
Considering age, osteochondroma should be considered among one of the differential diagnoses while dealing with similar cases.
Dr. Nishant Jagdale, Department of Orthopaedics, RCSM GMC, Kolhapur, Maharashtra, India. E-mail: nish.61093@gmail.com
Abstract
Introduction: Osteochondroma is the most common primary benign bone tumor. It’s radiologic characteristics are often pathognomonic. Osteochondromas usually occur at the metaphysis of long bones. The distal end of femur, proximal humerus, proximal tibia, and fibula are the common locations. Most cases present within the first three decades.
Case Report: A 12-year-old boy presented with osteochondroma of left acromion process. It is very unusual for its location with a mass over the left shoulder extending laterally into deltoid muscle. Radiologic studies showed large pedunculated mass arising from the acromion process. On surgical exploration, we found a pedunculated and well encapsulated mass on the lateral aspect of the left shoulder with a thin hyaline cartilaginous cap. The mass was carefully separated from nearby structures and resected en bloc.
Results: No post-operative complications were noticed. Patient was prescribed physiotherapy and we have him advised 6-month follow-up till skeletal maturity. Patient had complete range of motion at the last follow-up. He was able to do his all daily activities.
Conclusion: The acromion is very rare site for osteochondroma with mass extending into lateral deltoid muscle. Careful blunt dissection and protection of nearby structures and fairly good learning curve of surgeon is needed in operating such cases.
Keywords: Osteochondroma, exostoses, acromion process, proximal humerus, tumor.
Osteochondroma is the most common primary benign bone tumor and constitutes 36% to 41% of all tumors [1]. They present in two clinical forms: Single lesion (i.e., solitary osteochondromas) and multiple lesions (i.e., multiple exostoses) [2]. It is a cartilage covered osseous projection that protrudes from the surface of the affected bone. It is produced by progressive enchondral ossification of the hyaline cartilage. In 1920, Keith proposed the cause to be a defect in the perichondral ring around the growth plate [3]. Current thought says the cause being misdirected growth of a portion of growth plate. Most osteochondromas are found in the metaphysis of the distal femur, proximal tibia, and proximal humerus [4]. However osteochondromas may be found at distal radius, distal tibia, proximal and distal fibula, and rarely the flat bones such as ribs, ilium, and scapula. Osteochondromas are also noted within the spinal canal with neurologic compromise [5].
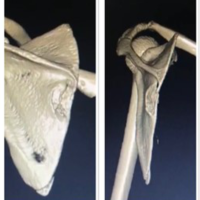
A 12-year-old boy presented with a mass over left shoulder for 1 year. The mass was insidious in onset, gradually progressive, and patient complained of mass effect, irritation while wearing tight clothing or combing hair and cosmetic reason.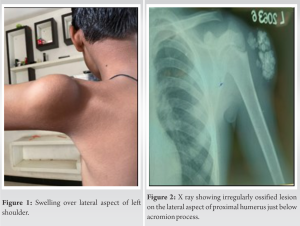 It was not associated with pain. There was no history of trauma to left shoulder. On examination, a hard and trans-illumination negative swelling, measuring 6*4*3 cm, was noted on the lateral aspect of left shoulder just below acromion process (Fig. 1). The swelling was non-mobile, non-tender, and non-adherent to overlying skin or muscle tissue. Skin over the swelling appeared normal. X-ray of the left shoulder showed irregularly ossified lesion on the lateral aspect of proximal humerus just below acromion process (Fig. 2) MRI was done and revealed a large, well defined, fairly well capsulated, and lobulated mass along lateral aspect of proximal humerus measuring 6*4*3.5 cm in size with a thin stalk connecting to postero-lateral corner of acromion process (Fig. 3). It showed multiple areas of extensive calcification with a very thin cartilaginous cap. Above said features defined a benign lesion but few peculiar signs of Exostoses. Hence, patient was posted for J needle biopsy which suggested bony trabeculae along with thin cartilage without dysplasia. As the lesion was benign, excisional biopsy was planned by direct lateral approach to proximal humerus and the mass was carefully separated from surrounding tissue with blunt dissection (Fig. 4).
It was not associated with pain. There was no history of trauma to left shoulder. On examination, a hard and trans-illumination negative swelling, measuring 6*4*3 cm, was noted on the lateral aspect of left shoulder just below acromion process (Fig. 1). The swelling was non-mobile, non-tender, and non-adherent to overlying skin or muscle tissue. Skin over the swelling appeared normal. X-ray of the left shoulder showed irregularly ossified lesion on the lateral aspect of proximal humerus just below acromion process (Fig. 2) MRI was done and revealed a large, well defined, fairly well capsulated, and lobulated mass along lateral aspect of proximal humerus measuring 6*4*3.5 cm in size with a thin stalk connecting to postero-lateral corner of acromion process (Fig. 3). It showed multiple areas of extensive calcification with a very thin cartilaginous cap. Above said features defined a benign lesion but few peculiar signs of Exostoses. Hence, patient was posted for J needle biopsy which suggested bony trabeculae along with thin cartilage without dysplasia. As the lesion was benign, excisional biopsy was planned by direct lateral approach to proximal humerus and the mass was carefully separated from surrounding tissue with blunt dissection (Fig. 4).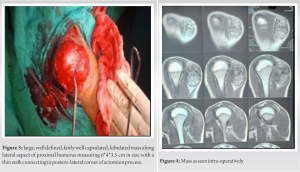 Tumor was excised en bloc. Gross examination of the specimen revealed a thin pedunculated and well encapsulated mass measuring 6*5*4 cm, oval shaped, with a thin cartilaginous cap (Fig. 5). Cut section revealed a grey white mass with variegated appearance. Histopathological examination revealed a benign tumor exhibiting a cap of benign mature cartilage. Sub-cartilagenous areas shows numerus mature bony trabeculae showing enchondral ossification suggestive of osteochondroma (Fig. 6).
Tumor was excised en bloc. Gross examination of the specimen revealed a thin pedunculated and well encapsulated mass measuring 6*5*4 cm, oval shaped, with a thin cartilaginous cap (Fig. 5). Cut section revealed a grey white mass with variegated appearance. Histopathological examination revealed a benign tumor exhibiting a cap of benign mature cartilage. Sub-cartilagenous areas shows numerus mature bony trabeculae showing enchondral ossification suggestive of osteochondroma (Fig. 6). 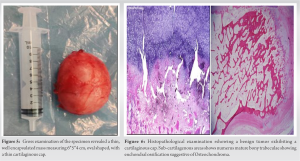 Postoperatively, we did regular dressing and suture removal. Surgical wound healed without any complication. In recent follow-up, patient had full range of motion at shoulder without local irritation and an acceptable surgical scar without any functional limitation of the extremity (Fig. 7a-c). We have advised patient regular follow-up every 6 months or so follow-up if sudden appearance or increase in size of the swelling, till skeletal maturity to diagnose early recurrence.
Postoperatively, we did regular dressing and suture removal. Surgical wound healed without any complication. In recent follow-up, patient had full range of motion at shoulder without local irritation and an acceptable surgical scar without any functional limitation of the extremity (Fig. 7a-c). We have advised patient regular follow-up every 6 months or so follow-up if sudden appearance or increase in size of the swelling, till skeletal maturity to diagnose early recurrence.
A focal herniation of the physeal plate results in an aberrant, cartilage covered, and eccentric small bone. They usually develop in bones that undergoes enchondral ossification but it has been noted in some flat bones like pelvis which develop from intra-membranous ossification [6]. Hereditary Multiple exostoses comprise an autosomal dominant condition but solitary osteochondromas are not genetically transmitted [7,8]. Osteochondromas are usually seen in growing skeleton with male predominance of 1.6–3.4:1 [9,10]. In majority of cases, osteochondroma becomes evident between ages 10 and 20 years. Mostly, it is discovered as incidental finding, or it may be palpated as a protruding bump. However, sometimes may cause localized pain, growth disturbances of an extremity, restricted joint motion or an abnormal cosmetic appearance, or pressure over adjacent tissues. Lower limb swelling secondary to vascular compression by osteochondroma knee has been noted [11]. Bursal osteochondromatosis of the rib has been described [12]. Osteochondroma has several pathognomic radiological findings
- It protrudes from parent bone as sessile or pedunculated mass.
- Never found in epiphysis.
- The lesion ranges between 2 and 12 cm.
- Cortex and cancellous bone of osteochondroma blend with parent bone.
If asymptomatic, solitary osteochondroma does not need to excise. Excision should be planned for lesions who cause symptom (pressure symptoms or cosmetic problems). After skeletal maturity, malignant transformation should be suspected if the cartilaginous cap continues to grow. Excision, if possible, should be postponed till late adolescence, as the growth potential of young lesions is unknown and risk of local recurrence is significant if excised early. Excision usually results in a successful outcome for patients and there is less to none morbidity [4,13].
Acromial osteochondroma is a very rare site for solitary osteochondroma and may cause pressure symptoms over surrounding structures such as axillary nerve and circumflex humeral vessels. Previously, very few cases have been noted. Various differential including osteochondroma should be kept in mind before treating such lesion and they have very low recurrence rate after surgical excision. Although regular follow-up should be advised to the patient to diagnose recurrence or malignant transformation.
History and clinical examination of any swelling is of much more importance than any other investigation. Also one should always know that establishing histopathological diagnosis is the gold standard and also of medico-legal importance while treating any tumor.
References
- 1.Dahlin DC, Unni KK. Bone Tumors: General Aspects and Data on 8542 Cases. Springfield, IL: Charles C Thomas; 1986. [Google Scholar | PubMed]
- 2.Dorfman HD, Czerniak B. Osteochondroma. Bone Tumors. St. Louis: Mosby; 1998. p. 331-46. [Google Scholar | PubMed]
- 3.Keith A. Studies on the anatomical changes which accompany certain growth disorders of the human body. I. The nature of the structural alterations in the disorder known as multiple exostoses. J Anat 1920;54:101-15. [Google Scholar | PubMed]
- 4.Essadki B, Moujtahid M, Lamine A, Fikry T, Essadki O, Zryouil B. Solitary osteocgondroma of the limbs. Clinical review of 76 cases and pathogenic hypothesis. Acta Orthop Belg 2000;66:146-53. [Google Scholar | PubMed]
- 5.Aarskog D, Tveteraas E. McCune-Albright’s syndrome following adrenalectomy for Cushing’s syndrome in infancy. J Pediatr 1968;73:89-96. [Google Scholar | PubMed]
- 6.Gokkus K, Atmaca H, Sagtas E, Saylik M, Ayudin AT. Osteochondromas originating from unusual locations complicating orthopaedic discipline: Case series. Eklem Hastalik Cerrahisi 2015;26:100-9. [Google Scholar | PubMed]
- 7.Francannet C, Cohen-Tanugi A, Le Merrer M, Munnich A, Bonaventure J, Legeai-Mallet L. Genotype-phenotype correlation in hereditary multiple exostoses. J Med Genet 2001;38:430-4. [Google Scholar | PubMed]
- 8.Sherazi Z, Saifuddin A, Shaikh MI, Natali C, Pringle JA. Unusual imaging findings in association with spinal osteoblastoma. Clin Radiol 1996;51:644-8. [Google Scholar | PubMed]
- 9.Heck KR. Benign bone tumors and neoplastic conditions simulating bone tumors. In: Canale ST, Beaty JH, editors. Campbell’s Operative Orthopaedics. 11th ed. Philadelphia, PA: Mobsy Elsevier; 2007. p. 858-61. [Google Scholar | PubMed]
- 10.Sharma S, Kalsotra N, Gupta P, Wani I, Singh M, Singh D. Solitary osteochondroma of the ilium: A case report. Int J Orthop Surg 2009;16:14. [Google Scholar | PubMed]
- 11.Sakamoto A, Tanaka K, Matsuda S, Harimaya K, Iwamoto Y. Vascular compression caused by solitary Osteochondroma: Useful diagnostic methods of magnetic resonance angiography and Doppler ultrasonography. J Orthop Sci 2002;7:439-43. [Google Scholar | PubMed]
- 12.Wood VE, Molitor C, Mudge MK. Hand involvement in multiple hereditary exostosis. Hand Clin 1990;6:685-92. [Google Scholar | PubMed]
- 13.Bottner F, Rodl R, Kordisg I, Winklemann W, Gosheger G, Lindner N. Surgical treatment of symptomatic osteochondroma. A three-to eight-year follow up study. J Bone Jt Surg Br 2003;85:1161-5. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 10, 2022 Solitary Osteochondroma of the Scapula in a Young Male: A Case Report
July 10, 2022 Solitary Osteochondroma of the Scapula in a Young Male: A Case Report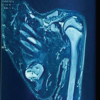 August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report
August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor