
Non-classical Celiac disease is an underdiagnosed condition with many non-specific symptoms and known cutaneous manifestations, and it should be considered in the work-up of refractory post-operative skin complications.
Dr. Vikranth Mirle, Midwest Orthopedics at Rush, Rush University Medical Center, Chicago, Illinois, USA. E-mail: vikranthmirle@uchicagomedicine.org
Abstract
Introduction: Non-classical Celiac disease is a previously undescribed cause of debilitating post-operative cutaneous complications following an orthopedic procedure. Non-specific symptoms and rarity of the disease pose a diagnostic challenge; however, given underdiagnosis and significant morbidity, after ruling out of acute pathology, Celiac disease should be included in differential diagnosis for refractory cutaneous complications following an operative procedure.
Case Report: A 34-year-old woman who underwent patellofemoral arthroplasty and medial patellofemoral ligament reconstruction experienced over 5 months of post-operative knee swelling, erythema, and pain unresponsive to antihistamines and negative infectious, vascular, and implant allergy testing workups. After careful dietary monitoring by an allergy specialist, she was tested and confirmed to have Celiac disease. Following cessation of her oral contraceptive pill and dietary gluten, her knee swelling, erythema, and debilitating pain resolved.
Conclusion: Skin erythema, swelling, and pain are known complications after any operative treatment, but after ruling out of acute infectious and thromboembolic processes, diagnosis and management of refractory complications pose a challenging scenario. In this rare phenomenon, previously undescribed, a patient presented with months of post-operative knee erythema, swelling, stiffness, and extreme pain on activity along with non-specific symptoms of headache and fatigue before diagnosis with Celiac disease. On cessation of her birth control and dietary gluten, her symptoms and knee function improved dramatically.
Keywords: Knee arthroplasty complication, celiac disease, medial patellofemoral reconstruction, patellofemoral arthroplasty, autoimmune disease.
Patellofemoral arthroplasty (PFA) has emerged as a viable tool in the surgical management of isolated patellofemoral arthritic conditions. Refinement in patient selection and advancements in implant design and surgical technique have resulted in improved implant performance and patient satisfaction [1,2,3]. However, post-operative stiffness and swelling is an uncommon, but frustrating complication following knee surgery, including PFA. The differential diagnosis for post-surgical swelling is broad. While extended post-operative pain, erythema, stiffness, and swelling are most concerning for an infectious etiology, a multitude of other etiologies, including thromboembolism and allergy-related complications, may be considered once an infection has been excluded from the study [4,5]. Even more rare, genetic causes include mastocytosis and hereditary angioedema. Celiac disease is an autoimmune enteropathic disorder that classically affects the small intestine in response to dietary gluten sensitivity. With an estimated prevalence of 1% in the population, Celiac disease has garnered significant public attention over the last few decades [6]. However, non-classical Celiac disease is an underdiagnosed disorder with numerous cutaneous manifestations, including dermatitis herpetiformis, erythema nodosum, urticaria, and atopic dermatitis [7]. To the best of our knowledge, a cutaneous manifestation of non-classical Celiac disease following an orthopedic surgical procedure has not been reported previously. We report the case of a patient who developed refractory right knee swelling, pain, and erythema following combined PFA and medial patellofemoral ligament reconstruction (MPFLR) reconstruction. The patient’s symptoms were determined ultimately to be secondary to a non-classical form of Celiac disease, and her symptoms resolved expeditiously following discontinuation of gluten intake. The patient was informed that data concerning her case would be submitted for publication, and she provided consent.
A 34-year-old female presented to clinic with an extensive history of right knee pain and patellar instability. The patient experienced three patellar dislocations as a high school student, all of which were treated nonoperatively. She endorsed intermittent anterior knee pain subsequently, which became progressive approximately 5 years before presentation. At the time of initial presentation in our clinic, her numeric rating pain scale ranged from 5 to 10/10. Physical examination was significant for a trace intra-articular effusion, a positive J sign, positive Clarke’s test, and positive patellar apprehension with passive lateral translation. Magnetic resonance imaging (MRI) demonstrated a laterally subluxated patella and significant patellofemoral osteoarthritis. Given the patient’s persistent knee pain and patellar instability, the patient was indicated for an initial diagnostic knee arthroscopy. During initial diagnostic knee arthroscopy, evaluation of the patellofemoral compartment confirmed lateral patellar subluxation and Outerbridge Grade 4 chondrosis of the medial and lateral patella facets. Based on these findings, the patient was indicated for a subsequent right knee patellofemoral resurfacing with concomitant MPFLR. On return to the operating room 7 weeks later, the patient was placed supine on the operating table, and a standard PFA was performed. Briefly, a 12 cm longitudinal midline incision was made on the anterior aspect of the right knee. Following a medial peripatellar arthrotomy, the patient’s trochlea was sized, prepared, and a 5 × 8.5 25 mm trochlear prosthesis and a 25 mm patellar button were implanted (PF Wave Implant System, Anika, Bedford, MA). After standard closure of the patellar arthrotomy, attention was turned to MPFLR. A 2.5 cm incision at the junction of the proximal one-third and distal two-thirds of the medial border of the patella was made for the MPFLR. A guidepin was placed at Shottle’s point under lateral radiography. The tibialis anterior allograft was then implanted on the femoral side with a 6.25 mm × 15 mm PEEK tenodesis screw and on the patellar side with two 2.4 PEEK suturetaks and four #4 FiberWire sutures. Following imbrication utilizing 0-Vicryl suture, the subcutaneous tissue and skin were closed in a layered fashion. At 4-week postoperatively, the patient noted an erythematous rash encompassing the arthrotomy incision. During this same period, she noticed increased knee stiffness, warmth, and swelling. On examination, her right knee had a trace effusion with range of motion (ROM) limited to 0–30°. The skin surrounding the knee was erythematous with mild urticaria, warm, blanchable, non-tender, and without edema. An outline of the redness was marked on her leg for comparison, and she was instructed to return to clinic in 2 days for repeat examination. In addition, the patient was started on a 7-day course of Bactrim with concern for a skin and soft-tissue infection. On return to clinic, the patient endorsed increasing pain and no change in erythema. She denied any systemic symptoms including fevers or chills. The patient’s vital signs remained stable, and examination was significant for newfound tenderness to palpation along the medial and lateral aspect of the joint line. The skin remained erythematous within previous boundary. The skin was warm and blanchable with no palpable edema. Mild intra-articular effusion remained. Neurovascular examination was intact, and the incision sites were well-healed and benign. Given persistent urticaria and erythema, the patient was referred to the emergency department (ED) for possible cellulitis or allergic reaction. In the ED, the patient was started on intravenous diphenhydramine and vancomycin before admission. During her admission, inflammatory markers and MRI were negative for infection with subjective improvement of erythema, urticaria, and swelling. The patient was discharged after 2 days with oral diphenhydramine and topical clabetasol with follow-up in clinic. Over post-operative week 7 through week 21, the patient continued to experience worsening of symptoms during activity including warmth and swelling around her knee, a reticular rash across the limb, and throbbing pain rated 10/10 (Fig. 1-3).  She experienced significant decline in ability to maintain independent activities of daily living. At week 14, she was seen in the ED for worsening symptoms including fatigue and headaches. Following negative infectious and thromboembolic workup in the ED, she was referred to outpatient allergy and vascular surgery.
She experienced significant decline in ability to maintain independent activities of daily living. At week 14, she was seen in the ED for worsening symptoms including fatigue and headaches. Following negative infectious and thromboembolic workup in the ED, she was referred to outpatient allergy and vascular surgery. She was seen by allergy specialists with concern for implant allergy, mastocytosis, and angioedema, and by vascular surgery for possible May-Thurner and popliteal entrapment syndrome. Advanced imaging including lower extremity MRI with angiography and abdominopelvic CT with contrast demonstrated patent vasculature. Patch testing was negative. Similarly, blood levels of C4 complement and tryptase were within normal limits. On further investigation, the patient reported recent onset intermittent sensations of bloating in addition to the fatigue and headaches. Consequently, the allergy team recommended maintenance of a rigorous food diary before pursuing further testing. The patient returned to the orthopedic surgery clinic at 22-week postoperatively. She expressed that after further visits with the allergy and gastroenterology clinic, she had been diagnosed with Celiac disease. After diet modifications, she expressed mild-to-moderate improvement in swelling with no change in pain during activity. The patient returned to clinic at 26-week postoperatively and reported that the allergy clinic had concluded her gluten allergy was likely related to a prescribed oral contraceptive pill (OCP). After elimination of the OCP and continued avoidance of gluten in her diet, the patient experienced rapid improvement in symptoms. On examination, the patient had ROM from 5° hyperextension to full flexion with normal skin findings of the knee (Fig. 4).
She was seen by allergy specialists with concern for implant allergy, mastocytosis, and angioedema, and by vascular surgery for possible May-Thurner and popliteal entrapment syndrome. Advanced imaging including lower extremity MRI with angiography and abdominopelvic CT with contrast demonstrated patent vasculature. Patch testing was negative. Similarly, blood levels of C4 complement and tryptase were within normal limits. On further investigation, the patient reported recent onset intermittent sensations of bloating in addition to the fatigue and headaches. Consequently, the allergy team recommended maintenance of a rigorous food diary before pursuing further testing. The patient returned to the orthopedic surgery clinic at 22-week postoperatively. She expressed that after further visits with the allergy and gastroenterology clinic, she had been diagnosed with Celiac disease. After diet modifications, she expressed mild-to-moderate improvement in swelling with no change in pain during activity. The patient returned to clinic at 26-week postoperatively and reported that the allergy clinic had concluded her gluten allergy was likely related to a prescribed oral contraceptive pill (OCP). After elimination of the OCP and continued avoidance of gluten in her diet, the patient experienced rapid improvement in symptoms. On examination, the patient had ROM from 5° hyperextension to full flexion with normal skin findings of the knee (Fig. 4). There was no effusion or interstitial swelling, and the patient demonstrated 5/5 hip abductor and quadricep strength. At 6 months, comparison to pre-operative PROs demonstrated an improvement of 9.4 points in International Knee Documentation Committee (IKDC) and 14.7 points in Knee Injury and Osteoarthritis Outcomes Score, Joint Replacement scores. Improvement in IKDC score met criteria for minimal clinically important difference [8]. The patient’s final clinic visit was 1-year postoperatively where she continued to progress well with no recurrences of swelling, pain, or erythema.
There was no effusion or interstitial swelling, and the patient demonstrated 5/5 hip abductor and quadricep strength. At 6 months, comparison to pre-operative PROs demonstrated an improvement of 9.4 points in International Knee Documentation Committee (IKDC) and 14.7 points in Knee Injury and Osteoarthritis Outcomes Score, Joint Replacement scores. Improvement in IKDC score met criteria for minimal clinically important difference [8]. The patient’s final clinic visit was 1-year postoperatively where she continued to progress well with no recurrences of swelling, pain, or erythema.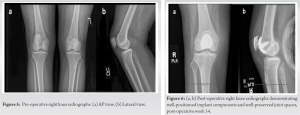
Refractory post-operative skin changes, swelling, and pain without other systemic signs are a challenging entity and have a wide differential diagnosis once acute infection and allergic reaction have been ruled out. 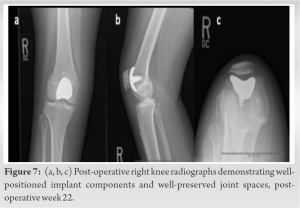 The patient described in this case report experienced months of debilitating knee swelling, erythema, and pain with normal radiographs (Fig. 5-7) unresponsive to antihistamines and negative infectious, vascular, and implant allergy testing workups (Fig. 8).
The patient described in this case report experienced months of debilitating knee swelling, erythema, and pain with normal radiographs (Fig. 5-7) unresponsive to antihistamines and negative infectious, vascular, and implant allergy testing workups (Fig. 8). 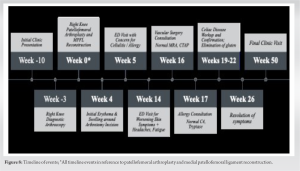 After careful dietary monitoring by an allergy specialist, she was tested and confirmed to have celiac disease. Following cessation of her OCP and dietary gluten, her knee swelling, erythema, and pain significantly improved. The potential etiologies of post-operative lower extremity pain following orthopedic surgery can be both broad and multifactorial. When more common diagnoses such as infection, venous thromboembolism, and hemarthroses are excluded, other less common etiologies require careful investigation. In reviewing complications of PFA, Familiari et al. demonstrate that infection, pain, and progression of arthritis in other compartments constitute a vast majority of complications [1]. In the case of MPFLR, Shah et al. conducted a systematic review of 629 reconstructions with an overall 164 complications (26.1%) with 13 (2%) wound complications [5]. Of these wound complications, 12 comprised of dehiscence, infection, or hematoma. Thus, the symptomatology of our patient represents a rare entity in the complications after PFA and MPFLR. A related but unavoidable aspect in delay of diagnosis is the urgency of thromboembolic and infectious complications leading to the patient receiving multiple MRIs, CT scans, and other imaging before significant allergy workup. Another consideration in diagnosis was the patient’s remote history of nickel allergy with eventual negative workup. Pacheco reported that implant allergy is one of the least considered causes of complications after arthroplasty and review the materials and incidence of implant allergy with nickel, cobalt, chromium, and bone cement being the most common culprits [9]. Granchi et al. demonstrated that total knee arthroplasty failure risk is increased fourfold in patients with pre-operative metal sensitivity [10]. While patch testing was negative in this patient, implant allergy is important in pre-operative and post-operative consideration for arthroplasty. The key challenge in diagnosis of Celiac disease as the underlying cause in this case was the presence of cutaneous symptoms unassociated with the disease and the absence of classical findings, such as prominent gastrointestinal symptoms and weight loss. Celiac disease is a T-cell mediated autoimmune enteropathy with an average prevalence around 1%. Celiac disease pathogenesis is multifactorial, including genetic, dietary, environment, and gut microbiome triggers. Both classical and non-classical forms can onset following an environmental gluten trigger, and in this patient, a culprit suggested was a newly started OCP [11]. As to clinical presentation, there numerous well-documented and well-studied intestinal and extra-intestinal manifestations. Rodrigo et al. review cutaneous and mucosal manifestations affected by gluten intake as including dermatitis herpetiformis, urticaria, atopic dermatitis, rosacea, and erythema nodosum among others [7]. In children, the classical form commonly presents with chronic diarrhea, weight loss, and poor appetite; however, in adults, the most common form is non-classical disease [6]. Non-classical disease commonly presents with non-specific complaints including mild and intermittent symptoms of fatigue, bloating, and abdominal discomfort. The generalized nature of these complains can render diagnosis difficult and likely contributes to the underdiagnosis of the disease [12]. As demonstrated in this patient, these non-specific symptoms necessitate a low threshold for further investigation. To the best of our knowledge, this case study represents the first report of an orthopedic surgical complication associated with a new diagnosis of non-classical celiac disease. Further, there is a paucity of literature examining the effect of celiac disease on outcomes following orthopedic surgery. In the lone published study, Cole et al. demonstrated significantly higher rates of myocardial infarctions and peri-prosthetic fractures following total hip arthroplasty among patients with celiac disease [13]. Given that as many as 70% of cases are undiagnosed with serious ramifications for untreated disease, [14] further research is imperative to understand the impact of celiac disease on pathogenesis of orthopedic conditions and outcomes of operative treatment.
After careful dietary monitoring by an allergy specialist, she was tested and confirmed to have celiac disease. Following cessation of her OCP and dietary gluten, her knee swelling, erythema, and pain significantly improved. The potential etiologies of post-operative lower extremity pain following orthopedic surgery can be both broad and multifactorial. When more common diagnoses such as infection, venous thromboembolism, and hemarthroses are excluded, other less common etiologies require careful investigation. In reviewing complications of PFA, Familiari et al. demonstrate that infection, pain, and progression of arthritis in other compartments constitute a vast majority of complications [1]. In the case of MPFLR, Shah et al. conducted a systematic review of 629 reconstructions with an overall 164 complications (26.1%) with 13 (2%) wound complications [5]. Of these wound complications, 12 comprised of dehiscence, infection, or hematoma. Thus, the symptomatology of our patient represents a rare entity in the complications after PFA and MPFLR. A related but unavoidable aspect in delay of diagnosis is the urgency of thromboembolic and infectious complications leading to the patient receiving multiple MRIs, CT scans, and other imaging before significant allergy workup. Another consideration in diagnosis was the patient’s remote history of nickel allergy with eventual negative workup. Pacheco reported that implant allergy is one of the least considered causes of complications after arthroplasty and review the materials and incidence of implant allergy with nickel, cobalt, chromium, and bone cement being the most common culprits [9]. Granchi et al. demonstrated that total knee arthroplasty failure risk is increased fourfold in patients with pre-operative metal sensitivity [10]. While patch testing was negative in this patient, implant allergy is important in pre-operative and post-operative consideration for arthroplasty. The key challenge in diagnosis of Celiac disease as the underlying cause in this case was the presence of cutaneous symptoms unassociated with the disease and the absence of classical findings, such as prominent gastrointestinal symptoms and weight loss. Celiac disease is a T-cell mediated autoimmune enteropathy with an average prevalence around 1%. Celiac disease pathogenesis is multifactorial, including genetic, dietary, environment, and gut microbiome triggers. Both classical and non-classical forms can onset following an environmental gluten trigger, and in this patient, a culprit suggested was a newly started OCP [11]. As to clinical presentation, there numerous well-documented and well-studied intestinal and extra-intestinal manifestations. Rodrigo et al. review cutaneous and mucosal manifestations affected by gluten intake as including dermatitis herpetiformis, urticaria, atopic dermatitis, rosacea, and erythema nodosum among others [7]. In children, the classical form commonly presents with chronic diarrhea, weight loss, and poor appetite; however, in adults, the most common form is non-classical disease [6]. Non-classical disease commonly presents with non-specific complaints including mild and intermittent symptoms of fatigue, bloating, and abdominal discomfort. The generalized nature of these complains can render diagnosis difficult and likely contributes to the underdiagnosis of the disease [12]. As demonstrated in this patient, these non-specific symptoms necessitate a low threshold for further investigation. To the best of our knowledge, this case study represents the first report of an orthopedic surgical complication associated with a new diagnosis of non-classical celiac disease. Further, there is a paucity of literature examining the effect of celiac disease on outcomes following orthopedic surgery. In the lone published study, Cole et al. demonstrated significantly higher rates of myocardial infarctions and peri-prosthetic fractures following total hip arthroplasty among patients with celiac disease [13]. Given that as many as 70% of cases are undiagnosed with serious ramifications for untreated disease, [14] further research is imperative to understand the impact of celiac disease on pathogenesis of orthopedic conditions and outcomes of operative treatment.
Skin erythema, swelling, and pain are known complications after any operative treatment, but after ruling out of acute infectious and thromboembolic processes, diagnosis and management of refractory complications pose a challenging scenario. In this rare phenomenon, previously undescribed, a patient presented with months of post-operative knee erythema, swelling, stiffness, and extreme pain on activity along with non-specific symptoms of headache and fatigue before diagnosis with Celiac disease. On cessation of her birth control and dietary gluten, her symptoms and knee function improved dramatically.
Post-operative skin erythema, swelling, and pain pose a challenging diagnostic scenario after ruling out of acute pathology including infectious, vascular, and acute allergy. In this case report, we demonstrate a previously undescribed phenomenon of non-classical Celiac disease as a cause of debilitating post-operative complications following a patellofemoral arthroplasty and medial patellofemoral reconstruction. Given the underdiagnosis and significant morbidity of celiac disease and autoimmune diseases in general, they are important to be included in the differential diagnosis of refractory post-operative complications after ruling out acute etiologies.
References
- 1.Familiari F, Madonna V, Mercurio M, Cinque ME, Gasparini G, Galasso O, et al. Outcomes and complications of inlay versus onlay patellofemoral arthroplasty: A systematic review. Knee 2023;41:124-36. [Google Scholar | PubMed]
- 2.Strickland SM, Bird ML, Christ AB. Advances in patellofemoral arthroplasty. Curr Rev Musculoskelet Med 2018;11:221-30. [Google Scholar | PubMed]
- 3.Li C, Li Z, Shi L, Gao F, Sun W. The short-term effectiveness and safety of second-generation patellofemoral arthroplasty and total knee arthroplasty on isolated patellofemoral osteoarthritis: A systematic review and meta-analysis. J Orthop Surg Res 2021;16:358. [Google Scholar | PubMed]
- 4.Bohensky MA, deSteiger R, Kondogiannis C, Sundararajan V, Andrianopoulos N, Bucknill A, et al. Adverse outcomes associated with elective knee arthroscopy: A population-based cohort study. Arthroscopy 2013;29:716-25. [Google Scholar | PubMed]
- 5.Shah JN, Howard JS, Flanigan DC, Brophy RH, Carey JL, Lattermann C. A systematic review of complications and failures associated with medial patellofemoral ligament reconstruction for recurrent patellar dislocation. Am J Sports Med 2012;40:1916-23. [Google Scholar | PubMed]
- 6.Catassi C, Verdu EF, Bai JC, Lionetti E. Coeliac disease. Lancet 2022;399:2413-26. [Google Scholar | PubMed]
- 7.Rodrigo L, Beteta-Gorriti V, Alvarez N, Gómez de Castro C, de Dios A, Palacios L, et al. Cutaneous and mucosal manifestations associated with celiac disease. Nutrients 2018;10:800. [Google Scholar | PubMed]
- 8.Walsh JM, Huddleston HP, Alzein MM, Wong SE, Forsythe B, Verma NN, et al. The minimal clinically important difference, substantial clinical benefit, and patient-acceptable symptomatic state after medial patellofemoral ligament reconstruction. Arthrosc Sports Med Rehabil 2022;4:e661-78. [Google Scholar | PubMed]
- 9.Pacheco KA. Allergy to surgical implants. Clin Rev Allergy Immunol 2019;56:72-85. [Google Scholar | PubMed]
- 10.Granchi D, Cenni E, Trisolino G, Giunti A, Baldini N. Sensitivity to implant materials in patients undergoing total hip replacement. J Biomed Mater Res B Appl Biomater 2006;77:257-64. [Google Scholar | PubMed]
- 11.Research C for DE and. Medications and Gluten. FDA. Published online; 09 February, 2019. Available from: https://www.fda.gov/drugs/ensuring-safe-use-medicine/medications-and-gluten. [Last accessed on 2023 Feb 07]. [Google Scholar | PubMed]
- 12.Elwenspoek MM, Thom H, Sheppard AL, Keeney E, O'Donnell R, Jackson J, et al. Defining the optimum strategy for identifying adults and children with coeliac disease: Systematic review and economic modelling. Health Technol Assess 2022;26:1-310. [Google Scholar | PubMed]
- 13.Cole MW, Ross BJ, Collins LK, Imonugo O, Sherman WF. The impact of celiac disease on complication rates after total joint arthroplasty: A matched cohort study. Arthroplast Today 2022;17:205-10.e3. [Google Scholar | PubMed]
- 14.Gatti S, Lionetti E, Balanzoni L, Verma AK, Galeazzi T, Gesuita R, et al. Increased prevalence of celiac disease in school-age children in Italy. Clin Gastroenterol Hepatol 2020;18:596-603. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 May 10, 2023 Robotic-Assisted Patellofemoral Arthroplasties Following Failed Treatment for Trochlear Dysplasia and Patellar Instability: A Case Report
May 10, 2023 Robotic-Assisted Patellofemoral Arthroplasties Following Failed Treatment for Trochlear Dysplasia and Patellar Instability: A Case Report November 19, 2011 Juxtaphyseal Intraosseous Hemangioma of Proximal Femur causing coxa vara andcoxa breva deformity in a growing child: a Case Report
November 19, 2011 Juxtaphyseal Intraosseous Hemangioma of Proximal Femur causing coxa vara andcoxa breva deformity in a growing child: a Case Report March 1, 2025 Joint Reconstruction using Tricortical Iliac Crest Bone Graft Block for Intra-Articular Extension of Aneurysmal Bone Cyst of Distal Tibia in a Skeletally Mature Patient – A Case Report and Review of Literature
March 1, 2025 Joint Reconstruction using Tricortical Iliac Crest Bone Graft Block for Intra-Articular Extension of Aneurysmal Bone Cyst of Distal Tibia in a Skeletally Mature Patient – A Case Report and Review of Literature December 1, 2025 A Prospective Study Comparing the Functional Outcomes of Complex Tibial Plateau Fractures Using Computed Tomography-based Three-column Theory Versus X-Ray-based Schatzker Classification Treated with Open Reduction with Locking Compression Plates
December 1, 2025 A Prospective Study Comparing the Functional Outcomes of Complex Tibial Plateau Fractures Using Computed Tomography-based Three-column Theory Versus X-Ray-based Schatzker Classification Treated with Open Reduction with Locking Compression Plates