with physical therapy and the collegiate athletic trainer and at 6 months following re-injury, he was back to throwing at 100% intensity. He gradually increased throwing distance and weight training over 4 months of therapy. He continues to take 2000 U of Vitamin D3, once a day. Today, he is 1 year out from the recurrent stress fracture and is throwing a baseball at 145 feet with original pre-injury intensity. He finished his senior year of college back on the baseball field, as his teams start catcher. Imaging of his humerus at 1 year post-recurrent stress fracture is demonstrated in (Fig. 5).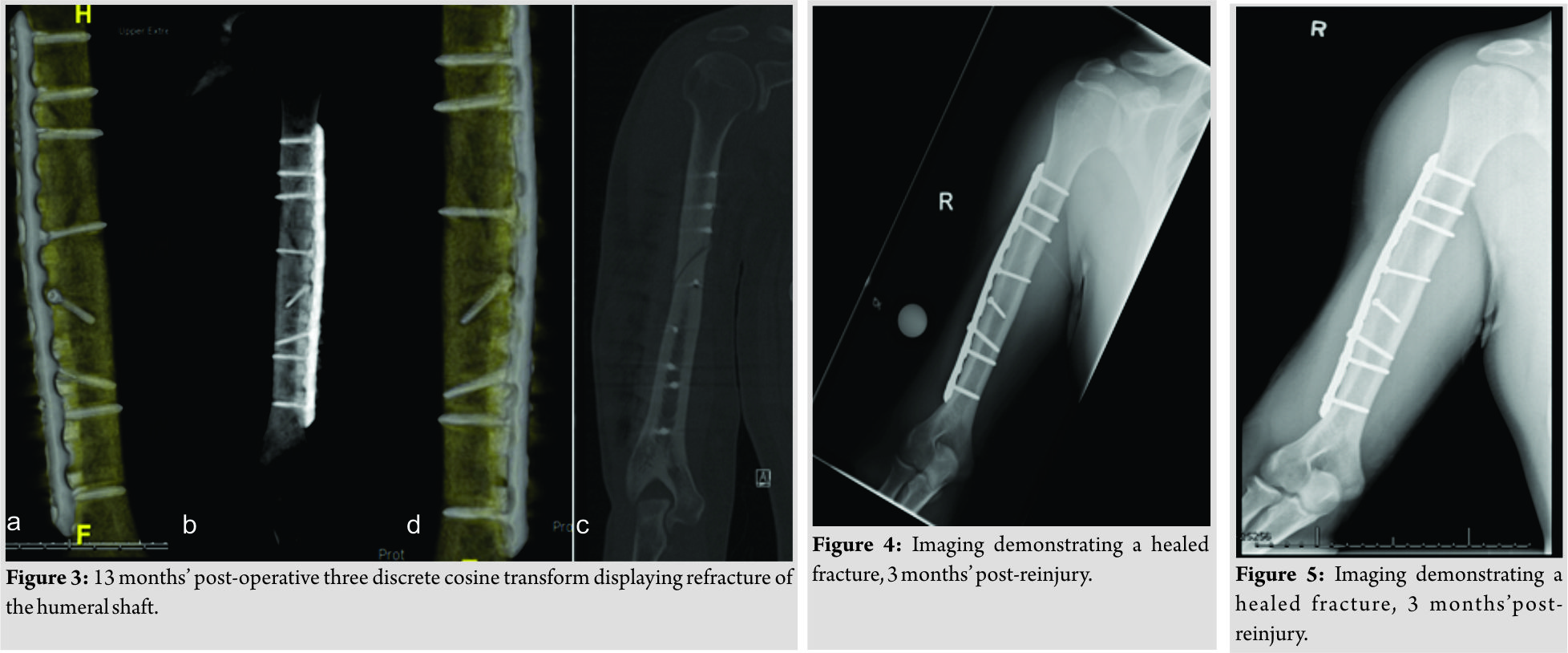
Discussion
The humeral diaphysis is the region between the proximal insertion of the pectoralis major and the distal metaphyseal flare of the humerus. It takes on a cylindrical shape, which contributes to humeral shaft strength and resistance to torsional and bending forces. The humeral shaft strength is still constantly tested due to forces generated by the insertion and origination of muscles on the shaft [2, 3, 7]. The inserting muscles consist of the deltoid, pectoralis major, teres major, latissimus dorsi, and coracobrachialis muscles. The originating muscles of the humeral shaft are the brachialis, brachioradialis, and triceps brachii medial and lateral heads. Humeral shaft strength is tested in throwing athletes such as baseball players [1, 3, 7]. When throwing an object, the midshaft of the humerus undergoes torsional forces due to pull of the deltoid insertion. The greater tuberosity experiences these forces due to the rotator cuff as well. These muscles act to abduct and externally rotate the humerus. When the external rotation ceases and internal rotation takes place, the flexion of the elbow now undergoes elbow extension, in which torsional force on the humerus is at a maximum. This is often the point at which these fractures occur. The most common site of fracture is below the insertion of the deltoid muscle at the middle to lower third of the humerus or along the radial groove [3]. Following the external rotation, internal rotation of the humerus takes place in which the pectoralis major and coracobrachialis insert into the medial aspect of the humerus [3]. In the acceleration phase of the throwing motion, the angular velocity of shoulder internal rotation occurs at 6000°/s. At the same time of the shoulder’s acceleration, the elbow is extended and undergoes an angular velocity of 4600°/s. The internal rotation of the shoulder that occurs in the throw generates a rotation torque of approximately 14,000 inch-pounds [8]. Every throw and pitch by competitive athletes, therefore, culminate in large stresses on the humerus. Due to the torsional forces applied to the humeral shaft by the insertions and origins of muscles involved in the throwing sequence, these midshaft “thrower’s fractures” are prone to occurrence [1, 2, 8]. When discussing biomechanical considerations, strength is derived from load capacity and energy storage capacity, while rigidity is a measurement of resistance to deformation under a stressor. Rigidity is a ratio of the applied torque and angular deformation of bone from a stressor. The maximum amount of torque, which may be applied axially to a bone before fracture occurs, is torsional bone velocity [9]. The humeral torque during a throw causes the distal end of the humerus to be externally rotated relative to the proximal end. This rotation is in accordance with the external rotation spiral fracture mechanism discussed previously [8, 9, 10]. The patient described in this report most likely had decreased humeral bone strength. There are multiple factors that contribute to an alteration in bone strength following a fracture and treatment using plates and screws. The size of the screw or defect does not play a role in this strength reduction. In addition, the presence of a plate will further reduce the bone strength as well [6]. Geometry and material properties of a plate attached to bone influence the load sharing of each structure. A plate may bear increased loads, which cause bone to atrophy in response to its role of carrying a decreased load. This leads to a decreased diaphysis diameter, which reduces the area and polar moment of inertia, therefore reducing bone strength. A 60% decrease in strength to torsion has been demonstrated to occur in as little as a 20% decrease in bone diameter. This decrease in bone size is usually followed by a secondary osteoporosis, which even further decreases bone strength [11]. Screw holes concentrate stress, which in turn makes bone weaker during bending and torsional loading [5, 6, 12]. Following ORIF, bone may produce a buttress against the screw, which will transmit compressive and small shear stress across the screw. Tensile and larger shear stresses will not be transmitted through the screw, which then leads to the concentration of stress around the screw [5]. Tensile stresses act perpendicular to the axis of the screw hole. The maximum stress on bone occurs at a 45 degree angle, and this maximum stress becomes 25% of the original bone when a screw hole is present [5]. An increased elasticity is present in screws over bone, resulting in possible displacements of bone. This displacement creates a space along with tangential displacements of the bone relative to the screw interface. This study also compared screw holes alone versus screw holes with the screws retained in the femurs of dogs. After 8 weeks post-operation, the maximum torque and energy absorption displayed no difference between the two groups. There was no drop in strength correlation with time after operation [5]. Screw hole defects are likely due to the screw’s ability to increase stress and weaken bone’s tensile strength when undergoing torsional loading. Another factor affecting the patient with regard to stress fracture risk was his low Vitamin D level. Bone mineral content plays an important role in its structure [13]. Vitamin D deficiency has been demonstrated to reduce bone mineral content and strength in studies on rats [14] The decreased levels of Vitamin D have demonstrated a 2%reduction in torsional strength when using the rat femur as a model [14]. The patient reported on may have, therefore, had a lower set point in the amount of force and repetition needed to sustain a throwers’ fracture due to his decreased Vitamin D levels. Conservative management proved effective following this patient’s recurrent stress fracture. Physical therapy and gradual increase in throwing were undertaken, with full recovery and return to sport at 6-month follow-up.
Conclusion
This case of non-traumatic humeral stress refracture following ORIF has not been described in the literature. The unusual case of humeral stress refracture following ORIF is presented. A combination of low Vitamin D and stress-shielded bone likely resulted in the reinjury. Physicians treating patients with these injuries should be aware of the possibility of refracture if inciting factors are not modified.
Clinical Message
Following ORIF for a humeral shaft fracture, patients are at increased risk for injury due to decreased bone strength due to implant stress shielding, followed by repetitive stress from the throwing motion. These individuals should be closely monitored and undergo a gradual return to participation in athletics. In addition, Vitamin D levels should be obtained in active individuals who suffer from stress fractures, as decreased bone mineralization can contribute to an increased likelihood of fracture.
References
1. Ashhurst AP. Fractures of the humerus by muscular violence. Univ Pa Med Bull 17:336-9, 1905-6.
2. Wilmoth CL. Recurrent fracture of the humerus due to sudden extreme muscular action. J Bone Joint Surg 1930;12:168-9.
3. Tullos HS, King JW. Throwing mechanism in sports. Orthop Clin North Am 1973;4:709-20.
4. Brukner P. Stress fractures of the upper limb. Sports Med 1998;26:415-24.
5. Burstein AH, Currey J, Frankel VH, Heiple KG, Lunseth P, Vessely JC, et al. Bone strength. The effect of screw holes. J Bone Joint Surg Am 1972;54:1143-56.
6. Orville B, Ferguson AB, Laing PG. Metals and Engineering in Bone and Joint Surgery. Baltimore: Williams and Wilkins; 1959. p. 303.
7. DiCicco JD, Mehlman CT, Urse JS. Fracture of the shaft of the humerus secondary to muscular violence. J Orthop Trauma 1993;7:90-3.
8. Ogawa K, Yoshida A. Throwing fracture of the humeral shaft. An analysis of 90 patients. Am J Sports Med 1998;26:242-6.
9. Alan MN, Melvin JW, editors. Accidental Injury: Biomechanics and Prevention. New York: Springer Science and Business Media; 2012.
10. Chao SL, Miller M, Teng SW. A mechanism of spiral fracture of the humerus: A report of 129 cases following the throwing of hand grenades. J Trauma 1971;11:602-5.
11. Slätis P, Paavolainen P, Karaharju E, Holmström T. Structural and biomechanical changes in bone after rigid plate fixation. Can J Surg 1980;23:247-50.
12. Chrisman OD, Snook GA. The problem of refracture of the tibia. Clin Orthop Relat Res 1968;60:217-9.
13. Burstein AH, Zika JM, Heiple KG, Klein L. Contribution of collagen and mineral to the elastic-plastic properties of bone. J Bone Joint Surg Am 1975;57:956-61.
14. Einhorn TA, Bonnarens F, Burstein AH. The contributions of dietary protein and mineral to the healing of experimental fractures. A biomechanical study. J Bone Joint Surg Am 1986;68:1389-95.
 |
 |
 |
 |
 |
| Dr. David N Kugelman | Dr. Victor H Frankel | Mr. Arthur Baker | Dr. Stuart Hershon | Dr. Kenneth Egol |
| How to Cite This Article: Kugelman DN, Frankel VH, Baker A, Egol K. A Recurrent Stress Fracture of the Humerus following Fixation: The Effect of Implant Stress Shielding. Journal of Orthopaedic Case Reports 2019 Mar-Apr; 9(2): 3-6. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 April 10, 2024 Reviewers Acknowledgement & Photo Gallery April 2024
April 10, 2024 Reviewers Acknowledgement & Photo Gallery April 2024 November 8, 2018 Paratesticular Paraganglioma with Metastasis to D1 Vertebra- A Case Report and Review of Literature
November 8, 2018 Paratesticular Paraganglioma with Metastasis to D1 Vertebra- A Case Report and Review of Literature May 10, 2021 Sacral Chordoma with Bilateral Inguinal Lymph Node Metastasis and Metachronous Tumor of the Clivus: A Case Report
May 10, 2021 Sacral Chordoma with Bilateral Inguinal Lymph Node Metastasis and Metachronous Tumor of the Clivus: A Case Report December 10, 2022 A Rare Case of Burkholderia Osteomyelitis Affecting the Hip Joint in an Adult
December 10, 2022 A Rare Case of Burkholderia Osteomyelitis Affecting the Hip Joint in an Adult