
[box type=”bio”] Learning Point of the Article: [/box]
Necrotizing fasciitis is a rapidly progressive infection of soft tissues with an obvious dilemma of a lifesaving amputation be necessary sometimes in situations, such as septic shock.
Case Report | Volume 10 | Issue 4 | JOCR July 2020 | Page 54-58 | Iraklis Itsiopoulos, Angelo V Vasiliadis, Dimosthenis Tsitouras, Patroklos Goulas, Petroula Malliou, Kiriakos Ktenidis. DOI: 10.13107/jocr.2020.v10.i04.1800
Authors: Iraklis Itsiopoulos[1], Angelo V Vasiliadis[2], Dimosthenis Tsitouras[1], Patroklos Goulas[1], Petroula Malliou[1], Kiriakos Ktenidis[3]
[1]Propedeutic Surgical Clinic, AHEPA University Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece,
[2]Department of Orthopaedic Surgery, “Papageorgiou” General Hospital of Thessaloniki, Thessaloniki, Greece,
[3]Vascular Surgery Clinic, AHEPA University Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece.
Address of Correspondence:
Dr. Dr. Angelo V Vasiliadis,
Department of Orthopaedic Surgery, “Papageorgiou” General Hospital of Thessaloniki, Thessaloniki, Greece.
E-mail: vasiliadis.av@gmail.com
Abstract
Introduction: Necrotizing fasciitis (NF) is known to be a life-threatening condition of the subcutaneous tissue and superficial fascia with rapid progression.
Case Presentation: This case report will present a relevant case and summarize the literature to discuss the dilemma of amputation in patients with NF. We present the case of a 32-year-old male with a longstanding history of intravenous drug abuse, who developed NF from a benign cellulitis after injection drug use in his right groin region, for which he underwent surgical debridement followed by above-the-knee amputation because of septic shock. He was discharged after 6 months from admission with all blood biochemical parameters recovered to normal.
Conclusion: Prompt intravenous antibiotics administration, surgical debridement, fluid and electrolytes management, and analgesia are the pillars of the treatment, while amputation seems to be a life-saving procedure.
Keywords: Necrotizing fasciitis, Staphylococcus aureus, surgical debridement, amputation
Introduction
Necrotizing fasciitis (NF) is a rapidly progressive, potentially lethal bacterial infection. It is a rare and severe infection, characterized by extensive necrosis of the dermis, subcutaneous tissue, fat, superficial fascia, deep fascia, and/or muscle [1]. Conventionally, NF is classified into four types, according to microbiological findings, without differences in clinical course, morbidity or mortality between the types [2]. Recognized predisposing risk factors include age (over 60 years), chronic diseases (diabetes mellitus, renal failure, and peripheral vascular disease), non-traumatic conditions (skin ulcer, abscess, burns, and soft-tissue infection), trauma (blunt or penetrating), multiple needle punctures, and surgical intervention [3, 4]. Treatments include rapid intravenous administration of appropriate antibiotics and surgical debridement. However, even with proper treatment, the amputation rates are up to 22% and mortality rates range from 6% to 76%, with a cumulative mortality rate of 34% [1, 3]. In this case report, we present the clinical case of a patient suffering from NF caused by Staphylococcus aureus after intravenous drug abuse, who underwent above knee amputation as a life-saving procedure. Informed consent was obtained from the patient after the nature of the procedures had been fully explained.
Case Presentation
A 32-year-old male presented to our emergency department (ED) complaining of painful right lower limb swelling, difficulty to walk, generalized weakness, and fever for 5 days. He had no history of trauma or any chronic medical illnesses, such as diabetes mellitus or coronary artery disease. He had a positive history of hepatitis C (positive anti-hepatitis C virus) and a longstanding history of intravenous drug abuse. His last use was 5 days ago around groin region. Further, physical examination revealed identifying points of focal tenderness, ecchymosis, and marked edema of knee joint (Fig. 1a). He was admitted in the department of pathology for further evaluation. A total of 60 ml of turbid yellowish synovial fluid were aspirated from the right knee joint and were sent to the laboratory for culture. At this time, neurological and vascular examination of the limb was satisfactory. A preliminary clinical diagnosis of cellulitis and the suspicion of septic arthritis of the knee (Fig. 1a and b) were made, while a regimen of empiric intravenous antibiotics (piperacillin and metronidazole) and intravenous fluids was commenced.
His initial vital signs were abnormal, with blood pressure of 98/54 mmHg, heart rate of 123 b/min, respiratory rate of 22/min, oxygen saturation of 92% on room air, and temperature of 38.1°C. The patient was alert, oriented, and neurovascularly intact in both lower limbs. In the ED, the patient was given intravenous fluids and was placed on a cardiac monitor with continuous pulse oximetry. He was given nonsteroidal anti-inflammatory drugs for analgesia. The initial blood investigation revealed 11,060/μL white blood cells, C-reactive protein: 36.8 mg/dL, hematocrit: 40.7%, hemoglobin:14.3 g/dL platelets of 184,000/μL, D-dimers: 127,5 μg/L, urea: 100 mg/dL, creatinine: 0.81 mg/dL, erythrocyte sedimentation rate: 108 mm/h, Na: 145 mmol/L, K: 4.6 mmol/L, creatine kinase: 1210 IU/L, and lactate dehydrogenase: 355 IU/L. After the initial evaluation, the area of cutaneous ecchymosis appeared worse (Fig. 1c). Urgent contrast-enhanced computed tomogram (CT) scan of his right thigh and knee was performed and revealed marked inflammatory stranding and low attenuation with suspicion of necrosis mainly in rectus femoris and vastus lateralis (Fig. 2). The CT added important value to the previous clinical and laboratory findings, enhancing the suspicion of NF. Immediately, the patient was guided to the operation theater and underwent prompt surgery. The surgery consisted of knee arthrotomy, extensive synovectomy, irrigation with 9 L of saline, and debridement of all infected soft tissues. Moreover, wide fasciotomy through anterolateral approach of the thigh and the debridement of extensive necrosis of subcutaneous fat and vastus lateralis were performed (Fig. 1d). The diagnosis was confirmed intraoperatively by the necrosis of the fascia and later on by the analysis of the tissue samples, which revealed S. aureus infection. As a result, intravenous vancomycin was added to the antibiotic regimen.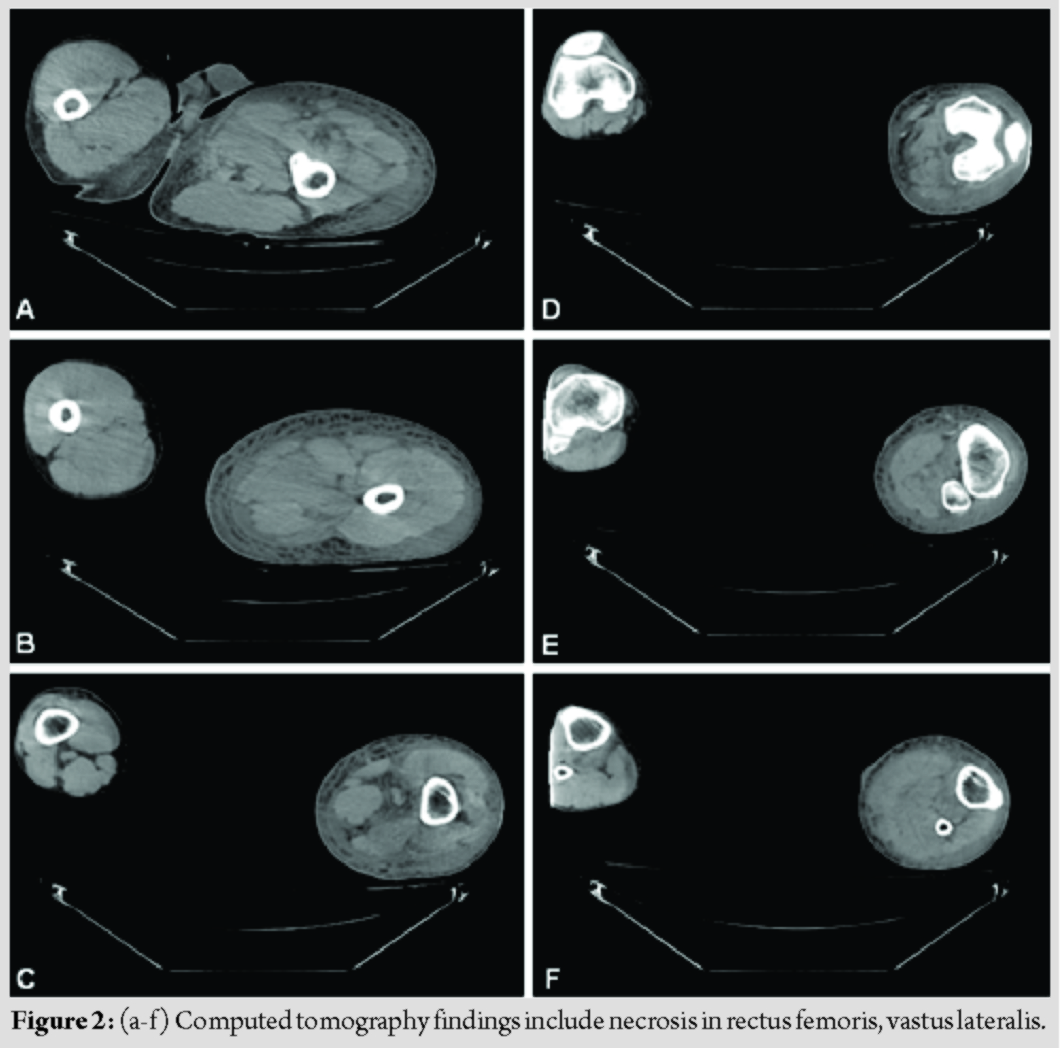
After the operation, the patient was admitted to the intensive care unit (ICU) and daily evaluation of the open wound with irrigation and aggressive surgical debridement was made whenever was necessary, to control a possible new infection and reduce mortality. However, 7 days later, the lesions became worse with foul-smelling necrotic materials. The decision of surgical exploration (in the operation theater) was made, to remove extensive necrosis of the fascia and surrounding tissues in the wound (Fig. 3a). During surgical debridement of the infected tissues in the thigh, knee, and tibia, a major vessel bleeding was observed. For this reason, an angiography was made, which revealed a large popliteal and peroneal artery thrombosed aneurysm. Surgical management consisted of hematoma/thrombus evacuation and stent insertion. Within 20 days, his clinical condition was very improved so the reconstructive and plastic surgeries were scheduled, to repair the damaged tissues (Fig. 3b). Unfortunately, 2 weeks later, his clinical picture deteriorated into septic shock (Fig. 3c) and he underwent a life-saving above-the-knee amputation to control this devastating condition (Fig. 3d). Following amputation, he remained to ICU for metabolic and hemodynamic support. He stayed 104 days in the ICU and then he was transferred to the department for further local wound care and fluid management. In total, the patient was admitted for 174 days and discharged and followed-up at regular intervals.
Discussion
NF is a severe form of soft-tissue bacterial infection with rapid progression, in which inflammation spreads across the fascial plane within the subcutaneous tissue [3, 4]. NF is predominantly caused by polybacterial infection from pathogens such as Klebsiella pneumonia, Aeromonas hydrophila, Pseudomonas aeruginosa, and Streptococcus [3, 4, 5, 6]. There have been rare reports of monobacterial NF caused by S. aureus (Table 1) [7, 8]. In the present case report, the course of infection was shown during the first 5 days but progressed rapidly. Despite the proper antibiotic coverage, the patient required an above knee amputation as a life-saving procedure. It is known that soft-tissue infection and cultures due to S. aureus are more likely to have cellulitis than NF. The present case report, along with the recently described cases in the literature [7, 8], provides evidence that S. aureus can be a bacterial factor that can cause severe NF. Review of the literature demonstrates a wide variety of different risk factors. NF generally impacts patients with chronic diseases. The majority of patients developing NF have some form of chronic diseases, such as poorly controlled or untreated diabetes [3, 8, 9], liver cirrhosis [10], coronary artery disease [3, 8], renal insufficiency [1], and use of injection drugs [9]. Trauma may also precede NF and usually the site of pathogen entry can be a puncture, a bruise, a laceration, a blister, a surgical wound, or a site of drug injection (Table 1) [3, 6, 7, 9, 11]. In our case, the patient had a medical history for hepatitis C infection and a longstanding history of intravenous drug abuse. Due to this fact, he was on chronic immunosuppressive therapy. His suppressed immune system contributed to the mild symptoms and the delay of the recognition of the infection. This led to an accelerated progress of the infection increasing the risk of limb amputation and mortality. Lower limbs were the mainly affected sites at initial presentation [4, 6, 8, 9, 12] followed by perineum, trunk head, and neck [1, 2]. The clinical presentation of NF entails progressive skin changes. On early stages, the most common initial sign is an erythematous area with edema, severe tenderness, and local warmth [7, 8, 9]. Occasionally, some patients may have unstable presentation. In a Hong Kong study, two patients presented with toxic shock [10]. Most of the patients presented in the later stages of NF accompanied with tissue crepitation, hyposensitivity, blister formation, and rarely with hemorrhagic bullae. This was attributed to the delay in referral, misdiagnosed in the previous health-care professional and non-proper treatment therapy [3, 8]. A high index of suspicion in patients with unexplained limb pain is the key for reaching an early diagnosis and to have a successful management [1, 4, 10]. When the diagnosis of NF is established, urgent exploration of the infection site and surgical debridement is imperative. Empiric intravenous antibiotic therapy should be administrated as soon as possible. The choice of treatment for NF is based on surgery, including aggressive debridement of all necrotic tissues and incisional drainage of involved fascia planes through extensive fasciotomy [4, 6, 9]. It is important to reevaluate the patient within 24 h as multiple surgical debridements are often necessary since the infection is rarely eliminated after a single debridement. Often, entire muscle groups are infected and must be removed. It is crucial to remove all tissues and structures that are infected to control the infection and prevent the spread of the infection to vital organs [5, 9, 11]. NF has the potential to become severe when there are irreversible necrotic changes or in the situation of an uncontrolled infection that predisposes a toxic appearance [4, 6]. In these situations, the dilemma of amputation, as a life-saving procedure, is a reality and seems to be the best answer to promptly control the septic focus [8, 11]. Amputation is usually a quicker treatment option that requires minimal reconstructive surgery resulting in a shorter recovery period than radical debridement [1]. Moreover, amputation is usually a shorter procedure which is associated with less blood loss. However, it is correlated with high rate of post-operative cardiopulmonary complications. Notwithstanding, appropriate post-operative care minimizes this risk. In contrary, radical debridement has less post-operative complications and the ability to mobilize the patient earlier after debridement. However, a radical debridement is not as quick as amputation to control the septic focus and as a result, multiple debridements may be done [11]. While amputation might be the answer to control a rapid infection, especially in a critically ill patient, a limb amputation does not affect significantly the survival rates [11, 13]. Tang et al. [13] noted in their study that in more severely affected cases that underwent amputation, there was a decrease in the mortality rate. They also reported that the level of involvement in the limb on admission had a significant effect on the rate of mortality, with infection in the proximal part of a limb at the time of admission had a high mortality. The same can be concluded from our literature review, where infection in the proximal part of a limb and trunk present seemed to increase mortality rate (Table 1) [3, 10].
Conclusion
Prompt intravenous antibiotics administration, surgical debridement, fluid and electrolytes management, and analgesia are the pillars of the treatment. Amputation might be necessary to control the infection or in case of a rapid deterioration of the patient’s health. The decision to amputate versus radical debridement must be made with great caution as both procedures have their own advantages and disadvantages.
Clinical Message
NF is a severe life-threatening soft-tissue bacterial infection most classically seen in patients with a history of diabetes mellitus, immunosuppression, and intravenous antibiotic drug abuse. A high index of suspicious leading to an early diagnosis and a subsequent prompt treatment with aggressive surgical therapy in concert with empirical intravenous antibiotic therapy is essential because of the high mortality rate of the disease. Amputation of the limb may be sometimes unavoidable, particularly in patients with an uncontrolled infection that predisposes to septic shock status.
References
1. Cheng NC, Wang JT, Chang SC, Tai HC, Tang YB. Necrotizing fasciitis caused by Staphylococcus aureus: The emergence of methicillin-resistant strains. Ann Plast Surg 2011;67:632-6.
2. Navinan MR, Yudhisdran J, Kandeepan T, Kulatunga A. Necrotizing fasciitis-a diagnostic dilemma: Two case reports. J Med Case Rep 2014;8:229.
3. Nazerani S, Maghari A, Motamedi MH, Ardakani J, Rashidian N, Nazerani T. Necrotizing fasciitis of the upper extremity, case report and review of the literature. Trauma Mon 2012;17:309-12.
4. Smeets L, Bous A, Heymans O. Necrotizing fasciitis: Case report and review of literature. Acta Chir Belg 2007;107:29-36.
5. Sun J, Tian X, Fang W, Huang J, Zhang T, Ding J. Post-traumatic necrotizing fasciitis and sepsis shock caused by Aeromonas hydrophila: A case report and summary of related reports. Biomed Res 2017;28:9885-9.
6. Huang YH, Hsieh TY, Chen IC, Lai CS, Lin SD, Lee SS, et al. Amputation of lower limb for necrotizing soft-tissue infection in an ultramarathon runner. Formos J Surg 2014;47:62-5.
7. Chauhan H, Patil S, Hajare A, Krishnaprasad K, Bhargava A. Necrotizing fasciitis of hand by methicillin resistant Staphylococcus aureus (MRSA)-a sinister. J Clin Diagn Res 2015;9:DD01-2.
8. Morgan WR, Caldwell MD, Brady JM, Stemper ME, Reed KD, Shukla SK. Necrotizing fasciitis due to a methicillin-sensitive Staphylococcus aureus isolate harboring an enterotoxin gene cluster. J Clin Microbiol 2007;45:668-71.
9. Suykerbuyk C, Frykberg R. Necrotizing fasciitis: A case report. J Diabet Foot Complications 2010;2:1-5.
10. Tang WM, Ho PL, Yau WP, Wong WK, Yip DK. Report of 2 fatal cases of adult necrotizing fasciitis and toxic shock syndrome caused by streptococcus agalactiae. Clin Infect Dis 2000;31:E15-7.
11. Ang N, Thomson M. Amputations and necrotizing fasciitis: A case report. Am Med Stud Res J 2015;2:71-4.
12. Jain M, Mavani K. Lethal necrotizing fasciitis triggered by plaster: Case report and review of literature. J Orthop Case Rep 2016;6:73-5.
13. Tang W, Ho P, Fung K, Yuen K, Leong J. Necrotising fasciitis of a limb. J Bone Joint Surg Br 2001;83:709-14.
 |
 |
 |
 |
 |
| Dr. Iraklis Itsiopoulos | Dr. Angelo V Vasiliadis | Dr. Dimosthenis Tsitouras | Dr. Patroklos Goulas | Dr. Kiriakos Ktenidis |
| How to Cite This Article: Itsiopoulos I, Vasiliadis AV, Tsitouras D, Goulas P, Malliou P, Ktenidis K. Amputation in Necrotizing Fasciitis – Dilemma or Reality: A Case Report and Literature Review. Journal of Orthopaedic Case Reports 2020 July;10(4): 54-58. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


