
Bilateral avulsion fractures of extensor carpi ulnaris (ECU) are rare injuries. Prompt diagnosis and appropriate management leads to good functional outcome.
Dr. Rajesh Kumar Vemparala, Department of Orthopaedic Surgery, Athani Hospitals, Palakkad, Kerala, India. E-mail: drrajesh086@gmail.com
Abstract
Introduction: Avulsion fractures of the extensor carpi ulnaris (ECU) from its insertion are rare injuries that are rarely reported in the literature. Most of the case reports detailed closed ruptures. We present avulsion fractures of the bilateral ECU from the base of the 5th metacarpal. Not much of the literature has been published in this regard.
Case Report: A 33 year old male presented with pain around both wrists and hands following a fall from a bike. Following evaluation and radiological investigation, he was found to have a volar Barton fracture with an undisplaced avulsed 5th metacarpal base fracture on the right side and a displaced avulsed fracture of the left 5th metacarpal base. Internal fixation of the volar Barton fracture and mini open fixation of the left 5th metacarpal were done with a wire. The wires were removed at 6 weeks and rehabilitation started. At 3 months, the patient returned to activity with full wrist and hand function.
Conclusion: Bilateral avulsion fractures of the ECU from its insertion are a rare injury. Displaced fractures might benefit from surgical intervention. Early diagnosis and treatment are essential for a good functional outcome.
Key words: Avulsion fracture, extensor carpi ulnaris, 5th metacarpal base.
The extensor carpi ulnaris (ECU) functions to dorsiflex and ulnarly deviate the wrist. In addition, it is an important stabilizer of the distal radioulnar joint [1]. ECU avulsion fractures are rare injuries that have not been previously described in the literature. The reported case details ECU avulsion fractures in the setting of wrist and forearm injuries. They reported fixation using K-wires and wire loops with satisfactory patient outcomes [2]. Several case reports detail closed ruptures [3]. Several cases of avulsion fractures of radial wrist extensors at their insertion are also reported in the literature [4-6]. We present a bilateral ECU avulsion fractures that has not been reported in the literature.
Patient information
A 33-year-old male presented one week after falling from a bike with pain and swelling over the bilateral hand and around the right wrist. There was no history of comorbidities.
Clinical findings
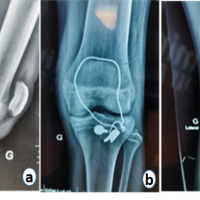
His vitals were stable. Tenderness was present over the dorsum of the base of the 5th metacarpal in both hands, and tenderness was present around the right wrist. Wrist extension and ulnar deviation strength were reduced on the left side. He was immobilized in a below elbow splint, and radiographs were taken. X-rays showed a left 5th metacarpal shaft with a displaced avulsed base fracture (Fig.1) and an undisplaced 5th metacarpal base fracture along with a volar Barton fracture on the right side (Fig. 2). A CT right wrist confirmed a fracture involving the volar ulnar corner of the distal radius (Fig.3).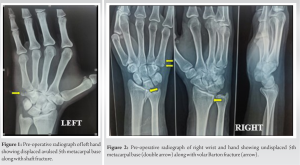
Treatment
Considering the displaced avulsed fracture and concern for altered wrist mechanics if left untreated, the patient was planned for operative repair.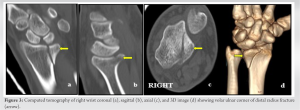
Left: Through a mini-open approach, under image guidance, fracture is reduced using a clamp. In keeping the fracture in reduction, a 1.5-mm K-wire was inserted to stabilize the avulsed fragment along with the shaft fracture (Fig. 4).
Right: Ulnar palmar approach was used to address the volar ulnar corner fracture fragment of the distal radius. Fracture is approached using the interval between the ulnar neurovascular bundle and the flexor tendon’s. Fracture is reduced and buttressed using a L-plate with screws (Fig.5). As the 5th metacarpal base fracture was undisplaced, it was decided to treat it non operatively.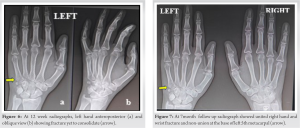
Follow-up and outcome
Post-operatively, the patient was placed in a short arm splint with the wrist in slight extension and ulnar deviation in the left hand. Later, it was changed to a cast after suture removal and once the wound healed. At 6 weeks, K-wires were removed and hand therapy protocol exercises were started. At 12 weeks, he had nearly symmetric wrist strength and range of motion, with no functional deficits (Fig.6). He resumed work after 12 weeks. At 7month follow up, though the radiograph showed no-union at the fracture site (Fig.7) clinically, he had full range of hand, wrist movements, and adequate grip strength (Fig. 8).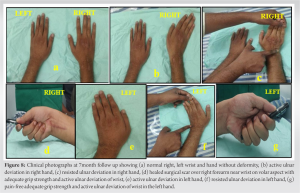
ECU an extensor compartment muscle of the forearm originates at the lateral epicondyle of the elbow and the posterior border of the ulna passes through the ECU groove and inserts into the base of the 5th metacarpal (Fig.9). The ECU functions not only as a dynamic stabilizer of the distal radioulnar joint [1] but also as an ulnar wrist extensor and ulnar deviator. Patients with ECU deficits may struggle to conduct some activities of daily living. Appropriate management may restore the functional activities of daily living. Lee et.al. [2] described a traumatic avulsion of the ECU tendon due to a roller injury. The functional outcome following the surgical intervention was found to be satisfactory.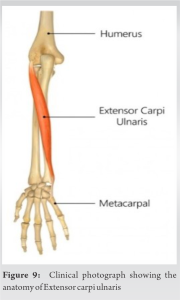
Moran and Ruby [3] described a closed rupture of the ECU with different mechanisms of injury. Several case reports of avulsion fractures of other wrist extensors have been described by DeLee [4], Jessa and Hodge [5], Sadr and Lalehzarian [6], Treble and Arif [7], Takami et.al.[8], Crichlow and Hoskinson [9]. The follow up of these patients has shown a good functional outcome. We present bilateral ECU avulsion fractures of both hands following a fall from a two-wheeler. The most probable mechanism of injury was forced flexion with simultaneous radial deviation of the wrist. On evaluation, it was found that there was a displaced avulsed fracture fragment on the left side and an undisplaced avulsed fracture on the right associated with a distal radius fracture. ECU functions not only an ulnar wrist extensor and ulnar deviator [10] but also as an important stabilizer of the distal radioulnar joint. Considering the importance of ECU in wrist kinematics, we elected surgical fixation. The avulsed fragment was reduced through a mini open approach and stabilized using a K-wire in the left hand. As the fracture was undisplaced in the right hand, it was decided to treat it non-operatively. The volar ulnar corner in the right wrist fracture was stabilized using a locking plate and screw. Following hand therapy at 12 weeks, the patient showed excellent results with minimal pain, full strength, and range of motion and returned to work. At 7 month follow up, though radiographs showed non-union at the fracture site, the patient maintained full range of motion and adequate grip strength without restriction.
A displaced avulsed fracture might benefit from surgical fixation to restore the functional kinematics of the wrist joint. Percutaneous fixation is one of the methods to reduce the fracture. Despite the rarity of these injuries, future work may focus on the better characteristics of these injuries and analyze the results of different techniques.
Bilateral ECU avulsion fractures are rare injuries. Proper diagnosis and timely intervention are essential to restore the functional biomechanics of the hand and wrist.
References
- 1.Spinner M, Kaplan EB. 22 Extensor carpi ulnaris: Its relationship to the stability of the distal radio-ulnar joint. Clin Orthop Relat Res 1970;68:124-9. [Google Scholar | PubMed]
- 2.Lee CY, Chen WC, Haw SY. Avulsion fracture of the extensor carpi ulnaris due to roller injury. J Chin Med Assoc 2005;68:237-9. [Google Scholar | PubMed]
- 3.Moran S, Ruby LK. Non rheumatoid closed rupture of extensor carpi ulnaris tendon. J Hand Surg 1992;17:281-3. [Google Scholar | PubMed]
- 4.DeLee JC. Avulsion fracture of the base of the second metacarpal by the extensor carpi radialis longus. A case report. J Bone Joint Surg Am 1979;61:445-6. [Google Scholar | PubMed]
- 5.Jessa KK, Hodge JC. Avulsion fracture of tendon of extensor carpi radialis longus: Unknown mechanism. J Emerg Med 1997;15:201-7. [Google Scholar | PubMed]
- 6.Sadr B, Lalehzarian M. Traumatic avulsion of the tendon of extensor carpi radialis longus. J Hand Surg 1987;12:1035-7. [Google Scholar | PubMed]
- 7.Treble N, Arif S. Avulsion fracture of the index metacarpal. J Hand Surg Br 1987;12:389. [Google Scholar | PubMed]
- 8.Takami H, Takahashi S, Ando M. Avulsion fracture of the second metacarpal base by the extensor carpi radialis longus. Arch Orthop Trauma Surg 1998;118:109-10. [Google Scholar | PubMed]
- 9.Crichlow TP, Hoskinson J. Avulsion fracture of the index metacarpal base: Three case report. J Hand Surg 1988;13:212-4. [Google Scholar | PubMed]
- 10.Brand PW, Beach RB, Thompson DE. Relative tension and potential excursion of muscles in the forearm and hand. J Hand Surg 1981;6:209-19. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 February 10, 2024 Tibial Tubercle Avulsion Fractures in Adolescence in Sports Injury about Four Cases Series
February 10, 2024 Tibial Tubercle Avulsion Fractures in Adolescence in Sports Injury about Four Cases Series August 10, 2022 An Avulsion Fracture of the Lesser Trochanter of the Femur with Prodromal Symptoms in an adult: A Case Report and Review of Literature
August 10, 2022 An Avulsion Fracture of the Lesser Trochanter of the Femur with Prodromal Symptoms in an adult: A Case Report and Review of Literature September 10, 2023 Use of Nanotechnology as an Alternative to Opioids for Post-operative Pain Management Following TKA
September 10, 2023 Use of Nanotechnology as an Alternative to Opioids for Post-operative Pain Management Following TKA July 1, 2026 Effectiveness of Conventional Kinesiotherapy and Pilates in Reducing Disability among Patients with Chronic Non-specific Low Back Pain
July 1, 2026 Effectiveness of Conventional Kinesiotherapy and Pilates in Reducing Disability among Patients with Chronic Non-specific Low Back Pain