
Bilateral, sequential anterior inferior iliac spine avulsion is a rare but potential injury in young athletes.
Dr. James Brock, Department of Trauma and Orthopaedics, Prince Charles Hospital, Merthyr Tydfil, Wales. E-mail: brockj194@gmail.com
Abstract
Introduction: Pelvic apophyseal injuries are common in young athletes where muscle strength exceeds the tensile strength of the physis. Sequential bilateral injuries are exceedingly rare, and little is known of their mechanism.
Case Presentation: A 15-year-old male cross-country runner presented with bilateral hip pain after sprint training. The patient describes going “flat out” and “overstriding” before collapsing with immediate pain. MRI imaging confirmed an acute bilateral Anterior Inferior Iliac Spine Injury (AIIS). Conservative management included protected weight-bearing, a hip strengthening program and graded return to play. At 6 months, the patient returned to full sporting activities with no symptoms.
Conclusion: We present a unique case of bilateral AIIS avulsion that offers insight into the potential mechanisms and adds to the evidence that these injuries may be managed successfully with conservative treatment.
Keywords: Pelvic avulsion injury, anterior inferior iliac spine.
Bilateral Anterior inferior iliac spine (AIIS) avulsion injuries are extremely rare. Groin injuries account for only 3–5% of sporting injuries in adolescent athletes [1]. Of the six potential pelvic apophyseal injuries, AIIS injury accounts for around 22% of injuries, with the majority caused by ischial tuberosity injury [2]. AIIS injury occurs more commonly in males and between the ages of 14–17 [3]. The injury occurs in this age group, as the ratio of muscular strength to physeal strength is highest [4]. Eccentric contraction of the rectus femoris during forceful extension causes avulsion of the muscle at its origin [5]. Only two cases of bilateral injury have previously been reported in a 100 m sprinter and a long jumper [6,7].
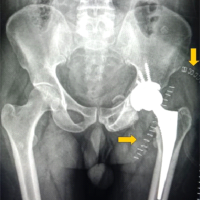
A 15-year-old male cross-country runner presented to accident and emergency immediately after sustaining a bilateral hip injury whilst sprint training at his local club. The patient had warmed up with race walking and was beginning a speed session. During the first sprint, at around the 50 m mark and going “flat out,” the patient felt a sequential “pop” sensation in his hips. This caused immediate pain and the patient to fall to the floor. There was no antecedent injury or pain. The patient was unable to comment on the phase of sprinting at which the injury occurred, but was concentrating on “striding out.” Although a warm up occurred, the patient felt that he could have involved more hip activation exercises. The patient was training 3 times a week at a club level, with no risk of overtraining. The patient had no relevant injury history. Medical history included asthma, eczema, and nut allergy. There was no family history of apophyseal injury. On examination, the patient was of a tall build and entered with wheelchair assistance. He had difficulty weight-bearing due to pain and weakness in his hips and stood with a flexed posture from the waist. He had groin tenderness in both hips and was unable to perform straight leg raise bilaterally. Thomas test revealed bilateral fixed flexion deformities. The patient had normal passive hip flexion to 80’, but passive extension was painful and limited to 25’. There was no neurovascular deficit. Plain radiograph of the pelvis (Fig. 1) confirmed bilateral AIIS spine avulsion injuries. The right AIIS avulsion was displaced at 4.2 mm and the left undisplaced. The patient was admitted overnight for optimization of analgesia and physiotherapy assessment and was the acuteness of the injury which was assessed through MRI (Fig. 2).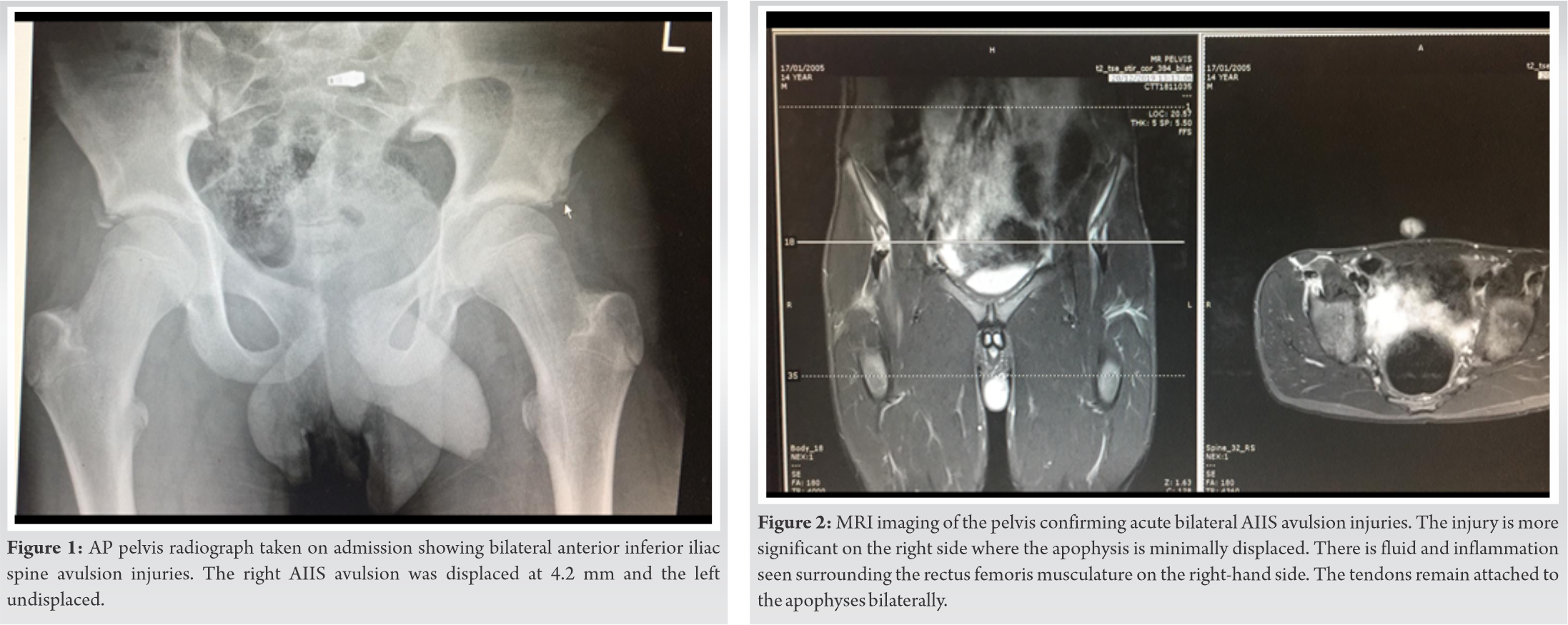 The MRI was reported as evidence of bilateral AIIS injury, more significant on the right side, where the apophysis is minimally displaced. On the MRI, more significant amount of fluid was seen surrounding the rectus femoris musculature on the right side, and both tendons remained attached to the apophyses bilaterally. The patient was discharged with protected weight-bearing, where the patient was given two crutches to use when mobilizing and advised to continue this without sporting activity for 6 weeks. At 2 weeks, the patient was reviewed in fracture clinic with satisfactory radiographs showing no further displacement. He was advised with a further 4 weeks of protected weight-bearing and then to begin a graded return to sporting activity with static bike exercise and swimming. The patient was advised to undertake progressively intense light jogging activities in the pool before progressing to full swimming strokes. The patient had two physiotherapy sessions at 4 and 8 weeks, to initiate and progress a basic hip-strengthening program. The patient was initially lost to follow-up due to the COVID-19 crisis; however, follow-up at 6 months through telephone consultation showed complete resolution of the injury. The patient was able to return to running at 3 months following the injury and his club coach was involved in creating a graded return to play program. This involved slow progression of intensity and distance of training runs. The patient is now 6 months post-injury and has returned to full participation with no symptoms, including sprint training.
The MRI was reported as evidence of bilateral AIIS injury, more significant on the right side, where the apophysis is minimally displaced. On the MRI, more significant amount of fluid was seen surrounding the rectus femoris musculature on the right side, and both tendons remained attached to the apophyses bilaterally. The patient was discharged with protected weight-bearing, where the patient was given two crutches to use when mobilizing and advised to continue this without sporting activity for 6 weeks. At 2 weeks, the patient was reviewed in fracture clinic with satisfactory radiographs showing no further displacement. He was advised with a further 4 weeks of protected weight-bearing and then to begin a graded return to sporting activity with static bike exercise and swimming. The patient was advised to undertake progressively intense light jogging activities in the pool before progressing to full swimming strokes. The patient had two physiotherapy sessions at 4 and 8 weeks, to initiate and progress a basic hip-strengthening program. The patient was initially lost to follow-up due to the COVID-19 crisis; however, follow-up at 6 months through telephone consultation showed complete resolution of the injury. The patient was able to return to running at 3 months following the injury and his club coach was involved in creating a graded return to play program. This involved slow progression of intensity and distance of training runs. The patient is now 6 months post-injury and has returned to full participation with no symptoms, including sprint training.
Gomez describe a similar case to that presented, of a 14-year-old male sprinter who felt sequential “pop” sensations in both hips near the finish line of a 100 m – sprint event at an amateur athletics competition [6]. The injury occurred during a maximal effort sprint and during the top speed phase of the sprint. The patient described an initial “pop” of sudden onset, but then tried to stop suddenly before the second injury. The patient did not collapse and delayed in presenting for medical advice for a week. The patient reported a good warm up and was habituated to sprinting through regular training. The group postulated that both mechanisms of AIIS avulsion, concentric contraction of rectus femoris during push off in the acceleration phase, and eccentric contraction during the recovery phase were involved in this injury. Yildiz et al. described another case in a 17-year-old male long jumper who sustained a sequential, bilateral AIIS avulsion injury 4 months apart [7]. Both injuries were described as occurring during the pre-takeoff phase, where the front leg is flexed in front and the ground leg in a position of full hip and knee extension, where the avulsion injury occurred. This was again a top speed injury, where maximal eccentric contraction of the rectus femoris occurred. The case presented here highlights again the role of eccentric rectus femoris contraction during maximal efforts and the top speed phase of sprinting. Overstriding is where elite sprinters let their shin and foot float forward in the air, before aggressively returning to the ground [8]. This however can be a source of injury risk in novice sprinters, whereby the leg is thrown forward but is not brought in reverse immediately, exposing novices to significant braking forces due to a lack of muscle pre-activation and stiffness in the striking leg [8]. This concept could equally be applied to both previously reported cases. Further research is needed to investigate the biomechanics of sprinting and pelvic apophyseal injury, to guide training specific interventions to minimize risk in adolescent athletes. AIIS avulsion fractures are well treated conservatively. Open reduction and internal fixation are only indicated when there is displacement, evidence of non-union, and persistent functional disability or pain [4,9]. Recent meta-analysis has suggested that pelvic apophyseal injury with displacement >1.5 cm should be managed with operative fixation to facilitate a faster return to play compared to conservative treatment (12 weeks vs. 17 weeks), through earlier return to active exercises and maintenance of thigh muscle strength [10]. Crutch weight-bearing allows for minimization of load through the hip joint in the acute phase. It has also been suggested that positioning the limb to minimize tension may prevent further displacement, this strategy was not specifically employed in this case and no displacement was seen [11]. Unilateral AIIS avulsion injury has been reported to take between 3 weeks and 4 months for full functional recovery [6]. Gomez report a 3-month recovery time for their 100m sprinter, while Yildiz et al. reported near full functional muscle recovery through isokinetic dynamometry at 6 months following the second sequential AIIS injury [6,7]. Our data adds to the suggestion that bilateral injury may take significantly longer than unilateral injury, at 4–6 months for full functional recovery.
This case reports the rare occurrence of bilateral anterior inferior iliac spine avulsion injury, it highlights the role of the top speed phase of sprinting in bilateral apophyseal injury and supports the conservative treatment of bilateral pelvic apophyseal injuries with displacement of <1.5 cm.
References
- 1.Schuett DJ, Bomar JD, Pennock AT. Pelvic apophyseal avulsion fractures: A retrospective review of 228 cases. J Pediatr Orthop 2015;35:617-23. [Google Scholar | PubMed]
- 2.Rossi F, Dragoni S. Acute avulsion fractures of the pelvis in adolescent competitive athletes: Prevalence, location and sports distribution of 203 cases collected. Skelet Radiol 2001;30:127-31. [Google Scholar | PubMed]
- 3.Waters PM, Millis MB. Hip and pelvic injuries in the young athlete. Clin Sports Med 1988;7:513-26. [Google Scholar | PubMed]
- 4.Ogden JA. Skeletal Injury in the Child. 3rd ed. New York: Springer Science and Business Media; 2006. [Google Scholar | PubMed]
- 5.Narayanasamy S, Krishna S, Sathiadoss P, Althobaity W, Koujok K, Sheikh AM. Radiographic review of avulsion fractures. Radiographics 2018;38:1496-7. [Google Scholar | PubMed]
- 6.Gomez JE. Bilateral anterior inferior iliac spine avulsion fractures. Med Sci Sports Exerc 1996;28:161-4. [Google Scholar | PubMed]
- 7.Yildiz C, Yildiz Y, Ozdemir MT, Green D, Aydin T. Sequential avulsion of the anterior inferior iliac spine in an adolescent long jumper. Br J Sports Med 2005;39:e31. [Google Scholar | PubMed]
- 8.Yu J, Sun Y, Yang C, Wang D, Yin K, Herzog W, et al. Biomechanical insights into differences between the mid-acceleration and maximum velocity phases of sprinting. J Strength Cond Res 2016;30:1906-16. [Google Scholar | PubMed]
- 9.Schlonsky J, Olix ML. Functional disability following avulsion fracture of the ischial epiphysis. J Bone Joint Surg Am 1972;54:641-4. [Google Scholar | PubMed]
- 10.Eberbach H, Hohloch L, Feucht MJ, Konstantinidis L, Südkamp NP, Zwingmann J. Operative versus conservative treatment of apophyseal avulsion fractures of the pelvis in the adolescents: A systematical review with meta-analysis of clinical outcome and return to sports. BMC Musculoskelet Disord 2017;18:8. [Google Scholar | PubMed]
- 11.Metzmaker JN, Pappas AM. Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-58. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 6, 2024 Neglected Anterior Dislocation of Hip Managed with Total Hip Arthroplasty Using Dual Approach: A Case Report and Review of Literature
August 6, 2024 Neglected Anterior Dislocation of Hip Managed with Total Hip Arthroplasty Using Dual Approach: A Case Report and Review of Literature August 6, 2024 Candida parapsilosis in Late Prosthetic Joint Infections Among Immunocompetent Patients: A Case Series
August 6, 2024 Candida parapsilosis in Late Prosthetic Joint Infections Among Immunocompetent Patients: A Case Series October 10, 2025 The Rise of Minimally Invasive “DAA” Hip Replacements: Hype, Hope, and Reality
October 10, 2025 The Rise of Minimally Invasive “DAA” Hip Replacements: Hype, Hope, and Reality May 1, 2026 Influence of Cementation Sequence on Screw Fixation Strength in Reconstructed Bone Defects: Experimental Biomechanical Implications for Trauma and Reconstructive Surgery
May 1, 2026 Influence of Cementation Sequence on Screw Fixation Strength in Reconstructed Bone Defects: Experimental Biomechanical Implications for Trauma and Reconstructive Surgery