
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]Leptospirosis is a rare but possible cause of reactive arthritis, especially when associated with jaundice and other clinical manifestations of leptospirosis.
Case Report | Volume 11 | Issue 3 | JOCR March 2021 | Page 79-84 | Sudipan Dey, Arun Kumar Sipani, Rajdeep Das. DOI: 10.13107/jocr.2021.v11.i03.2098
Authors: Sudipan Dey[1], Arun Kumar Sipani[2], Rajdeep Das[2]
[1]Department of Orthopaedics, Diphu Medical College and Hospital, Diphu, Assam, India,
[2]Department of Orthopaedics, Silchar Medical College and Hospital, Silchar, Assam, India.
Address of Correspondence:
Dr. Rajdeep Das,
S/O Late Rajat Kanti Das, House No: 15, Sreepally Lane, College Road, Silchar – 788 007, Assam, India.
E-mail: rajdeepdas92@gmail.com
Abstract
Introduction: Leptospirosis is a zoonosis caused by infection with pathogenic Leptospira species. Leptospirosis has protean manifestations and rare, unusual presentations should be kept in mind in relevant epidemiological scenario. Reactive arthritis refers to acute non-purulent arthritis complicating an infection elsewhere in the body. It is attributed to an immune activation following certain infections; it is, therefore considered as aseptic arthritis. Very few case reports are available attributing leptospirosis as an established cause of reactive arthritis. We present a case of reactive arthritis of the hip joint due to leptospirosis.
Case Report: Here, we present a case of a 12-years- old female child who was admitted to our hospital with complaints of fever, headache, and pain in the right hip joint since past 5 days from admission. Subsequent elaboration revealed a past history of fever, headache, and myalgia for around 5-7 days around a week before the present complaints. There was rat infestation near her house and her father was working as sewage cleaner. Routine investigations, Ultrasonography (USG), Magnetic Resonance Imaging (MRI) of both hips and subsequently, diagnostic hip aspiration was performed. USG revealed synovitis, MRI revealed hip joint arthritis of infective or inflammatory origin. Diagnostic hip aspiration was negative for any microorganism. On 10th day of admission, patient started developing icterus with yellowish discolouration of urine. Patient was evaluated for the cause of jaundice. Screening for Leptospira was positive. Synovial biopsy of hip was performed, which showed inflammation with no specific pathology and no growth of any microorganism. In addition, Leptospira IgM MAC ELISA was done which was positive. Patient was thus confirmed to be having leptospirosis and reactive arthritis as a consequence of it.
Conclusion: The presentation of reactive arthritis secondary to leptospirosis is rare. Leptospirosis can be an etiological factor for reactive arthritis, especially if reactive arthritis is complicated with jaundice.
Keywords: Reactive arthritis, Reiter’s syndrome, leptospirosis.
Introduction
Leptospirosis is considered to be the most widespread zoonosis in the world caused by spirochetes belonging to the order Spirochaetales and the family Leptospiraceae. Leptospires are coiled microorganisms with hooked ends. They are motile by two periplasmic flagella. Recent phylogenetic and virulence analyses have classified the genus Leptospira into 22 species – ten pathogenic, five intermediate, and seven non-pathogenic [1]. The species has several serological variants – the serovars. Serovar based taxonomy continues to have epidemiological value [2].
Clinical features
The incubation period of the disease is 1–2 weeks, but ranges from 1 day to 30 days [1]. Leptospirosis classically manifests as a biphasic illness [2]. The first phase of the disease (septicemic phase) lasts for about 3–10 days duration [1] and coincides with leptospiremia. Symptoms include fever, headache, body ache, mild cough, rash, nausea, and vomiting. Signs include conjunctival suffusion, lymphadenopathy, and anorexia [2]. If present, the skin rash is often transient, lasting <24 h [3]. This phase is followed by a brief afebrile period of variable duration that, in turn, is followed by the immune phase of illness. Fever returns heralding the second phase of illness (immune phase) that may be accompanied by jaundice and renal failure. During this period, leptospires are excreted in urine [2]. Liver and kidneys are commonly affected. Both organ derangements are reversible. Unfortunately, the distinction between first and second phase is not always clear; milder cases do not always include the second phase, and severe cases may be monophasic and fulminant [1].
The source of infection is usually direct or indirect contact with urine, blood, or tissue from an infected animal or more commonly, exposure to environmental contamination [1]. It usually enters through an abrasion or cut in the skin or through mucous membrane. Inhalation of water or aerosols [3] and rarely, animal bites [1] also may result in infection.
Immunological manifestation is rare and includes antiphospholipid syndrome and reactive arthritis. Such manifestations are likely to be the result of an immunological cross reactivity. Antibodies generated in response to leptospiral infection may cross react with host antigens and could lead to an inflammatory response [2]. Reactive arthritis refers to an infection-induced systemic illness and is characterized by an aseptic inflammatory joint involvement occurring in a genetically predisposed patient with a bacterial infection localized in a distant organ/system [4] involving the musculoskeletal, ophthalmologic, dermatologic, cardiovascular, and genitourinary systems [5]. The definition of reactive arthritis must be based on the major and minor criteria that are shown [6, 7]:
Major criteria
1. Arthritis, with two of three of the following findings:
• Asymmetric
• Mono- or oligoarthritis
• Affection predominantly in lower limbs
2. Preceding symptomatic infection, with one or two of the following findings:
• Enteritis (diarrhea for at least 1 day, 3 days–6 weeks before the onset of arthritis)
• Urethritis (dysuria or discharge for at least 1 day, 3 days–6 weeks before the onset of arthritis)
Minor criteria, at least 1 of the following:
1. Evidence of triggering infection
• Positive nucleic acid amplification test in the morning urine or urethral/cervical swab for Chlamydia trachomatis
• Positive stool culture for enteric pathogens associated with reactive arthritis
2. Evidence of persistent synovial infection (positive immunohistology or Polymerase Chain Reaction for Chlamydia).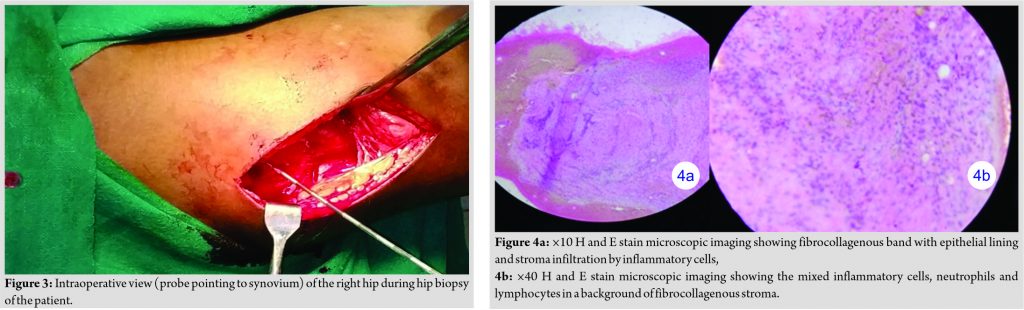
A “definite” diagnosis of reactive arthritis is based on the fulfillment of both major criteria and a relevant minor criterion, while a “probable” diagnosis is characterized by both major criteria but no relevant minor criterion or one major criterion and one or more of the minor criteria. The identification of the trigger infection is also required [7].
Reactive arthritis is a well-defined clinical syndrome, occurring after enteric infection with any of the several Shigella, Salmonella, Yersinia, and Campylobacter species; by genital infection with C. trachomatis and other agents as well. Organisms such as Clostridium difficile, Campylobacter coli, certain toxigenic Escherichia coli, Ureaplasma urealyticum, and Mycoplasma genitalium are also causative agents of reactive arthritis. Chlamydia pneumoniae is another trigger of reactive arthritis, although far less common than C. trachomatis [1]. There is also evidence that it can also be caused by pathogens like: parvovirus B19, Gonococcus species, mycobacterial, and streptococcal infections, as well as parasitic diseases such as Entamoeba, Giardia, and Strongyloides [8]. The triad of arthritis, urethritis, and conjunctivitis represents a small part of the spectrum of the clinical manifestations of reactive arthritis and only a minority of patients present with this “classical triad” of symptoms. Human leukocyte antigen B27 (HLAB27) seems to be associated with more severe and chronic forms of the “classical triad” of reactive arthritis. About 30–50% patients of reactive arthritis are HLAB27 positive [1]. Arthritis is usually asymmetric and additive, with involvement of new joints occurring over few days to 1–2 weeks. Arthritis typically persists for 3–5 months, but more chronic courses do occur. Chronic joint symptoms persist in about 15% patients and in up to 60% patients in hospital-based series, but these tend to be less severe than in the acute stage. Recurrences of the acute syndrome are also common. Low back pain, sacroiliitis, and frank ankylosing spondylitis are also common sequelae. In most studies, HLAB27 positive patients have shown a worse outcome than HLAB27 negative patients [1].
Case Report
A 12-years-old female child was admitted to our hospital with complaints of fever, headache, and pain in the right hip joint since past 5 days from admission. She could stand and walk without support, but had difficulty doing her activities of daily living. Subsequent elaboration revealed a past history of fever, headache, and myalgia for around 5–7 days around a week before the present complaints, which subsided on taking oral medications. She was of rural origin and there was rat infestation near her house and her father was working as sewage cleaner. She was otherwise previously apparently healthy. She had an antalgic gait. On clinical examination, the patient was febrile with 101° Fahrenheit, tachycardia was noted, and inguinal lymph nodes were palpable and tender. Local examination of right hip revealed warmth, fullness, tenderness, and global restriction of movements (Fig. 1). Left hip examination was normal. Patient was started on intravenous antibiotic ceftriaxone on an empirical basis along with nonsteroidal anti-inflammatory drugs (NSAIDs) and skin traction. The initial laboratory work-up showed anemia with hemoglobin of 6.4 mg/dL, leukocyte count of 9.04 × 103 cells/µL, and neutrophilia of 74.9%. C-reactive protein was markedly elevated with 93.7 mg/dL, and other biochemical parameters were normal. Chest X-ray and electrocardiogram were normal. USG of abdomen was normal; blood culture was negative for any growth. Urine examination was normal. USG of the right hip showed synovial proliferation suggestive of synovitis. MRI of both hips revealed right hip synovial thickening with enhancement on post-contrast studies, femoral head and acetabulum erosion and irregularity of right hip with joint space reduction, and bone marrow and muscle edema; suggestive of hip joint arthritis of infective or inflammatory origin (Fig. 2a, b, c, d). On 7th day of admission, diagnostic hip aspiration was performed. The synovial fluid analysis showed clear straw color fluid with 30–50 polymorphonuclear leukocytes per high power field with no other abnormality. Fluid was negative for any infectious organism. On 10th day, patient started developing icterus with yellowish discoloration of urine. Total bilirubin was 6.16 mg/dL, conjugated bilirubin 5.14 mg/dL, unconjugated bilirubin 1.02 mg/dL, aspartate aminotransferase 93.5 U/L, alanine aminotransferase 149.4 U/L, alkaline phosphatase 186.1 U/L, and gamma-glutamyl transferase 77.4 U/L. Serum total protein was 8.22 g/dL, and serum albumin was low with 2.83 g/dL. Prothrombin time-international normalized ratio (PT-INR) was slightly deranged with PT-INR of 1.35. Patient was shifted from intravenous ceftriaxone to cefotaxime, NSAIDs were stopped and symptomatic and nutritional management was done. Screening for bacterial and viral causes of hepatitis was negative. Screening for Leptospira was positive. Patient was continued on intravenous cefotaxime and synovial biopsy was performed for confirming the diagnosis and ruling out any infective pathology. The biopsy was done through a posterior approach (Fig. 3). After skin incision and subcutaneous tissue dissection, the gluteus muscle fibers were split to reach the short external rotators of the hip. The piriformis muscle was retracted to gain access to the capsule of the hip. Appropriate synovial biopsy samples were obtained. There was no evidence of any pus or infected tissue. The synovium or articular cartilage did not show pannus or any evidence of gross destruction, thus ruling out infective arthritis. Synovial biopsy analysis showed no growth of any microorganism and histopathological examination showed fibrocollagenous band infiltrated with mixed inflammatory cells with no other specific pathology (Fig. 4a, b). In addition, Leptospira IgM MAC ELISA test was done which was positive. Patient was thus diagnosed to be having leptospirosis and reactive arthritis secondary to it. She was discharged with oral doxycycline for 10 days. Subsequent follow-up of the patient showed complete healing of the operated site (Fig. 5) and follow-up at 6 months showed disappearance of symptoms and near normal restoration of normal hip range of movements. The follow-up roentgenogram of the patient at 6 months shows sclerosis of the acetabular margin (Fig. 6).
Discussion
The term “reactive arthritis” was introduced in the year 1969 [9]. It was defined as arthritis, which develops during or soon after an infection elsewhere in the body, but in which the microorganism does not enter the joint cavity. Since then, it has been shown that antigens of the triggering microbe can be detected in the synovial fluid or synovial tissue of affected joints [10, 11, 12], and rarely, even replicating microbes have been demonstrated in the joints of patients with typical clinical features of reactive arthritis [13]. Despite this, the original definition covers reasonably well the clinical entity of reactive arthritis [6]. A 12-year-old female patient developed reactive arthritis of the hip joint following acute leptospirosis. Manifestations of leptospirosis may range from asymptomatic infection to fulminant fatal disease with myositis, conjunctivitis, hepatic, renal and neurological involvement, and hemorrhagic and immune mediated manifestations. Most of the complications of leptospirosis are associated with localization of leptospires within the tissues during the immune phase [1]. Reactive arthritis is found to be a rare immune mediated complication of leptospirosis [3]. A detailed search through medical literature showed two such case reports [8, 14]. Although most textbooks demand the presence of various extra-articular presentations for diagnosis, the disease most often presents solely as arthritis [8]. Although the causes of reactive arthritis are well known, random reports attributed to other causative agents are advisable. The term could be hypothetically attributed to an antigenic activation of the immune system of the patient. Leptospira species are acknowledged immunomodulators [8]. The surface lipopolysaccharides of Leptospira species are highly immunogenic [3], whereas the role of autoantibodies in the second stage of acute leptospirosis is undeniable. Anticardiolipin antibodies and antineutrophil cytoplasmic antibodies have been reported in course of acute leptospirosis [8]. Doxycycline therapy, by eradicating the leptospires and thereby removing the source of antigens, could prevent the formation of immune complexes leading to a decrease in the inflammatory response [2].
Conclusion
Reactive arthritis is thus a rare manifestation of leptospirosis. The possibility of leptospirosis should be borne in mind when evaluating patients with reactive arthritis and the propensity of various organisms to produce such a syndrome must be speculated further. A high degree of clinical suspicion is necessary, particularly in endemic areas. Physicians should be aware of the possibility of reactive arthritis due to leptospirosis, as the disease presents with unusual features.
Clinical Message
The probability of leptospirosis as a causative agent of reactive arthritis, although very rare, should be considered; especially in the setting of other clinical manifestations of leptospirosis in endemic areas.
References
1. Harrison TR, Kasper DL, Fauci AS. Harrison’s Principles of Internal Medicine. 19th ed. New York: McGraw-Hill; 2015.
2. Bal AM. Unusual clinical manifestations of leptospirosis. J Postgrad Med 2005;51:179-83.
3. Levett PN. Leptospirosis. Clin Microbiol Rev 2001;14:296-326.
4. Flores D, Marquez J, Garza M, Espinoza LR. Reactive arthritis: Newer developments. Rheum Dis Clin North Am 2003;29:37-59.
5. Kim PS, Klausmeier TL, Orr DP. Reactive arthritis: A review. J Adolesc Health 2009;44:309-15.
6. Hannu T. Reactive arthritis. Best Pract Res Clin Rheumatol 2011;25:347-57.
7. Selmi C, Gershwin ME. Diagnosis and classification of reactive arthritis. Autoimmun Rev 2014;13:546-9.
8. Pappas G, Akritidis N, Christou L, Mastora M, Tsianos E. Unusual causes of reactive arthritis: Leptospira and Coxiella burnetii. Clin Rheumatol 2003;22:343-6.
9. Ahvonen P, Sievers K, Aho K. Arthritis associated with Yersinia enterocolitica infection. Acta Rheumatol Scand 1969;15:232-53.
10. Keat A, Dixey J, Sonnex C, Thomas B, Osborn M, Taylor-Robinson D. Chlamydia trachomatis and reactive arthritis: The missing link. Lancet 1987;1:72-4.
11. Granfors K, Jalkanen S, von Essen R, Lahesmaa-Rantala R, Isomäki O, Pekkola-Heino K, et al. Yersinia antigens in synovial-fluid cells from patients with reactive arthritis. N Engl J Med 1989;320:216-21.
12. Granfors K, Jalkanen S, Mäki-Ikola O, Lahesmaa-Rantala R, Saario R, Toivanen A, et al. Salmonella lipopolysaccharide in synovial cells from patients with reactive arthritis. Lancet 1990;335:685-8.
13. Inman RD, Whittum-Hudson JA, Schumacher HR, Hudson AP. Chlamydia and associated arthritis. Curr Opin Rheumatol 2000;12:254-62.
14. Winter RJ, Richardson A, Lehner MJ, Hoffbrand BI. Lung abscess and reactive arthritis: rare complications of leptospirosis. Br Med J (Clin Res Ed) 1984;288:448-9.
 |
 |
 |
| Dr. Sudipan Dey | Dr. Arun Kumar Sipani | Dr. Rajdeep Das |
| How to Cite This Article: Dey S, Sipani AK, Das R. Case report of a rare cause of reactive arthritis: Leptospirosis. Journal of Orthopaedic Case Reports 2021 March;11(3): 79-84. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


