
Osteoid osteoma of the phalanges is uncommon and should always be included as differential in chronic foot pain with nocturnal predominance as the prognosis post-treatment is excellent.
Dr. M L V Sai Krishna, Consultant, Department of Orthopaedics, Aayush Hospitals, Eluru, India. Email: krishna.mlv.sai@gmail.com.
Abstract
Introduction: Osteoid osteoma is a common benign osteoblastic lesion of the bone. Although it commonly affects the cortex of long bones, it rarely involves the cancellous portion of the small bones such as phalanges. The occurrence of osteoid osteoma in phalanges poses a diagnostic dilemma.
Case Report: In our case report, we presented a 26-year-old patient with long-standing pain over the great toe. The radiographs and magnetic resonance imaging (MRI) were unable to diagnose the lesion, and a single-photon emission computerized tomography scan picked up the nidus. She underwent radiofrequency ablation and post-procedure she was relieved of her symptoms.
Conclusion: Osteoid osteoma of the phalanges is uncommon, and at times, routine radiographs and MRIs might not point us to the correct diagnosis. As the prognosis is excellent after the treatment is instituted, osteoid osteoma should always be a differential in chronic foot pain with nocturnal predominance.
Keywords: Osteoid osteoma, chronic foot pain, radio frequency ablation.
Osteoid osteoma is a common benign osteoblastic lesion of the bone. It accounts for 10–12% of benign bone tumors, and its incidence in affecting the foot and hallux is 2% [1,2]. It commonly affects the cortex of the long bones. The characteristic feature is a nidus, which is a radiolucent area surrounded by reactive sclerosis. The symptoms include worsening night pain, which responds to nonsteroidal anti-inflammatory drugs (NSAIDs). The occurrence of osteoid osteoma in the phalanges of toes is uncommon, and only a few such reports have been described in the literature. It even poses a diagnostic challenge because of its varied presentation [1-12]. We presented in our case report one such osteoid osteoma of the great toe.
A 26-year-old female presented to us with a complaint of pain over the right foot great toe for 6 years. She was already evaluated for hyperuricemia and inflammatory arthritis, and for both of them, she tested negative. She was taking over-the-counter painkillers for a long time, in an on-and-off manner. Despite the usage of painkillers, she never had complete relief from pain, which hampered her day-to-day life and affected her daily living. When she presented to us, we re-evaluated her and took a detailed history. Her history revealed that she used to have mid-night pain or late-night pain; for the same, she was taking NSAID, which gave her relief but not complete, and she was taking the same on and off for the past 6 years. On examination, she had tenderness over the proximal phalanx of the great toe. There was no erythema and swelling (Fig. 1). The nail bed and nails were fine. Serum chemistry markers erythrocyte sedimentation rate, and serum C-reactive protein levels were normal. The patient underwent radiographs (Fig. 2) of the foot, which showed a benign, purely lytic lesion in the great toe proximal phalanx with no periosteal reaction or joint involvement. The non-contrast computerized tomography (Fig. 3) of the foot showed an eccentric circumscribed lytic lesion (nidus) 5–6 mm in the first proximal phalange with a surrounding sclerotic rim.
The nail bed and nails were fine. Serum chemistry markers erythrocyte sedimentation rate, and serum C-reactive protein levels were normal. The patient underwent radiographs (Fig. 2) of the foot, which showed a benign, purely lytic lesion in the great toe proximal phalanx with no periosteal reaction or joint involvement. The non-contrast computerized tomography (Fig. 3) of the foot showed an eccentric circumscribed lytic lesion (nidus) 5–6 mm in the first proximal phalange with a surrounding sclerotic rim. 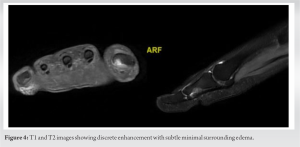 The magnetic resonance imaging (MRI) (Fig. 4) revealed a corresponding circumscribed T1 iso to hypointense/T2 hyperintense lesion at the first proximal phalange, showing discrete enhancement with subtle minimal surrounding edema. Adjacent distal interphalangeal joint shows minimal joint effusion with normal soft tissue, bones, and tendons. On single-photon emission computerized tomography (SPECT), there was a focal area of increased radiotracer uptake with central nidus with an adjacent region of halo with peripheral sclerosis noted in the computed tomography (CT) in the posterior aspect of the shaft of the first proximal phalanx of the right foot suggestive of osteoid osteoma (Fig. 5). The patient underwent CT-guided radiofrequency ablation (RFA) (Fig. 6) for osteoid osteoma. An 11G bone biopsy needle was used through which 18G probe needle was inserted.
The magnetic resonance imaging (MRI) (Fig. 4) revealed a corresponding circumscribed T1 iso to hypointense/T2 hyperintense lesion at the first proximal phalange, showing discrete enhancement with subtle minimal surrounding edema. Adjacent distal interphalangeal joint shows minimal joint effusion with normal soft tissue, bones, and tendons. On single-photon emission computerized tomography (SPECT), there was a focal area of increased radiotracer uptake with central nidus with an adjacent region of halo with peripheral sclerosis noted in the computed tomography (CT) in the posterior aspect of the shaft of the first proximal phalanx of the right foot suggestive of osteoid osteoma (Fig. 5). The patient underwent CT-guided radiofrequency ablation (RFA) (Fig. 6) for osteoid osteoma. An 11G bone biopsy needle was used through which 18G probe needle was inserted.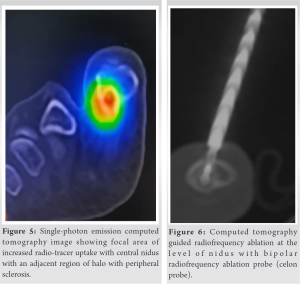 9 mm active tip bipolar RFA probe (Celon probe) used, and 0.5 KJ energy deposited at nidus. On follow-up, sequential radiographs were taken at 3 months and 1 year following intervention with no recurrence of symptoms.
9 mm active tip bipolar RFA probe (Celon probe) used, and 0.5 KJ energy deposited at nidus. On follow-up, sequential radiographs were taken at 3 months and 1 year following intervention with no recurrence of symptoms.
Osteoid osteoma affecting the toes of the foot is rather uncommon. In long bones, the site of predilection is the cortex, whereas in small bones of the foot, it affects the cancellous portion and has unique and varied clinical and radiological features. In our patient, the radiographs and MRI findings gave us the impression of a focal cortical defect/nonossifying fibroma, which falls under the category of do not touch lesion, but the patient’s long-term severe midnight toe pain history made us think again, and the patient was further evaluated on SPECT imaging. Trave et al. [1] presented a patient with pain in the toes, which was initially treated as osteomyelitis but with no resolution in symptoms and later diagnosed as osteoid osteoma and treated accordingly. Osteoid osteoma of the foot can have symptoms of local warmth and swelling with erythema, with more suspicion of an infectious etiology due to its involvement of cancellous bone in the phalanges with thin soft tissue coverage [1]. Seo et al. [2] in their case report also presented a pediatric patient with chronic foot pain due to osteoid osteoma. Such presentation of osteoid osteoma at an atypical location results in challenging differentials, more so in favor of osteomyelitis or abscess. Any patient with chronic foot pain having nocturnal predominance and relief with NSAIDs should always have osteoid osteoma in its differentials [1-12]. Turkmen et al. [3] and Jowett and Singh et al. [4] also in their reports emphasized the diagnostic dilemma an osteoid osteoma can pose when presented in an atypical location like phalanges. Osteoma of the short bones of the foot presents as a painful swelling, which is the not scenario of the long bones. The swelling tends to have all the characteristic features of inflammation. This results in delayed diagnosis, and at times, the imaging is also ambiguous resulting in further delay of the diagnosis [5-7]. Even in our patient, the radiograph and MRI were not suggestive of osteoid osteoma; the patient’s nocturnal characteristic pain with relief after NSAIDs prompted us to go for further imaging. For any patient with chronic foot pain where the differential of osteoid osteoma is made due to the worsening night pain and relief with NSAID, even though the imaging with radiographs and MRI is unambiguous when in doubt, a histopathology or a nuclear medicine imaging helps. The prognosis with appropriate diagnosis and treatment is excellent [8,9]. In the few case reports that discussed patients with an osteoid osteoma of the toes, many authors have attributed the delay in diagnosis due to the unusuality of the location and ambiguous radiological findings [1-12]. Although the patient’s demography, pain pattern, and radiological features do not meet the classic definition of osteoid osteoma, it should always be included in the differentials of chronic foot pain.
Osteoid osteoma of the phalanges is uncommon, and at times, routine radiographs and MRIs might not point us to the correct diagnosis. In our patient, the long-standing history and nocturnal occurrence of pain and relief with NSAIDs and SPECT imaging guided us toward the diagnosis. As the prognosis is excellent after the treatment is instituted, osteoid osteoma should always be a differential in chronic foot pain with nocturnal predominance.
Osteoid osteoma should always be included in the differentials of chronic foot pain, and further investigations with nuclear imaging or biopsy is necessary for a definitive diagnosis as once the treatment is instituted, the prognosis is excellent.
References
- 1.Trave I, Chiarlone F, Barabino G, Parodi A. Osteoid osteoma of the great toe: Dermatological signs as a disease spy. Int J Dermatol 2020;59:e213-4. [Google Scholar | PubMed]
- 2.Seo KB, Yoo SJ, Chu YY, Lim C. Osteoid osteoma of the proximal phalanx of the great toe in a 13-year-old female patient. J Am Acad Orthop Surg Glob Res Rev 2023;7:e21.00223. [Google Scholar | PubMed]
- 3.Turkmen I, Alpan B, Soylemez S, Ozkan FU, Unay K, Ozkan K. Osteoid osteoma of the great toe mimicking osteomyelitis: A case report and review of the literature. Case Rep Orthop 2013;2013:234048. [Google Scholar | PubMed]
- 4.Jowett CR, Singh D. Osteoid osteoma of the great toe: A case report. Foot Ankle Surg 2010;16:e12-5. [Google Scholar | PubMed]
- 5.Mohsen M, Ilaslan H, Davis A, Sundaram M. Subungual osteoid osteoma of the distal phalanx of the great toe. Orthopedics 2015;38:344, 398-9. [Google Scholar | PubMed]
- 6.Thiemann R, Seide HW, Luitjens KD, Beil FT, Rolvien T, Krüger L. Erschwerte diagnosestellung eines osteoidosteoms der Großzehe: Fallbericht mit review der literatur [Difficulties in diagnosing an osteoid osteoma of the big toe: A case report with review of the literature]. Orthopade 2021;50:689-99. [Google Scholar | PubMed]
- 7.Torrent J, Bailez A, Asuncion J. Recurrence of an intra-articular osteoid osteoma of the great toe: A case report and review of the literature. J Surg Case Rep 2017;2017:rjw226. [Google Scholar | PubMed]
- 8.Kahn MD, Tiano FJ, Lillie RC. Osteoid osteoma of the great toe. J Foot Surg 1983;22:325-8. [Google Scholar | PubMed]
- 9.Ekmekci P, Bostanci S, Erdoğan N, Akçaboy B, Gürgey E. A painless subungual osteoid osteoma. Dermatol Surg 2001;27:764-5. [Google Scholar | PubMed]
- 10.Basile A, Liuni FM, Fontanarosa A, Zoccali C, Baldi J, Lanzetti RM. Osteoid osteoma of the proximal phalanx of the hallux: A case report of a challenging diagnosis. Acta Biomed 2020;91:360-4. [Google Scholar | PubMed]
- 11.Özdemir M, Kavak RP, Demirler Şimşir B, Duman E. Unusually delayed manifestation of a hallux osteoid osteoma: A case report. Int J Surg Case Rep 2020;68:8-11. [Google Scholar | PubMed]
- 12.Oztürk A, Yalçinkaya U, Ozkan Y, Yalçin N. Subperiosteal osteoid osteoma in the hallux of a 9-year-old female. J Foot Ankle Surg 2008;47:579-82. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Efficacy and Safety of Microwave Ablation for Osteoid Osteoma: A Retrospective Analysis of 35 Cases
June 1, 2026 Efficacy and Safety of Microwave Ablation for Osteoid Osteoma: A Retrospective Analysis of 35 Cases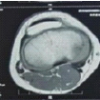 June 1, 2026 Cortical Lytic Lesion of the Proximal Tibia in an 8-Year-Old Child: A Pediatric Diagnostic Conundrum
June 1, 2026 Cortical Lytic Lesion of the Proximal Tibia in an 8-Year-Old Child: A Pediatric Diagnostic Conundrum May 1, 2026 Atypical Hip Pain due to Intra-articular Osteoid Osteoma Treated by Surgical Hip Dislocation in an Adolescent: Case Report
May 1, 2026 Atypical Hip Pain due to Intra-articular Osteoid Osteoma Treated by Surgical Hip Dislocation in an Adolescent: Case Report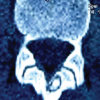 May 1, 2026 Navigation-Assisted Endoscopic Excision of Lumbar Vertebral Osteoid Osteoma: A Case Report
May 1, 2026 Navigation-Assisted Endoscopic Excision of Lumbar Vertebral Osteoid Osteoma: A Case Report