
[box type=”bio”] Learning Point of the Article: [/box]
Both high and low frequency TENS therapy are proven to be effective in symptomatic relieve of knee osteoarthritis, the choice depends on the severity of symptom, patient’s expectation and patient’s ability to withstand the therapy.
Case Report | Volume 10 | Issue 3 | JOCR May – June 2020 | Page 108-113 | Charles Ang Poh Thean, Mohd Shukrimi Bin Awang, Zamzuri Bin Zakaria, Ardilla Hanim Binti Abdul Razak. DOI: 10.13107/jocr.2020.v10.i03.1772
Authors: Charles Ang Poh Thean[1], Mohd Shukrimi Bin Awang[1], Zamzuri Bin Zakaria[1], Ardilla Hanim Binti Abdul Razak[1]
[1]Department of Orthopaedics, International Islamic University Malaysia Medical Centre, Jalan Sultan Ahmad Shah, 25200 Kuantan, Pahang, Malaysia.
Address of Correspondence:
Dr. Charles Ang Poh Thean,
Department of Orthopaedics, International Islamic University Malaysia Medical Centre, Jalan Sultan Ahmad Shah, 25200 Kuantan, Pahang, Malaysia.
E-mail: capt85@hotmail.my
Abstract
Introduction: The prevalence of knee osteoarthritis is on the raise. This raise has been a huge financial burden to developed countries in treating the disease. Transcutaneous electrical nerve stimulation (TENS) is a cost-effective, easily available, and self-applicable mode of non-pharmacological pain relieve technique. Despite these advantages, the use, settings, and effectiveness of portable TENS are still poorly understood. The aim of this study is to determine the effectiveness of portable TENS at different frequencies in treating knee osteoarthritis.
Materials and Methods: This is a single-center quasi-experimental study involving 100 patients seen in the outpatient department with knee osteoarthritis. They were randomly (computer generated) allocated into two arms (high frequency [H-F] or low frequency [L-F]). H-F is set at 100 Hz and L-F is set at 4 Hz. A baseline assessment is taken with the visual analog score (VAS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Oxford Knee Score, and Lequesne index. They were instructed to self-administer the TENS therapy as per protocol and followed up at the 4th and 12th week to be reevaluated on the above scores.
Results: The final results show that both H-F and L-F groups showed improvement in all parameters of the VAS, WOMAC index, Oxford Knee Score, and Lequesne index (73%). Only the pain component of Lequesne index, activities of daily living component of Lequesne index, total Lequesne index, and pain component of WOMAC index shows a statistically significant difference, favoring the H-F group. The H-F group yields a faster result; however, with time the overall effect remains the same in both groups.
Conclusion: Both H-F and L-F groups show improvement in all the component of Lequesne index, Oxford Knee Score, WOMAC index, and VAS with no statistical difference between the two groups. Although H-F yields a faster result, not everyone is able to tolerate the intensity. Therefore, the selection of H-F or L-F should be done on case basis depending on the severity of symptoms, patient’s expectation, and patient’s ability to withstand the treatment therapy. Based on this 12th week follow-up, both groups will continue to improve with time. A longer study should be conducted to see it this improvement will eventually plateau off or continue to improve until the patient is symptom free.
Keywords: Knee osteoarthritis, non-pharmacological pain relieve, OA, pain management, TENS, transcutaneous electrical nerve stimulation therapy.
Introduction
The purpose of this study is to compare at which frequency of portable transcutaneous electrical nerve stimulation (TENS) is the optimal frequency for the treatment of knee osteoarthritis. The two said frequencies are high frequency (H-F) – 100 Hz and low frequency (L-F) – 4 Hz. The reason why this study was selected is because there are insufficient data regarding the effectiveness of TENS therapy at different frequencies clinically. Theoretically, it is known that TENS at different frequencies works through different mechanisms of pain control; however, clinically, this information is still very scanty. H-F TENS is believed to work through the pain gate theory, providing only short-term relieve [1, 2]. L-F, on the other hand, is believed to work through release of endorphins, giving a more systemic and long-term response [3]. However, some studies have demonstrated that H-F TENS has a longer-lasting effect than L-F TENS [4]. In 1998, Sluka et al. proved that the effect of L-F TENS is reversed by spinal administration of low-dose naloxone (selective for m-opioid receptors). H-F TENS antihyperalgesia effect, on the other hand, is prevented by blockade of d-opioid receptors in the spinal cord. Therefore, it is concluded that L-F TENS works through activation of m-opioid receptors and H-F TENS works through the activation of d-opioid receptors [5].
Law and Cheing in 2004 concluded that after 2 weeks of repeated TENS therapy at L-F, H-F, and alternating L-F and H-F, all significantly reduce OA knee pain. This pain reduction occurred in a cumulative manner from day 1 to day 10 and the analgesic effects produced by the 10th day were able to last for up to 2 weeks [6]. He also states that the pain-limited range of knee motion is significantly improved in both groups [6]. Carol et al. stated that both H-F and L-F TENS reduce primary hyperalgesia, but only H-F TENS reduces secondary hyperalgesia in OA patients [7].
Chen et al. observed that TENS is more effective than intra-articular HA injection, judged based on the improvement of visual analog score (VAS) at 2 weeks follow-up and the Lequesne index at 2 weeks and 3 months follow-up [8]. Cherian et al., in 2014, concluded that the use of TENS shown positive results on improvement of pain, subjective and objective functional outcomes, and the quality of life in knee OA patients. He went on to attribute his findings to the ability of TENS to be worn throughout most activity of daily living without/with minimal disruption [9]. In 2016, he drawn a few more conclusion based on two studies stating that patients on TENS showed improvement in all outcome measures, the VAS score, new knee society scale functional scores, lower extremity functional scale, and short form-36 had an overall lower decline in quadriceps and hamstring strength, decrease in consumption of analgesia, and finally fewer patients eventually progressed to total knee arthroplasty [10]. Law et al. and several other authors suggest that 40 min is the optimal treatment duration to relief OA knee pain [11, 12]. Manuela et al. suggested that constant increase of pulse amplitude activates a larger number of large-diameter afferent nerves, maintaining the action of inhibitory interneurons in the dorsal horn longer, thereby prolonging the analgesic effect [13].
To the author’s knowledge, there is no article found that shows comparison between this two frequencies in Malaysian population. Furthermore, the conclusions from the previous studies in other countries were focused on other parameters such as the duration of therapy per session and the effectiveness at different pulse amplitude. None compared the H-F against the L-F.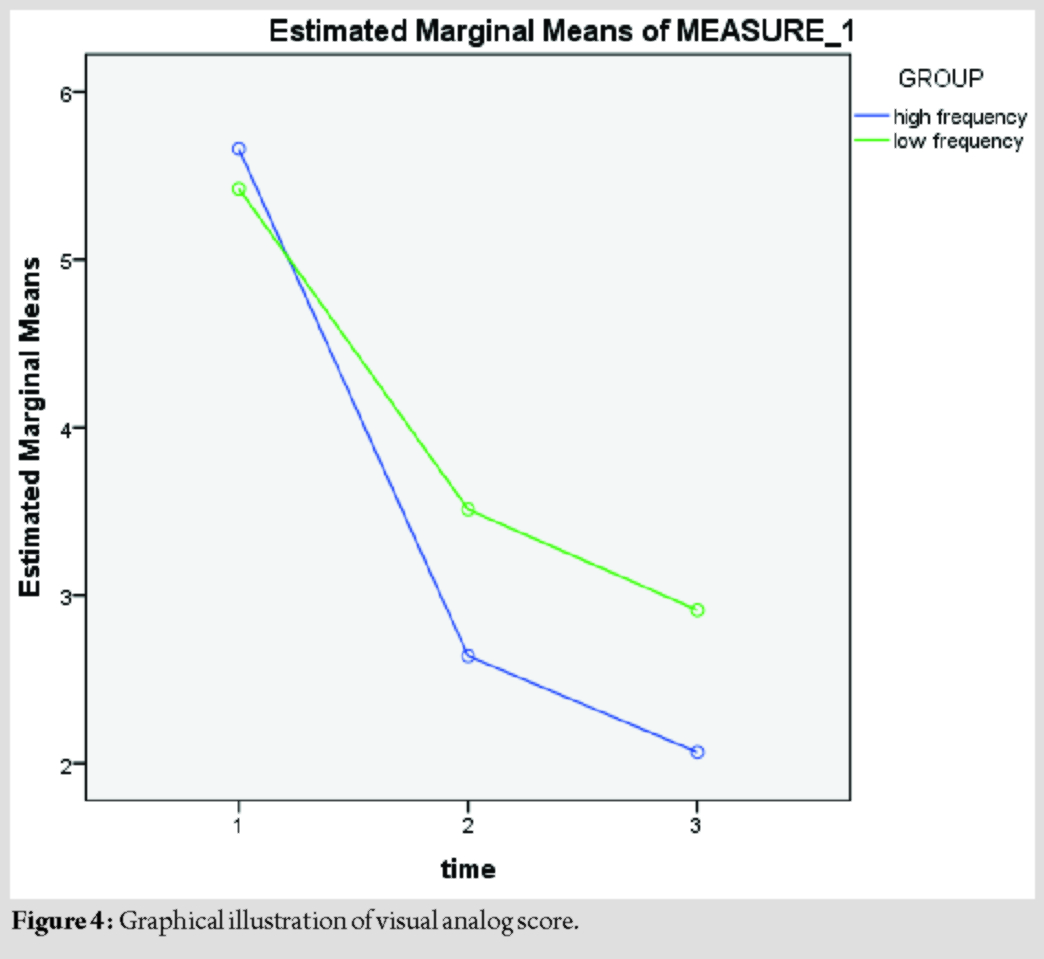
Materials and Methods
This is a single-center quasi-experimental study involving 100 patients seen in the outpatient department with knee osteoarthritis (based on Kellgren and Lawrence Grade II to IV) that willingly participate and consented. They were randomly (computer generated) allocated to the two arms (L-F or H-F). These patients were evaluated (baseline assessment) with the VAS, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Oxford Knee Score, and the Lequesne index. They were then followed up at the 4th and 12th week to be re-evaluated on the above scores. Participants were advised to use the device at least once daily regardless of symptoms (with a minimum requirement of at least 5 times per week). TENS model Well-Life (WL-2103A) is used for this study. It is validated and has been sold in the Malaysian market for over 2 years. The primary investigator helped the subjects to identify the area of maximal tenderness and placed the electrodes at four corners 4 cm away from the site of maximum tenderness (interferential current concept). Subjects were then encouraged to take a picture of the site of placement for their future references. A pictorial diagram was also provided to patients to guide them on the sites of electrode placement. Subjects should clean and dry the skin over the area of electrode placement with a dry cloth each time before use. Shaving or trimming of hair around the area is not necessary. The TENS machine settings are fixed to strength of six, continuous mode, and frequency according to group (L-F or H-F). The device is to be used 40 min each time with increasing pulse amplitude, beginning with 100 µs, and increasing by 50 µs every 10 min to a maximum of 250 µs as recommended by Manuela et al. [13]. Should the subject experiences acute exacerbation of symptoms, they are encouraged to use the device each time they have the exacerbation (up to 2 consecutive times per exacerbation). If pain is still not relieved, subjects are then encouraged to take the rescue drug (oral/intramuscular or intravenous tramadol). Subjects were then allowed to continue or withdraw from the study after informing the primary investigator. A maximum of 5 times per 24 h is recommended. Once exceeding the maximum amount to times allowed, subjects were encouraged to take the rescue drug. The number of times used per day is not fixed as different individuals have different amount of times of symptoms relapse. More relapse, use the device more. There is no fixed time of the day to use the device; however, subjects are encouraged to use it at the same time of the day according to their schedule. Example: If the subject is usually free during lunch hours 1300 h–1400 h, then the subject is encouraged to use it daily during that hour. Subjects were encouraged to use the device as rescue procedure in the event of acute exacerbation of symptoms at the frequency to which group they belonged to. Example: The HF group will use HF as their rescue procedure and the LF group will use LF as their rescue procedure. All subjects were provided with a patient diary to monitor compliance. The inclusion criteria were as follows: (I) Knee pain plus any three of the following; over 50 years of age, <30 min of morning stiffness, crepitus on active motion, bony tenderness, bony enlargement (joint appears bigger than normal side due to osteophytes), and no palpable warmth of synovium. (II) Plain radiograph Kellgren and Lawrence Grade II to Grade IV. (III) Not on any oral or topical analgesics for the knee osteoarthritis, besides the allowed rescue drug (if exposed, a washout period of 2 weeks is observed). The exclusion criteria were as follows: (I) Individuals undergone HA or steroid intra-articular injections before, (II) individuals with rheumatoid or gouty arthritis, (III) individuals undergone knee surgery before, (IV) individuals having cardiac pacemaker, and (V) individuals receiving TENS in the past 1 month. Sample size estimation was calculated using two population proportions formula (Lemeshow et al., 1990). Prior data indicate that the proportion of effective TENS of the high-intensity TENS group was 0.598 and the proportion of low-intensity TENS group was 0.279. Thus, a minimum sample size of 37 samples per group to be able to reject the null hypothesis with probability (power) 0.8. The Type I error probability associated with this test of this null hypothesis is 0.05. The Pearson’s Chi-square test for independence will be used to evaluate this null hypothesis. With an additional of 20% dropout rate, the sample size is 47 samples per group. The raw data were collected and processed accordingly. The collected data were recorded and analyzed using the Statistical Package for the Social Sciences® version 22.0 software. Demographic characteristic was analyzed descriptively. Independent t-test is used for analysis of NSA difference in both groups while Pearson’s Chi-square test is used to analysis the functional score and significance in pain outcome. The VAS, OKS, WOMAC, and Lequesne index were used to assess the functional outcome and marks are given based on the participants feedback. The statistical analysis was done using independent t-test. P < 0.05 is considered statistically significant. The principal investigator in this study has obtained the good clinical practice certificate by National Committee for Clinical Research, Ministry of Health (MOH), Malaysia. Investigator has also obtained ethical approval from the National Medical Research and Ethics Committee (MREC) of the MOH, Malaysia, through the National Medical Research Registry (NMRR). The approval from MREC and NMRR is obtained, and the investigator has also acquired approval from IIUM Research Ethics Committee. All responses are confidential, documents are kept in locked locker, and respondents are allowed to refuse to participate in the study at any time if they are not keen.
Results
Out of the 100 participants, eight were dropped out of the study for not adhering to the criteria, three from the H-F group, and five from the L-F group. Two from the H-F group reported that they were unable to tolerate the H-F and requested to drop out of the study. One reported no improvement thereby defaulted the follow-up. All five from the L-F group reported no improvement and two eventually undergone total knee replacement. The remaining three defaulted follow-up.
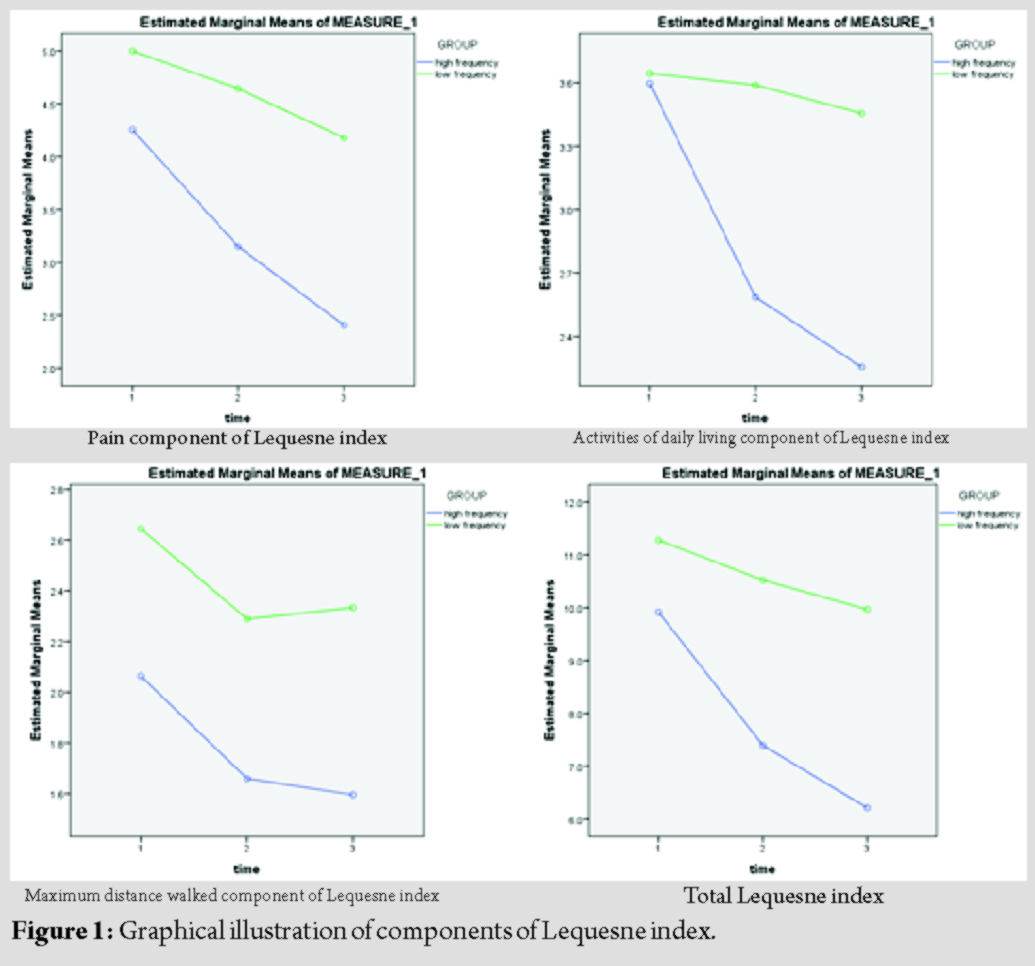
1. Pain component of Lequesne index (Fig. 1: Top left)
F test: 18.478
P value: <0.001 (significant)
Df: 1
Mean difference (95% CI): −1.338 (−1.956, −0.720)
For the pain component of Lequesne index between groups (H-F and L-F), both groups show improvement with time. However, the improvement in the H-F group is much more and is statistically significant (P < 0.001) as compared to the L-F group. This is evident by the steeper graph as seen above.
2. Activities of daily living component of Lequesne index (Fig. 1: Top right)
F test: 5.490
P value: 0.021 (significant)
Df: 1
Mean difference (95% CI): −0.751 (−1.388, −0.114)
For the activities of daily living component of Lequesne index between groups (H-F and L-F), both groups show improvement with time. However, the improvement in the H-F group is much more and is statistically significant (P = 0.021) as compared to the L-F group. This is evident by the steeper graph as seen above.
3. Maximum distance walked component of Lequesne index (Fig. 1: Bottom left)
F test: 2.816
P value: 0.097 (not significant)
Df: 1
For the maximum distance walked component of Lequesne index between groups (H-F and L-F), both groups show improvement, especially in the 1st month. However, this improvement between the groups is not statistically significant (P = 0.097) as evident by the relatively similar graph pattern.
4. Total Lequesne index (Fig. 1: Bottom right)
F test: 7.318
P value: 0.012 (significant)
Df: 1
Mean difference (95% CI): −4.560 (−8.031, −1.088)
For the total Lequesne index between groups (H-F and L-F), both groups show improvement with time. However, the improvement in the H-F group is much more and is statistically significant (P = 0.012) as compared to the L-F group. This is evident by the steeper graph as seen above.
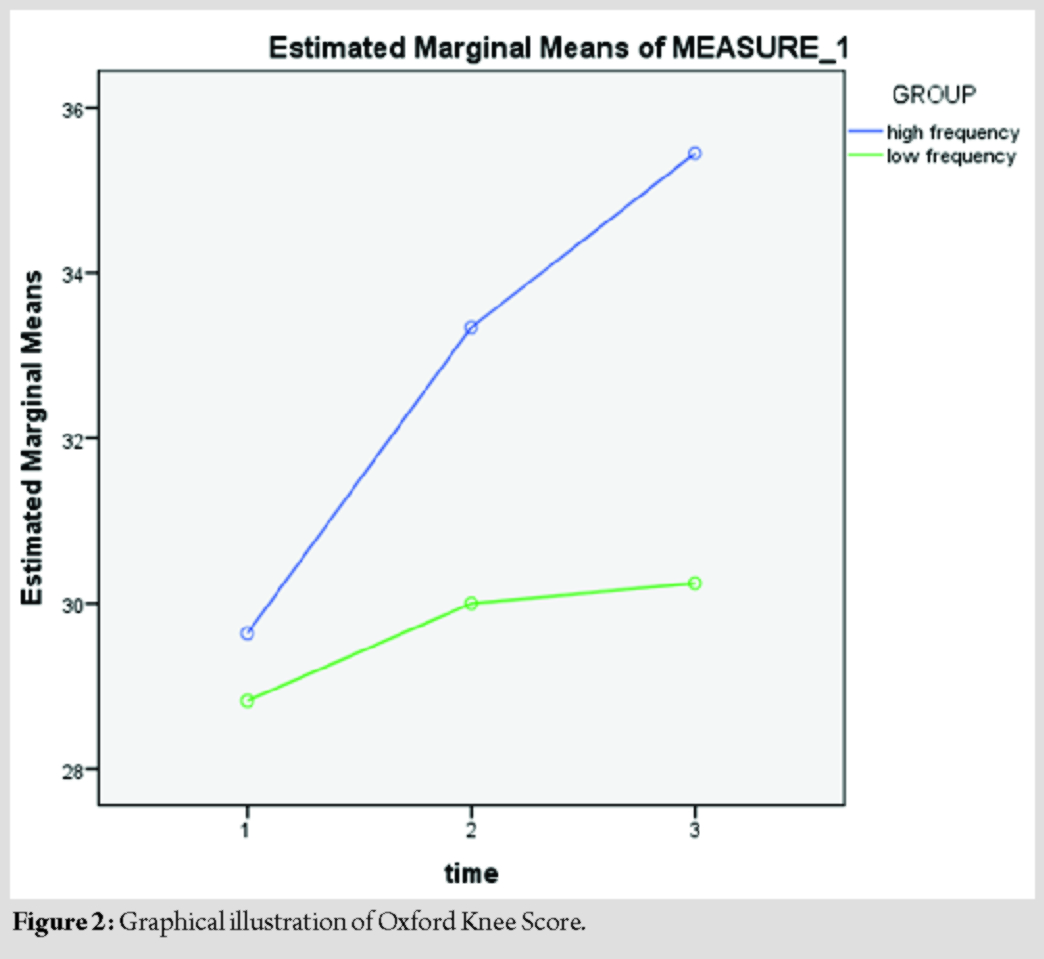
5. Oxford Knee Score (OKS) (Fig. 2)
F test: 3.686
P value: 0.058 (not significant)
Df: 1
For the Oxford Knee Score between groups (H-F and L-F), both groups show improvement with time. This improvement between the groups is statistically not significant (P = 0.058).
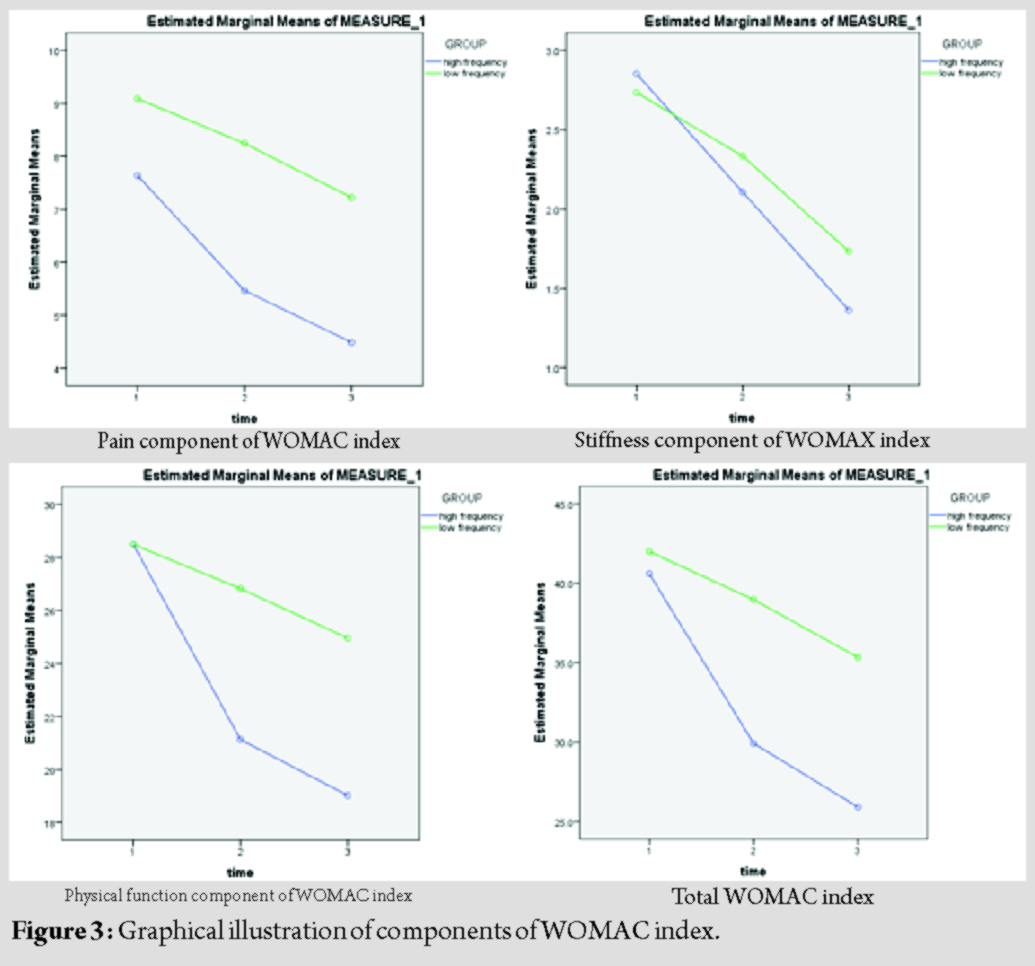
6. Pain component of WOMAC index (Fig. 3: Top left)
F test: 8.331
P value: 0.005 (significant)
Df: 1
For the pain component of WOMAC index between groups (H-F and L-F), both groups show improvement with time. However, the improvement in the H-F group is much more and is statistically significant (P = 0.005) as compared to the L-F group. This is evident by the steeper graph as seen above.
7. Stiffness component of WOMAC index (Fig. 3: Top right)
F test: 0.225
P value: 0.637 (not significant)
Df:1
For the stiffness component of WOMAC index between groups (H-F and L-F), both groups show improvement with time. This improvement between the groups is statistically not significant (P = 0.637).
8. Physical function component of WOMAC index (Fig. 3: Bottom left)
F test: 1.719
P value: 0.193 (not significant)
Df: 1
For the physical function component of WOMAC index between groups (H-F and L-F), both groups show improvement with time. This improvement between the groups is statistically not significant (P = 0.193).
9. Total WOMAC index (Fig. 3: Bottom right)
F test: 2.563
P value: 0.113 (not significant)
Df: 1
For the total WOMAC index between groups (H-F and L-F), both groups show improvement with time. This improvement between the groups is statistically not significant (P = 0.113).
10. VAS (Fig. 4)
F test: 3.043
P value: 0.084 (not significant)
Df: 1
For the VAS between groups (H-F and L-F), both groups show improvement with time. This improvement between the groups is statistically not significant (P = 0.084).
Discussion
Both the H-F and L-F groups show improvement in all components of Lequesne index, Oxford Knee Score, WOMAC index, and the VAS. However, when comparing the improvements between groups, only the pain component of Lequesne index, activities of daily living component of Lequesne index, total Lequesne index, and the pain component of WOMAC index show a statistically significant difference all favoring the H-F group, indicating that the improvement in the H-F group in these components is much more as compared to the L-F group. The remaining components, namely, the maximum distance walked component of Lequesne index, Oxford Knee Score, stiffness component of WOMAC index, physical function component of WOMAC index, total WOMAC index, and the VAS show no statistically difference in their improvement; however, the H-F group has shown to achieve the desired effect at a faster rate as evident by the steeper inclination of the graph shown above. As for the overall results, this study yields 73% report in improvement rate with the use of TENS therapy (combination of both groups). About 80% improvement seen with the H-F group and 66% improvement seen with the L-F groups. 19 patients reported no improvement of symptoms (7 from the H-F group and 12 from the L-F group) and 8 patients were dropped out of the study for not adhering to the criteria of the study. 2 specifically report that they were unable to tolerate the H-F. Previous studies on effectiveness of TENS on knee osteoarthritis only yield an average of 60–67% improvement, as compared to 73% in this study. This better yield of results may be attributed to the investigator’s effort in combining the findings from various studies such as increasing pulse amplitude, application of interferential current concept, and daily use despite symptoms. The other possible reasons being different race and ethnics may react differently to the treatment. There are a few limitation to this study. First being the duration, a 12th week follow-up shows no significant difference between the groups; however, a longer follow-up may yield a different result. Also should a longer duration study be conducted, we would be able to see if this improvement will continue to occur with time or the effect will eventually plateau off at some point. The other limitations being patients compliance as patients carry out the treatment by self at home, although this error has been minimized by providing the patients with a patient diary to record each time they undergone the therapy. Finally, this study is conducted only among the local population, different race and ethnics may yield different results. Thereby, similar studies with longer duration should be conducted in different continents to see if this result is consistent.
Conclusion
Both H-F and L-F groups show improvement in all the components of Lequesne index, Oxford Knee Score, WOMAC index, and the VAS with no statistical difference between the two groups.
Clinical Message
Thereby, both H-F and L-F TENS therapies should be considered as an alternative non-pharmacological method of treatment. The choice should depend on the severity of symptoms, patient’s expectation, and patient’s ability to withstand the treatment therapy. In patients with high threshold for pain with severe symptoms and expects a faster result should consider the H-F setting. Where else patients with low threshold for pain or mild symptoms, may consider the L-F setting.
References
1. Garrison DW, Foreman RD. Decreased activity of spontaneous and noxiously evoked dorsal horn cells during transcutaneous electrical nerve stimulation (TENS). Pain 1994;58:309-15.
2. Hollman JE, Morgan BJ. Effect of transcutaneous electrical nerve stimulation on the pressor response to static handgrip exercise. Phys Ther 1997;77:28-36.
3. Sjolund B, Eriksson M. The influence of naloxone on analgesia produced by peripheral conditioning stimulation. Brain Res 1979;173:295-301.
4. Walsh DM, Liggett C, Baxter D, Allen JM. A double-blind investigation of the hypoalgesic effects of transcutaneous electrical nerve stimulation upon experimentally induced ischaemic pain. Pain 1995;61:39-45.
5. Sluka KA, Bailey K, Bogush J, Olson R, Ricketts A. Treatment with either high or low frequency TENS reduces the secondary hyperalgesia observed after injection of kaolin and carrageenan into the knee joint. Pain 1998;77:97-102.
6. Law PP, Cheing GL. Optimal stimulation frequency of transcutaneous electrical nerve stimulation on people with knee osteoarthritis. J Rehabil Med 2004;36:220-5.
7. Vance CG, Rakel BA, Blodgett NP, DeSantana JM, Amendola A, Zimmerman MB, et al. Effects of transcutaneous electrical nerve stimulation on pain, pain sensitivity, and function in people with knee osteoarthritis: A randomized controlled trial. Phys Ther 2012;92:898-910.
8. Chen WL, Hsu WC, Lin YJ, Hsieh LF. Comparison of intra-articular hyaluronic acid injections with transcutaneous electric nerve stimulation for the management of knee osteoarthritis: A randomized controlled trial. Arch Phys Med Rehabil 2013;94:1482-9.
9. Cherian JJ, Kapadia BH, Bhave A, McElroy MJ, Cherian C, Harwin SF, et al. Use of transcutaneous electrical nerve stimulation device in early osteoarthritis of the knee. J Knee Surg 2015;28:321-8.
10. Cherian JJ, Kapadia BH, McElroy MJ, Johnson AJ, Bhave A, Harwin SF, et al. Knee osteoarthritis: Does transcutaneous electrical nerve stimulation work? Orthopedics 2016;39:e180-6.
11. Cheing GL, Tsui AY, Lo SK, Hui-Chan CW. Optimal stimulation duration of TENS in the management of osteoarthritic knee pain. J Rehabil Med 2003;35:62-8.
12. Lundeberg T, Nordemar R, Ottoson D. Pain alleviation by vibratory stimulation. Pain 1984;20:25-44.
13. Pantaleão MA, Laurino MF, Gallego NL, Cabral CM, Rakel B, Vance C, et al. Adjusting pulse amplitude during transcutaneous electrical nerve stimulation (TENS) application produces greater hypoalgesia. J Pain 2011;12:581-90.
 |
 |
 |
 |
| Dr. Charles Ang Poh Thean | Dr. Mohd Shukrimi Bin Awang | Dr. Zamzuri Bin Zakaria | Dr. Ardilla Hanim Binti Abdul Razak |
| How to Cite This Article: Charles APT, Shukrimi BA, Zamzuri BZ, Ardilla HAR. Portable Transcutaneous Electrical Nerve Stimulation Therapy at Different Frequencies in the Treatment of Knee Osteoarthritis: A Quasi-Experimental Study. Journal of Orthopaedic Case Reports 2020 May-June;10(3): 108-113. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


