
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
Penetrating plant thorn injuries can cause devastating articular septic arthritis despite no foreign bodies that are found in ultrasound.
Case Report | Volume 11 | Issue 3 | JOCR March 2021 | Page 13-15 | Jorge Teixeira Ramos, Nuno Barbosa, João Almeida, Samir Karmali, Rui Guerreiro, Glória Magalhães. DOI: 10.13107/jocr.2021.v11.i03.2066
Authors: Jorge Teixeira Ramos[1], Nuno Barbosa[1], João Almeida[1], Samir Karmali[1], Rui Guerreiro[1], Glória Magalhães[1]
[1]Department of Orthopedic Surgery, Hospital Vila Franca de Xira, Vila Franca de Xira, Portugal.
Address of Correspondence:
Dr. Jorge Teixeira Ramos,
Department of Orthopedic Surgery, Hospital Vila Franca de Xira, Vila Franca de Xira, Portugal.
E-mail: jorge.a.ramos@hvfx.pt
Abstract
Introduction: A monoarthritic painful knee may have multiple etiologies, of which septic arthritis is commonly considered to be one of the most deleterious pathologies. This type of acute symptom is, in the literature, for some rare cases, related to an inflammatory process secondary to a penetrating plant thorn, which was considered an aseptic process and therefore treated by removing the foreign body. This work reports a recent case falling into that diagnosis, which due to its infrequent nature, could have been misevaluated and consequently mistreated.
Case Report: Our goal is to bring to the attention of the orthopedic community that this type of deleterious pathology, which is today uncommon, must never be fully disregarded. We share a case of a 68-year-old male who was admitted 2 days after being injured by a palm tree (Arecaceae) thorn with acute inflammatory signs and effusion in the left knee. Although, ultrasound excluded pathway or intra-articular foreign bodies, in the arthroscopic procedure, a thorn was found and removed. Pantoea agglomerans was identified in the synovial fluid.
Conclusion: Following the removal of the foreign body, empirical antibiotic treatment with coverage against Gram-negative pathogens was initiated and later on replaced by appropriate antibiotics, after susceptibility testing is obtained.
Keywords: Knee, palm tree, pantoea agglomerans, septic arthritis, thorn.
Introduction
Monoartrhitis of the knee is a common presentation in the emergency room, which can have a broad variety of diagnosis. Being aware of the multiple possible diagnosis is key to the adequate management of those patients. Degenerative or traumatic etiologies are the most common causes, nevertheless infectious or inflammatory diseases should be suspected in some specific cases. Among the rare cases addressed in the literature for plant thorn synovitis, some early reports pointed to a foreign body/toxin-related reaction with sterile synovial fluid [1, 2]. More recent reports tend to propose microorganisms as a significant contributing factor with Pantoea agglomerans being the most frequent [3, 4].
Case Report
This work presents the case of a 68-year-old male with a palm tree thorn penetrating injury to the lateral supra-patellar side of his left knee while gardening and which was claimed to have been immediately removed. Only diabetes mellitus type 2 was found as a relevant comorbidity. Two days later, he presented to the ER feeling feverish, with a swollen, painful left knee which exacerbated by articular movement despite being on rest, ice, and anti-inflammatory medication. No other articular involvement was found. Physical examination demonstrated an auricular temperature of 37.3oC and a swollen, warm, and highly painful knee. There was a relevant intra-articular effusion with a range of movement restricted to 30o–90o. Skin inspection revealed a lateral millimetric entry wound. Blood tests disclosed a leukocytosis (14.4×10^3/µL) with neutrophilia (89.1%) and RCP of 4.44 mg/dL. Percutaneous arthrocentesis was done, and a cloudy synovial fluid was collected and sent for culture and biochemistry revealing a cell count of 14×10^4 Cells/µL, 92% being polymorphonuclear cells. Plain radiographs were unremarkable. Ultrasound excluded the presence of any foreign bodies near the entry wound or intra-articular. As septic arthritis was suspected, urgent arthroscopy was performed. No tourniquet was used and 2g Cefazolin was administered after synovial fluid was harvested to culture. Anterolateral and anteromedial portals were used, and generalized synovitis was found. Mild damage to the patellofemoral joint was found, presumed chronic. At the suprapatellar pouch, a foreign body was found that matched the distal end of the thorn (Fig. 1A, B). Lavage with 9L saline and arthrotomy was performed to exclude the thorn pathway. The knee was protected with Robert–Jones dressing (soft-padded bandages) for 5 days to allow careful mobilization and a faster functional recovery. Total weight-bearing was advised according to pain. Empiric antibiotic therapy was initiated with amoxicillin + clavulanic acid, 875 mg + 125 mg tid. On the 6th post-operative day, Pantoea agglomerans was identified in the synovial fluid susceptible to amoxicillin + clavulanic acid and resistant to ampicillin and amoxicillin. The patient was discharged at day 6 and kept antibiotic therapy for 6 weeks. At that time, physical examination as well as the analytic control were unremarkable (no inflammatory parameters were elevated, namely, RCP and leucocytes).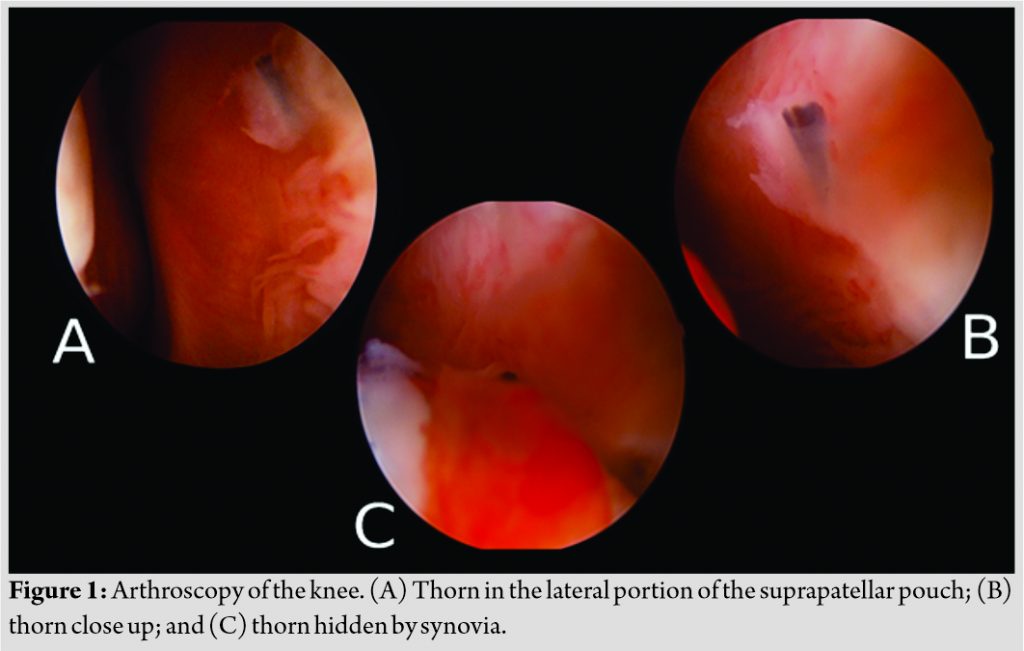
Discussion
Arhtritis secondary to plant thorn prick is an established medical condition occurring mostly on children [5]. Palm tree thorn (Phoenix dactylifera) appears to be the most frequently involved, perhaps due to its length and the tip being prone to break inside the articulation [4]. Although, the knee seems to be the most frequently affected joint, this type of condition can also occur on other joints [6, 7, 8]. As mentioned above, early reports dated as far as 1953 referred to an aseptic arthritis probably due to an allergic foreign body reaction or to the plant toxins [1], which lead this disease to be commonly addressed as “Blackthorn inflammation” [9]. For those cases, antibiotic therapy seemed to provide additional relief over symptomatic therapy [3, 9] and only in 1977 was published the first paper identifying Staphylococcus albus, Streptococcus hemolyticus, and Gram-negative rods as the main relevant causative agents of this monoartrhitis [3]. Moreover, it was not until 1978 that Pantoea agglomerans appeared for the first time in the literature described as an etiologic agent for this disease [10]. In the present case, we had a patient with an acute presentation favoring the link between the thorn and the arthritis. Nevertheless, according to the reported literature, most cases present in a subacute/chronic fashion which can delay/impair the diagnosis [11, 12]. Radiographs are useless in detecting foreign bodies in the acute phase, although they can be of use in the chronic setting if osteolytic changes have occurred in response to the inflammatory process. This case shows that although ultrasound is usually sufficient to identify any fragment, this was not the case, as it failed to identify the foreign body detected during surgery. In fact, CT scans or MRI are known to be able to provide additional information but are seldom necessary and were not requested; therefore, the ability of such methods to identify foreign bodies is not possible to be evaluated in the scope of the present work. In the past times, and before the widespread use of arthroscopic treatment, the removal of foreign bodies as palm tree thorns was commonly conducted through arthrotomy [1, 3, 12]. Nowadays, the advantages of arthroscopic treatment outweigh arthrotomy by simultaneously allowing complete articular inspection and foreign body removal.
Conclusion
In this case, it was highlighted that one must be aware that an acute symptomatic painful knee may have multiple etiologies, which include the inflammatory process deriving from a penetrating plant thorn. This work also stresses out the possibility of any foreign body, and in particular a plant thorn, being obscured by any reactive synovia (Fig. 1C) and for that reason not be identified through the most commonly used methods. As with any other infection, antibiotherapy is the cornerstone of treatment and should be initiated as soon as possible. Empirical therapy should begin as soon as fluids for culture are harvested and should be adjusted according to microorganism susceptibilities with relation to reported resistances [13].
Clinical Message
Penetrating plant thorn injuries can cause devastating articular septic arthritis despite no foreign bodies are found in ultrasound. Foreign body removal and expeditious antibiotherapy are cornerstone for a good outcome.
References
1. Karshner RG, Hanafee W. Palm thorns as a cause of joint effusion in children. Radiology 1953;60:592-5.
2. Olenginski TP, Bush DC, Harrington TM. Plant thorn synovitis: An uncommon cause of monoarthritis. Semin Arthritis Rheum 1991;21:40-6.
3. Sugarman M, Stobie DG, Quismorio FP, Terry R, Hanson V. Plant thorn synovitis. Arthritis Rheum 1977;20:1125-8.
4. Kratz A, Greenberg D. Pantoea agglomerans as a cause of septic arthritis after palm tree thorn injury; case report and literature review. Arch Dis Child 2003;88:542-4.
5. Cahill N, King JD. Palm thorn synovitis. J Pediatr Orthop 1984;4:175-9.
6. Blake DR, Bacon PA, Scott CA, Potter AR. Monoarthritis from blackthorn injury: A novel means of diagnosis. Br Med J (Clin Res Ed) 1981;282:361-2.
7. Freiberg AA, Herzenberg JE, Sangeorzan JA. Thorn synovitis of the knee joint with Nocardia pyarthrosis. Clin Orthop Relat Res 1993;287:233-6.
8. Miller EB, Gilad A, Schattner A. Cactus thorn arthritis: Case report and review of the literature. Clin Rheumatol 2000;19:490-1.
9. Kelly JJ. Blackthorn inflammation. J Bone Joint Surg Br 1966;48:474-7.
10. Flatauer FE, Khan MA. Septic arthritis caused by Enterobacter agglomerans. Arch Intern Med 1978;138:788.
11. De Champs C, Le Seaux S, Dubost JJ. Isolation of Pantoea agglomerans in two cases of septic monoarthritis after plant thorn and wood sliver injuries. J Clin Microbiol 2000;38:460-1.
12. Zoltan JD. Cactus thorn synovitis. Arthroscopy 1991;7:244-5.
13. Hamilton-Miller JM, Shah S. Identity and antibiotic susceptibility of enterobacterial flora of salad vegetables. Int J Antimicrob Agents 2001;18:81-3.
 |
 |
 |
 |
| Dr. Jorge Teixeira Ramos | Dr. Nuno Barbosa | Dr. João Almeida |
Dr. Samir Karmali |
| How to Cite This Article: Ramos JT, Barbosa N, Almeida J, Karmali S, Guerreiro R, Magalhães G. Knee Septic Arthritis after Palm Tree Thorn Injury: A Case Report. Journal of Orthopaedic Case Reports 2021 March 11(3):Page 13-15 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


