
Open Reduction and Internal Fixation is preferred in cases of Pediatric Isolated Coronoid fractures. It allows early mobilization of elbow and reduces chances of stiffness.
Dr. Ronak Khatri, Department of Orthopaedics, BLDEA’s Shri B M Patil Medical College and Hospital, Vijayapur, Karnataka, India. E-mail: ronakha3@gmail.com
Abstract
Introduction: Isolated coronoid fractures in the pediatric age group are uncommon and ill-defined in literature; here, we are studying the characteristics of the fracture and surgical management to gain good functional outcomes in such cases.
Case Report: A case of 9-year-old boy who presented with isolated right elbow coronoid displaced fracture Type IIIA of Regan and Morrey Classification, underwent open reduction internal fixation with headless screws and was followed up for 1-year postoperatively. A satisfactory functional outcome with full range of movement achieved with no complications at the final follow-up.
Conclusion: Headless screw fixation for Type IIIA coronoid fractures in pediatric elbow gives good functional outcome and range of movements with low rates of complications.
Keywords: Pediatric trauma, coronoid fracture, Herbert’s screw, pediatric elbow.
Coronoid fractures are usually associated with posterior dislocations of the elbow, which is uncommon in the pediatric population with an incidence of 3% as per the study of Henrikson [1]. Coronoid fractures occur in 2–15% of elbow dislocations making coronoid fractures uncommon injury in the pediatric population. Isolated coronoid fractures are rare in the pediatric population [1,2,3,4], and their description in the literature is unthorough; hence, here, we describe a case, its treatment aspects and outcomes. Regan and Morrey [5] classified coronoid fractures into three types (Fig. 1). Small fragments, that is, Type I that do not involve articular surfaces, can be treated conservatively; larger fragments, that is, Types II and III, which are intra-articular and block the elbow flexion, require fixation [4,6].
Here, we present a case of a male, aged 9 years, with history of injury over his right elbow due to a slip and fall with hand outstretched. The patient presented with complaints of pain over the elbow. On examination, swelling and tenderness were noted, and the range of motion was restricted, particularly elbow was in extension, and flexion was not possible. No neurovascular deficits were noted. The patient elbow was splinted in a comfortable position, and plain radiographs (Fig. 2) were taken in anteroposterior and lateral views, and the diagnosis was made as isolated right elbow coronoid displaced fracture Type IIIA of Regan and Morrey Classification. The patient was planned for operative treatment, and after all pre-operative examinations, the patient was taken under general anesthesia. Elbow was approached by the modified anteromedial approach for exposure of the coronoid [7], a curved “boat-race” incision centered over the elbow crease (Fig. 3) was followed by finding interval between brachial artery and median nerve to save recurrent radial artery. Coronoid was reached through this B-M interval for better exposure. The elbow was exposed after identifying all neurovascular structures and securing them with retractors. Fragment was reduced under direct vision. A 2.7 mm Herbert screw was put anteroposteriorly after a guide wire, and fixation was confirmed stable under fluoroscopy (Fig. 4).
The patient was planned for operative treatment, and after all pre-operative examinations, the patient was taken under general anesthesia. Elbow was approached by the modified anteromedial approach for exposure of the coronoid [7], a curved “boat-race” incision centered over the elbow crease (Fig. 3) was followed by finding interval between brachial artery and median nerve to save recurrent radial artery. Coronoid was reached through this B-M interval for better exposure. The elbow was exposed after identifying all neurovascular structures and securing them with retractors. Fragment was reduced under direct vision. A 2.7 mm Herbert screw was put anteroposteriorly after a guide wire, and fixation was confirmed stable under fluoroscopy (Fig. 4).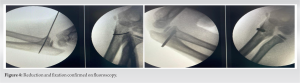 Screw was kept intentionally long (Figs. 4 and 5) keeping in mind easy implant removal from posterior approach as identifying anatomical neurovascular structures are difficult after index surgery. The wound was closed in layers, and the limb was immobilized in an above elbow slab, post-operative period went uneventful, sutures were removed on the 25 post-operative day and the slab after 4 weeks after the radiographic union was confirmed. Range of motion was restricted by 15° extension-lag and flexion up to 100° only, which was brought to normal at 2 months postoperatively (Fig. 6 and Video 1) by aggressive range of movement exercises; there were no restrictions noted in supination and pronation. The patient was followed up at 6 weeks, 3 months, 6 months, and 1 year. Our patient did not have any pain, and his elbow had a restored complete range of motion with a stable elbow joint at final follow-up after 1 year.
Screw was kept intentionally long (Figs. 4 and 5) keeping in mind easy implant removal from posterior approach as identifying anatomical neurovascular structures are difficult after index surgery. The wound was closed in layers, and the limb was immobilized in an above elbow slab, post-operative period went uneventful, sutures were removed on the 25 post-operative day and the slab after 4 weeks after the radiographic union was confirmed. Range of motion was restricted by 15° extension-lag and flexion up to 100° only, which was brought to normal at 2 months postoperatively (Fig. 6 and Video 1) by aggressive range of movement exercises; there were no restrictions noted in supination and pronation. The patient was followed up at 6 weeks, 3 months, 6 months, and 1 year. Our patient did not have any pain, and his elbow had a restored complete range of motion with a stable elbow joint at final follow-up after 1 year. 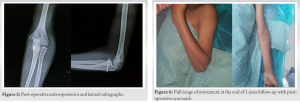 Implant removal was done at 1 year by approaching screw from posterior aspect. There was no episode of elbow subluxation or dislocation in follow-up period.
Implant removal was done at 1 year by approaching screw from posterior aspect. There was no episode of elbow subluxation or dislocation in follow-up period.
Isolated coronoid fractures are uncommon that too in the pediatric population, it is rare [4], making it rare to find references of these fractures treated surgically. It is pretty common to miss these fractures or misdiagnose in the pediatric population due to small fragments and the presence of cartilage. These injuries, especially Types II and III, if managed by closed reduction and casting or K-wiring, increase chances of non-union and recurrent dislocation due to unstable elbow. The elbow is prone to develop stiffness that too if intra-articular fractures are immobilized for a long period, certainly ends up in restricted elbow movements. Recommended idea to treat such fractures is by open reduction followed by rigid internal fixation with no step-off at the articular surface. In our study, a case of a male, aged 9 years, with history of an injury over his the right elbow due to slip and fall with hand outstretched. He was operated by open reduction internal fixation by Herbert’s screw and was followed up clinically and radiologically for 1 year. Arnold and Fehringer [8] in their study included a case of a 7-year-old male child who had a history of stairwell fall. They used a posterior approach to the elbow and fixed the reduced fragment with a K-wire, and the elbow was stabilized with a hinged external fixator to distract the humeroulnar joint. The patient was advised range of movement from the 1st post-operative day. They followed the case for 5 months. Godin et al. [9] reported a case of a coronoid fracture associated with the elbow posterior dislocation (Type IIIB) in a 7-year-old girl, who sustained trauma to her elbow by fall from a trampoline. The anteromedial approach was used, open reduction of elbow and coronoid fragment was done. Internal fixation by K-wiring was done and immobilized in a cast. The cast and wires were removed at 4 weeks postoperatively. We received satisfactory results and full range of motion at 2 months postoperatively. No neurovascular injuries, instability or stiffness, were noted in our case. In Arnold and Fehringer [8]’s case, the external fixator was removed at 4 weeks, and the K-wire at 3 months. The range of motion achieved normal by the 5th post-operative month. No neurovascular injury or instability was noted. In study of Godin et al. [9] no neurovascular deficits were noted, range of movement after cast and K-wire removal at 1 month was 20–90°.
Open reduction-internal fixation in coronoid fractures is a reliable method for fixation with low chances of complications. It can be considered as the treatment of choice for Type III coronoid fractures. It allows early movement at the elbow joint lowering the chances of joint stiffness, which is the most common complication after fractures around the elbow.
Keen examination, early diagnosis, and adequate treatment with open reduction-internal fixation in coronoid fractures give good functional outcomes in cases of pediatric Type III coronoid fractures.
References
- 1.Henrikson B. Supracondylar fracture of the humerus in children. A late review of end-results with special reference to the cause of deformity, disability and complications. Acta Chir Scand Suppl 1966;369:1-72. [Google Scholar | PubMed]
- 2.Regan W, Morrey B. Fractures of the coronoid process of the ulna. J Bone Joint Surg Am 1989;71:1348-54. [Google Scholar | PubMed]
- 3.Carlioz H, Abols Y. Posterior dislocation of the elbow in children. J Pediatr Orthop 1984;4:8-12. [Google Scholar | PubMed]
- 4.Selesnick FH, Dolitsky B, Haskell SS. Fracture of the coronoid process requiring open reduction with internal fixation. A case report. J Bone Joint Surg Am 1984;66:1304-6. [Google Scholar | PubMed]
- 5.Regan W, Morrey BF. Classification and treatment of coronoid process fractures. Orthopedics 1992;15:845-8. [Google Scholar | PubMed]
- 6.Hanks GA, Kottmeier SA. Isolated fracture of the coronoid process of the ulna: A case report and review of the literature. J Orthop Trauma 1990;4:193-6. [Google Scholar | PubMed]
- 7.Yang F, Feng K, Sun Y, Dai K, Wang X, Tang J. A modified anteromedial approach for exposure of coronoid fractures: An anatomical cadaver study. Biomed Res Int 2019;2019:6872948. [Google Scholar | PubMed]
- 8.Arnold RM, Fehringer EV. Displaced basal coronoid fracture and fixation in a 7 year old: A case report and review of the literature. Shoulder Elbow 2009;1:104-7. [Google Scholar | PubMed]
- 9.Godin JA, Tainter DM, Klement MR, Alman BA, Grier AJ, Templeton EL, et al. Incarcerated coronoid fracture at the time of pediatric elbow dislocation. Duke Orthop J 2018;8:22-7. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Generalized Tetanus Following Traditional Manipulation of an Open Supracondylar Humerus Fracture in a Child: A Rare Case Report
August 1, 2026 Generalized Tetanus Following Traditional Manipulation of an Open Supracondylar Humerus Fracture in a Child: A Rare Case Report August 1, 2026 The “Terrible Tetrad” of the Elbow: A Case Series of Two Patients with a Rare Quadruple-Component Injury and a Proposed New Classification Term
August 1, 2026 The “Terrible Tetrad” of the Elbow: A Case Series of Two Patients with a Rare Quadruple-Component Injury and a Proposed New Classification Term January 1, 2026 Successful Thumb Replantation Following Dog Bite Avulsion Amputation in a 2-Year-Old Child: A Case Report and Literature Review
January 1, 2026 Successful Thumb Replantation Following Dog Bite Avulsion Amputation in a 2-Year-Old Child: A Case Report and Literature Review October 1, 2025 A Unique Case of Bilateral Elbow Terrible Triad in a Polytrauma Patient: Associated Challenges in Management
October 1, 2025 A Unique Case of Bilateral Elbow Terrible Triad in a Polytrauma Patient: Associated Challenges in Management