
[box type=”bio”] Learning Point of the Article: [/box]
ACL reconstruction in a case of multiple osteochondromatosis can be challenging. Keen attention to tunnel positions and correct choice of implants can result in a predictable outcome.
Case Report | Volume 10 | Issue 4 | JOCR July 2020 | Page 31-34 | Deepak A Tambe, Aditya C Pawaskar, Kiran P Dhole, Ashok K Rathod, Ajinkya R Bandebuche. DOI: 10.13107/jocr.2020.v10.i04.1788
Authors: Deepak A Tambe[1], Aditya C Pawaskar[2], Kiran P Dhole[2], Ashok K Rathod[2], Ajinkya R Bandebuche[3]
[1]Department of Orthopaedics, Rural Medical College of Pravara Medical Trust, Loni, Maharashtra, India,
[2]Department of Orthopaedics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India,
[3]Department of Orthopaedics, Topiwala National Medical College and B.Y.L. Nair Charitable Hospital, Mumbai, Maharashtra, India
Address of Correspondence:
Dr. Aditya C Pawaskar,
Department of Orthopaedics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India.
E-mail: pawaskaraditya@gmail.com
Abstract
Introduction: Osteochondroma is the most common benign bone tumor and usually occurs in the metaphyseal region of the long bones. Anterior cruciate ligament (ACL) tear is the most common ligament injury of the knee joint, and reconstruction of the ACL is the most commonly performed procedure in the knee joint nowadays.
Case Presentation: A 26-year-old male with multiple osteochondromas around the knees, shoulders, and ankles presented with a chronic ACL injury. Reconstruction of ACL using quadrupled hamstring tendon grafts was done. Anterior drawer and Lachman tests were negative postoperatively. The Cincinnati score increased from 180 to 310 at 3-month follow-up. This is a novel case report to describe ACL injury in a case of osteochondromatosis managed by an arthroscopic ACL reconstruction. The problems faced are discussed.
Conclusion: Our report highlights the fact that ACL tear may occur in a patient having osteochondromas around the knee. ACL reconstruction can be performed in routine fashion in such patients with particular attention to careful harvesting of grafts and tunnel placements.
Keywords: Anterior cruciate ligament reconstruction, anterior cruciate ligament reconstruction, osteochondroma, multiple osteochondromatosis.
Introduction
Osteochondroma or exostosis is one of the most common benign bony tumorous conditions commonly occurring in lower extremities [1]. It involves painless bony swellings around the joint. Hereditary multiple osteochondromatosis or exostoses is a rare genetic disorder characterized by the presence of multiple osteochondromas [2]. Common sites are metaphysis of long bones, but can also be seen at the diaphysis of long bones. The diagnosis is based on the clinical and radiological findings. Malignant transformation to osteochondrosarcoma occurs in 1–5% of the patients and more commonly with increasing age [3]. These are usually asymptomatic but may get complicated by nerve compression, vessel injury, and chest complications. Symptoms also depend on the location of the mass and the complications it leads to, which include fracture, bone deformity, mechanical joint problems, vascular, and neurological compromise. In this case report, we present a patient with multiple osteochondromas who suffered an anterior cruciate ligament (ACL) injury which was treated by an arthroscopic reconstruction. Such injury has not been reported in the literature.
Case Presentation
A 26-year-old male suffered trauma to his left knee 2 years back by fall of a heavy suitcase over his left knee. He developed pain and swelling in the knee in 5–6 h, which was managed just by anti-inflammatory drugs. He, however, had no relief and started experiencing giving away of the knee while walking and descending steps and occasional locking episodes. He underwent primary treatment with a general practitioner but never saw an orthopedic surgeon. On clinical examination, anterior drawer test and Lachman test were positive. Bony swellings were seen around the injured knee on the distal femur and proximal tibia, which were asymptomatic. The swellings measured approximately 5 cm in all dimensions. On further, examination swellings were also noted in both shoulders and ankles. His pre-operative Cincinnati score was 180.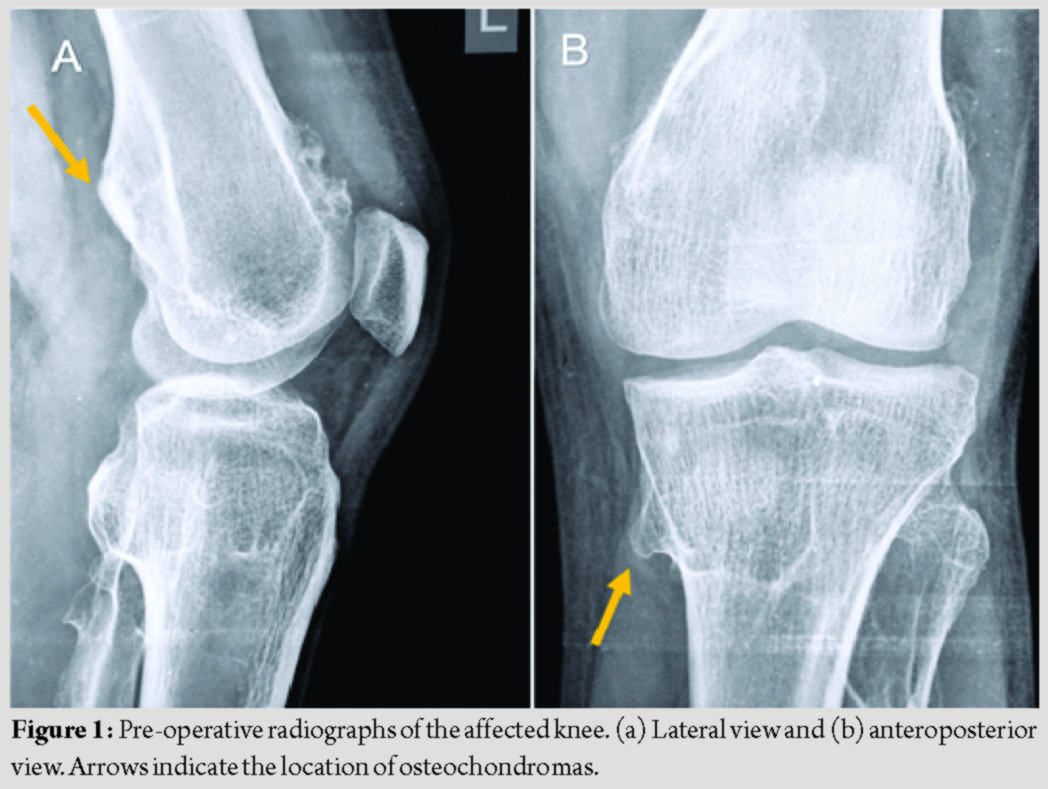
Radiographs of the knee revealed bony swellings of the left proximal tibia and left distal femur, which suggested osteochondromas (Fig. 1). Radiographs of other joints revealed osteochondromas of both ankles and shoulders (Fig. 2). MRI of the left knee revealed a bucket handle tear involving the posterior horn and body of the medial meniscus. A complete tear of the ACL is shown in Fig. 3. The diagnosis of osteochondroma was also confirmed on MRI.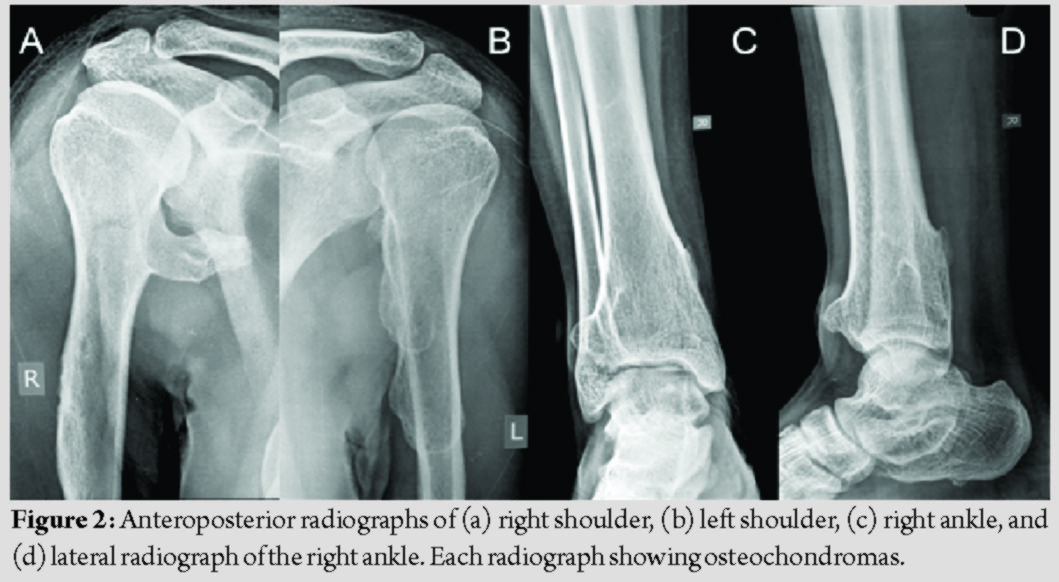
The patient was operated under spinal anesthesia in a supine position with the leg hanging by the side. Anteromedial and anterolateral portals were used during the procedure. A 2.5 cm longitudinal incision just below and medial to tibial tuberosity was used for harvesting the hamstring tendons. Arthroscopy revealed normal synovium, a bucket handle tear of the medial meniscus, and a complete ACL tear (Fig. 4). Articular cartilages were pristine. No other intra-articular pathology was appreciated. The medial meniscus was treated by partial meniscectomy and balancing. Reconstruction of ACL using quadrupled semitendinosus and gracilis tendon grafts was done using fixed loop endobutton (Endo-CL, Smith and Nephew, Andover, MA) on femoral side and a titanium interference screw on the tibial side.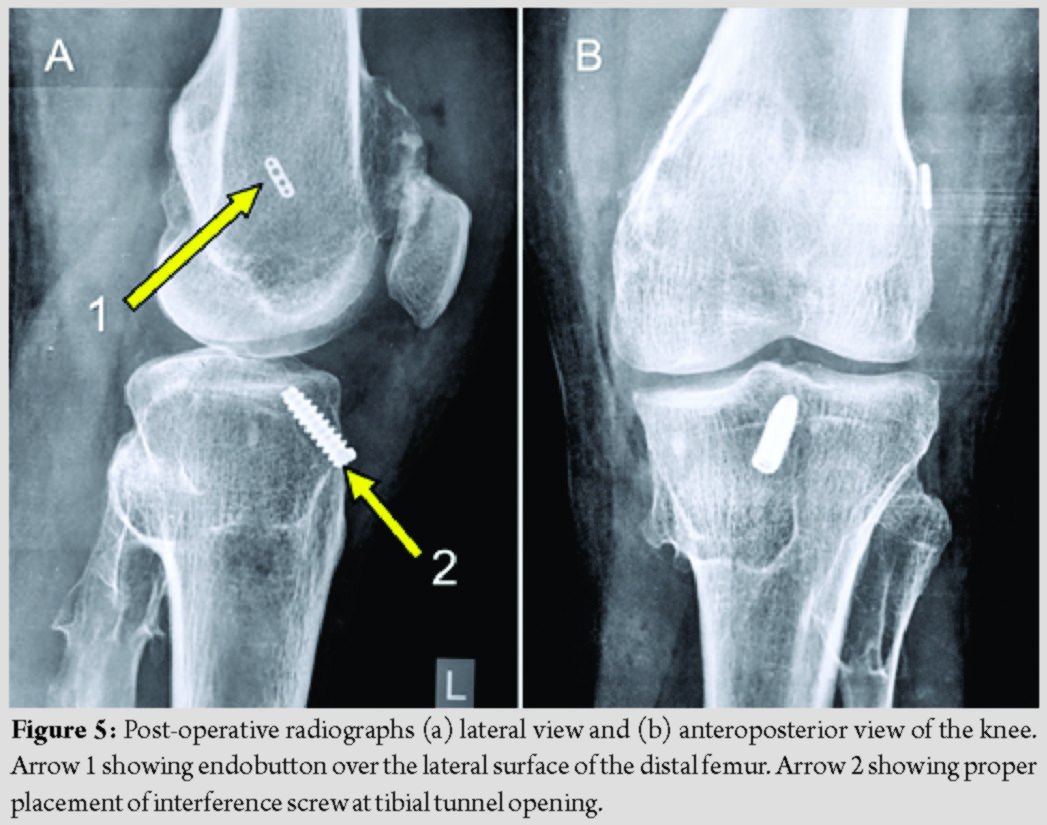
The problem faced by us was in graft harvesting. The tibial osteochondroma was underlying the pes insertion. There was difficulty in the identification of pes. A vertical 2.5 cm incision was taken for a better orientation of pes tendons. The upper border of pes insertion was then identified, which was lying caudal to the medial tibial osteochondroma. Pes insertion was cut vertically, and semitendinosus, and gracilis tendons where caught in a Kocher’s forceps. Tendons were freed from the fascial bands. It was difficult to maneuver the tendon stripper around the tumor. Finally, the stripper was passed to cross the tibial osteochondroma and retrieve the graft. Reaming for the tibial interference screw passed through the junction of the tumor and normal bone. The purchase of the interference screw in the bone, however, was firm. Post-fixation probing of the graft revealed an adequately tensioned graft. Gentle, on table anterior drawer testing revealed correction of pre-operative status. There was no impingement of the graft in the femoral notch on full extension. Post-operative radiographs revealed the proper placement of interference screw at the tibial tunnel opening and endobutton over the lateral surface of the distal femur (Fig. 5).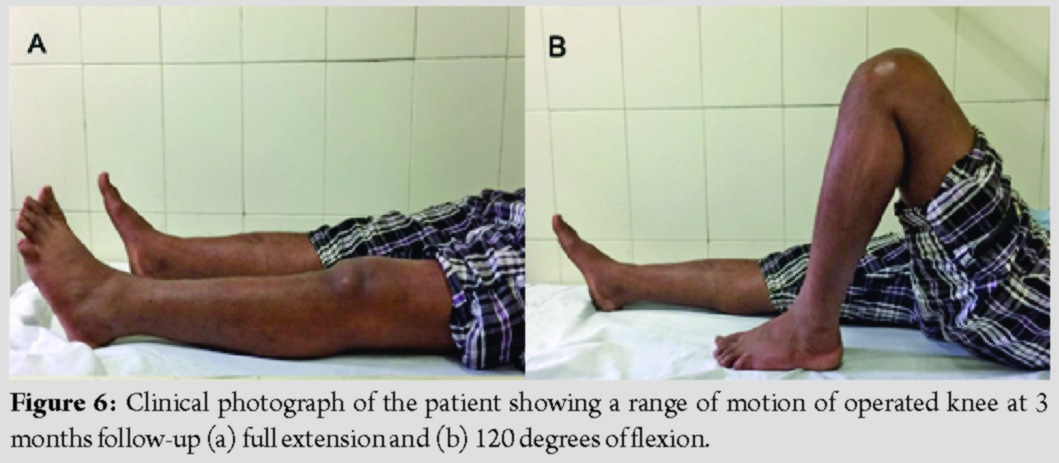
Post-operative rehabilitation involved partial weight-bearing with a brace for 2 weeks followed by full weight-bearing. Active and active-assisted knee range of motion (ROM) with strengthening exercises were started on the 2nd day. At 2 weeks, operative wounds had healed well, and suture removal was done. At our last follow-up at 3 months, the Cincinnati score was 310. The ROM of the knee was a complete extension to 120° of flexion (Fig. 6). Lachman and anterior drawer tests were negative.
Discussion
We ran a comprehensive search on PubMed, Google, and Scopus for similar cases, but no such case of ACL injury in a case of osteochondroma was found. Musculoskeletal injuries associated with osteochondromas are rare, and involvements reported to date include snapping medial hamstring tendon, cystic involvement of ACL, rotator cuff tears, and subacromial, ischiofemoral, or femoroacetabular impingement [4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. Intra-articular osteochondromas have also been reported earlier in the hip, ankle, and knee, but none associated with ACL tear [14, 15]. The previous reports of osteochondromas arising from ACL do not deal with an ACL injury and reconstruction. Alaqeel and Al-Ahaideb reported an osteochondroma originating from the ACL. The patient presented with pain and restricted knee ROM. Arthroscopic excision of the ACL mass was done without an ACL reconstruction. Six months post-surgery patient gained full ROM with no ACL laxity [4]. Chung et al. reported a case of synovial osteochondromatosis originating from the synovium of the ACL with multiple loose bodies in the knee. The patient experienced pain and swelling; however, there was no ligamentous laxity. Arthroscopic removal of loose bodies and ACL excision was done, but ACL was not reconstructed as the patient opted for conservative management. The patient did not experience much discomfort in daily activities postoperatively [5]. Chekofsky reported an 8-year-old boy having epiphyseal osteochondroma of ACL. The first arthrotomy did not have any positive findings. The second arthrotomy revealed the mass growing into the ACL. The mass was excised along with 70% of the ACL [6]. Morey et al. reported an intercondylar osteochondroma of the knee. The mass was excised arthroscopically. Postoperatively, the patient was painless and had attained full knee ROM [7]. Thus, none of the reported studies have reported an association of an ACL tear with osteochondroma, for which an arthroscopic reconstruction was done.
Conclusion
Our report highlights the fact that ACL tear may occur in a patient having osteochondromas around the knee. ACL reconstruction can be performed in routine fashion in such patients with special attention to careful harvesting of grafts and tunnel placements.
Clinical Message
ACL reconstruction can be performed in routine fashion in patients with osteochondromas around the knee. Special attention is to be given while harvesting a graft from the medial aspect of the proximal tibia and tibial tunnel placements near the location of osteochondroma at the proximal tibia.
References
1. Kitsoulis P, Galani V, Stefanaki K, Paraskevas G, Karatzias G, Agnantis NJ, et al. Osteochondromas: Review of the clinical, radiological and pathological features. In Vivo 2008;22:633-46.
2. Stieber JR, Dormans JP. Manifestations of hereditary multiple exostoses. J Am Acad Orthop Surg 2005;13:110-20.
3. Ozaki T, Hillmann A, Blasius S, Link T, Winkelmann W. Multicentric malignant transformation of multiple exostoses. Skeletal Radiol 1998;27:233-6.
4. Alaqeel MA, Al-Ahaideb A. Synovial osteochondroma originating from the synovium of the anterior cruciate ligament. BMJ Case Rep 2013;2013:bcr2012008218.
5. Chung JW, Lee SH, Han SB, Hwang H, Lee D. A synovial osteochondroma replacing the anterior cruciate ligament at the intercondylar notch. Orthopedics 2011;34:136.
6. Chekofsky KM, Scott WN, Fielding JW. Epiphyseal osteochondroma of the anterior cruciate ligament. Clin Orthop Relat Res 1979;139:86-7.
7. Morey VM, Jalan D, Mittal R, Gamangatti S. Intraarticular osteochondroma of the knee. Indian J Orthop 2014;48:332-4.
8. Assefa D, Murphy RC, Bergman K, Atlas AB. Three faces of costal exostoses: Case series and review of literature. Pediatr Emerg Care 2011;27:1188-91.
9. Göçmen S, Topuz AK, Atabey C, Şimşek H, Keklikçi K, Rodop O. Peripheral nerve injuries due to osteochondromas: Analysis of 20 cases and review of the literature. J Neurosurg 2014;120:1105-12.
10. Pavić P, Vergles D, Sarlija M, Ajduk M, Cupurdija K. Pseudoaneurysm of the popliteal artery in a patient with multiple hereditary exostoses. Ann Vasc Surg 2011;25:268.e1-2.
11. Huang TF, Wu JJ, Chen TS. Bilateral shoulder bursal osteochondromatosis associated with complete rotator cuff tear. J Shoulder Elbow Surg 2004;13:108-11.
12. Viala P, Vanel D, Larbi A, Cyteval C, Laredo J. Bilateral ischiofemoral impingement in a patient with hereditary multiple exostoses. Skeletal Radiol 2012;41:1637-40.
13. Hussain W, Avedian R, Terry M, Peabody T. Solitary osteochondroma of the proximal femur and femoral acetabular impingement. Orthopedics 2010;33:51-4.
14. Siebenrock KA, Ganz R. Osteochondroma of the femoral neck. Clin Orthop Relat Res 2002;394:211-8.
15. Yamashita T, Sakamoto N, Ishikawa I, Usui M, Fujisawa Y. Intra-articular osteochondroma of the ankle joint. J Foot Ankle Surg 1998;37:66-8.
 |
 |
 |
 |
 |
| Dr. Deepak A Tambe | Dr. Aditya C Pawaskar | Dr. Kiran P Dhole | Dr. Ashok K Rathod | Dr. Ajinkya R Bandebuche |
| How to Cite This Article: Tambe DA, Pawaskar AC, Dhole KP, Rathod AK, Bandebuche AR. Arthroscopic Anterior Cruciate Ligament Reconstruction in a Case of Multiple Osteochondromatosis: A Case Report. Journal of Orthopaedic Case Reports 2020 July;10(4): 31-34. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


