
A novel extra-mucosal approach for limited oncologic mandibular resection is described.
Dr. Shruti Morabia, Department of Surgical Oncology, Sir H. N. Reliance Foundation Hospital and Research Centre, Prarthana Samaj, Girgaon, Mumbai, Maharashtra, India. E-mail: morabia.shruti@gmail.com, shruti.morabia@rfhospital.org
Abstract
Introduction: Malignant tumors afflicting the sub-condylar area and ascending ramus of the mandible without mucosal involvement are extremely rare. Traditional approaches such as lip-split-cheek flap and Visor flap would prove sub-optimal and excessive for such limited lesions and entail salivary contamination and mental nerve sacrifice. To circumvent these limitations, we developed a surgical approach that achieves wide, extra-oral exposure to the condyle and ascending ramus and permits controlled resection, affording protection to the facial nerve branches and mental nerve, while avoiding salivary contamination.
Cases: The main features of the approach include a pre-auricular skin crease incision extendable both ways, trans-parotid dissection with protection of facial nerve branches, and controlled bony resection. In all cases, monobloc resection was possible with preservation of the uninvolved facial nerve branches, avoidance of salivary contamination, and prompt healing.
Conclusion: An extra-oral non-mucosal surgical approach is described for highly selected cases of mandibular resection.
Keywords: Facial nerve, mandible, parotid gland, resections, non-mucosal.
Malignant lesions originating in the sub condylar region of the mandible and involving portions of the ascending ramus with no mucosal proximity are extremely rare and invariably demand sound surgical resection. The most common approaches to mandibular resection for all oncologic indications involve a lip-split of variable design, with a cheek flap for exposure to the area of resection [1] or alternatively, a Visor flap to gain access to the segment to be resected [2]. All these approaches are essentially trans-mucosal, with salivary contamination. We present an alternative “non-mucosal” approach with excellent exposure and significant advantages. There have been numerous extra-oral surgical approaches described in the literature for accessing the temporo-mandibular joint (TMJ) and condylar process of the mandible [3]. However, none of these are useful in oncologic settings, which typically require wide exposure of soft tissues along with bone. Furthermore, this area is perilously close to the extra-cranial, intra-parotid facial nerve arborization, which needs careful preservation [4]. We developed a surgical approach that achieves wide, extra-oral exposure to the condyle and ramus of the mandible with adequate preservation of facial nerve branches. In addition, this approach avoids sacrifice of the inferior dental nerve and prominent scars over the lower face, while remaining extra-mucosal and avoiding salivary contamination.
The incision is placed in a pre-auricular skin crease and is extendable upwards into the hair-bearing scalp and downward into the neck. Following elevation of extra-platysmal skin flaps, trans-parotid dissection is performed, with demonstration and protection of facial nerve branches. This enables controlled bony resection without either mucosal violation or nerve damage. In addition, the inferior alveolar nerve is spared whenever appropriate, protecting lip sensation; and facial scars are avoided in aesthetically prominent areas. The approach is versatile, permitting generous exposure to even the deep parapharyngeal space, as will be seen in ensuing descriptions.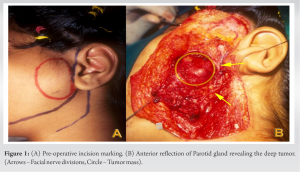
Case 1
A 17-year-old female of Indian origin presented with a painless, apparently causeless swelling in the left pre-auricular region, increasing rapidly in size over a 2-month period. Physical examination revealed a solitary, 3 × 3 cm, bony hard, non-tender swelling in the stated area with no evidence of intra-oral extension, and with free movements at the TMJ. Evaluation of the facial nerve demonstrated normal function. Computed tomography (CT) imaging demonstrated a bony lesion in the sub condylar region of the mandible, exhibiting a sunburst type of periosteal reaction along the lateral aspect of the ascending ramus and condylar process of the mandible, suggestive of chondrosarcoma/osteogenic sarcoma. The surrounding soft tissues as well as the remaining portion of the mandible were uninvolved. Magnetic resonance imaging (MRI) demonstrated a well-defined mass with altered marrow signals limited to the site of the lesion. The surrounding soft tissues were normal. Surgical excision was thus advised on the presumptive diagnosis of a malignant lesion arising from and limited to the sub condylar region of the mandible. A pre-auricular incision was planned with extension craniad into the hair bearing area of the scalp and caudad into the upper neck crease (Fig. 1a). A large skin flap was elevated anteriorly in an extra-platysmal plane, beyond the palpable limit of the mass, maintaining the parotido-masseteric fascia intact. Dissection was then undertaken to demonstrate the main trunk of the facial nerve and its proximal division. The principal upper and lower divisions were displaced away from each other by the mass during their intra-parotid course. These divisions were dissected peripherally into the parotid substance, carrying the dissection down to the level of the masseter muscle. The anterior limit of dissection was deliberately kept short of the anterior parotid margin to leave as much as possible of the intra-parotid as well as the peripheral arborization of the nerve undisturbed. The central portion of the parotid gland overlying the lesion was now free above and below and connected anteriorly with the rest of the parotid gland. This portion of the gland was then separated posteriorly and reflected anteriorly, off the masseter, displaying the muscle with the underlying tumor-bearing bone. This revealed a well-circumscribed mass arising from the sub condylar region, with no involvement of the surrounding muscles and soft tissues (Fig. 1b). Dividing the masseter fibers around the tumor bearing area resulted in demonstration of normal bone of the mandible beyond the mass and the TMJ above. The mass approached the root of the coronoid process anteriorly, and the junction of the upper and middle thirds of the ascending ramus inferiorly.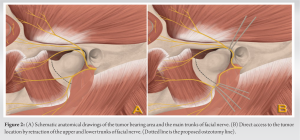
Carefully protecting facial nerve branches above and below, bony cuts were made through the surrounding normal bone (Fig. 2a and b) with a fine reciprocating saw, and the specimen removed in monobloc fashion by dividing the capsular ligaments and disarticulating at the TMJ (Fig. 3a). Immediate specimen radiographs demonstrated bone margins to be clear. After securing complete hemostasis, the central portion of the parotid gland was returned to its bed, avoiding a conspicuous hollow. Bony reconstruction was not performed. The wound was closed over a single non-suction drain. The patient returned to oral feeds by the evening of surgery and was discharged on the 3rd post-operative day.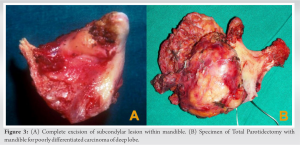
The post-operative period was uneventful, with primary uncomplicated healing of all wounds. There was transient paresis of the left angle of the mouth, which recovered fully to restore normal facial nerve function. Normal occlusal relationships were preserved, and dental and lip sensations were fully intact. The aesthetic result was excellent, with inconspicuous scarring and normal facial expression. Final histopathologic evaluation of the specimen revealed Ewing’s sarcoma with clear margins. Adjuvant chemo-radiation was advised but refused by the patient, who remains free of disease, 16 years post-surgery.
Case 2
A 60-year-old gentleman first presented elsewhere with a 3–4-month history of progressive left hemi-facial pain that was originally thought to be dental in origin. When there was no relief and in fact worsening of symptoms, a CT scan was advised, which revealed a deep lobe parotid mass. Soon, he went on to develop a lower motor neuron facial palsy, followed within a week by hoarseness and dysarthria, suggesting vagal and hypoglossal nerve involvement. MRI evaluation revealed a large, 6 cm deep lobe parotid tumor, tightly abutting the inner surface of the ramus of the mandible, with effacement of the intervening plane and possible involvement of the inferior alveolar nerve at the lingula. A PET-CT had also been performed, which demonstrated a metabolically active lesion as above, with no evidence of distant metastasis. CT-guided fine-needle aspiration cytology had been performed and reported as a poorly differentiated carcinoma. He was advised urgent surgery. At surgery, an extended pre-auricular approach was employed and the main trunk of the facial nerve exposed posteriorly at its emergence from the stylomastoid foramen. The nerve appeared congested, and the lower trunk inseparable from the parotid mass. A decision was taken to divide the lower trunk just beyond its origin, preserving the main trunk and the upper division. The TMJ, coronoid process, and ascending ramus were all exposed externally. Without breach of the oral mucosa, the ascending ramus was divided with an oscillating saw just beyond the angle of the mandible, and the condyle of the mandible disarticulated at the TMJ. The divided mandible was then rotated externally to provide direct access to the adherent tumor mass. It was possible to separate the tumor from the internal carotid artery, which was stretched, and from the vagus and hypoglossal nerves, which were compressed and displaced. The cranial limit of dissection was at the skull base and a complete monobloc R0 resection achieved, incorporating the tumor mass in continuity with the mandibular ramus (Fig. 3b). A cable graft was placed between the cut end of the lower trunk of the facial nerve and the peripheral portion of the marginal mandibular nerve. A significant skeletal and soft tissue gap resulted following the extensive resection, which was filled with a Pectoralis major flap incorporating a de-epithelialized skin paddle. Final histopathology confirmed a poorly differentiated carcinoma of salivary origin with negative nodes and clear margins. Recovery of vagal and hypoglossal function and complete relief of pain marked the post-operative period. The patient went on to receive radical adjuvant radiotherapy. At 6 months follow-up post-surgery, the patient was locally controlled, pain free and had regained eye-closure, indicating return of function of the upper trunk of the facial nerve. He finally succumbed to liver metastases, remaining locally controlled and symptom-free.
Case 3
A 55-year-old gentleman, who had received extensive treatment earlier (repeatedly operated, reconstructed, and radiated twice earlier for multifocal advanced cancers of the tongue and left cheek), presented with a painful, solitary intra-osseous metastasis in the area of the right mandibular angle. Imaging demonstrated a large focus of disease completely eroding the mandible at the area of the right angle and ascending ramus without any mucosal disease. CT-assisted biopsy confirmed squamous carcinoma. We were thus confronted with a unique situation where a major segmental mandibulectomy was needed, without disturbing the intra-oral flap or the twice-operated lip. The extra-oral approach (slightly modified to achieve exposure to the angle of the mandible) was employed. The angle was first exposed, followed by adjacent portions of the ramus and body, to gain direct access to the diseased portion of the mandible for resection. The intra-oral flaps were undisturbed, salivary contamination avoided, and primary healing achieved in a hostile field. Complete pain relief was achieved before the patient finally succumbed to distant metastasis.
A well-chosen surgical incision is the first and key step during any surgical procedure in the facial area [5]. Several surgical approaches have been described in the literature for access to the TMJ and condylar area such as pre- and post-auricular [4] and endaural [6] approaches which offer limited but sufficient access for the same. In these approaches, the facial nerve is not electively demonstrated. For procedures requiring more extensive access, the coronal approach [7] can be employed. Retromandibular and submandibular incisions are also used for surgeries of the sub condylar region [8-10]. However, the most preferred incision is preauricular [11] with its numerous modifications in incision design [3,12] and dissection techniques depending on the plane and area of exposure needed [7,13]. All these approaches have been used mainly for sub condylar fractures, TMJ surgeries including replacement, and benign neoplasms involving the joint. This is perhaps the first paper which outlines the use of an extra-oral non-mucosal pre-auricular approach for oncologic resections. For all posteriorly located malignant lesions of the mandible, splitting of the lower lip with lateral reflection of the cheek flap is the typical approach [14]. The Visor flap is a good alternative, which avoids splitting the lip, but is suitable mainly for tumors that involve the body and angle portion of the mandible. In cases where only the condyle/TMJ and surrounding soft tissues are involved, without involvement of the mucosa of the oral cavity, a traditional lip split-cheek flap or a Visor flap would result in unnecessary dissection, with the target area of resection being far away from the incision. The conventional lip-split and cheek flap approach employed for hemi-mandibular resection were considered unsuitable in the above cases for numerous reasons. First, to obtain sufficient access, it would have been necessary to completely erase the attachments of the masseter and superficial temporalis, perform a great deal of unnecessary dissection around the body of the mandible, and retract considerably to reach the main area of interest, which would be the deepest and farthest point of exposure. Moreover, to achieve a wide, monobloc resection of the sub condylar area with a cuff of soft tissue would undoubtedly place the facial nerve branches at risk due to uncontrolled diathermy dissection. Second, it would involve sacrifice of the mental nerve, producing anesthesia of half of the lip on the side of division. Finally, the cheek flap approach would entail a prominent scar across the median plane of the lower face, and risk salivary contamination. Thus, we modified the pre-auricular approach, extended it sufficiently to give adequate exposure for a monobloc resection without visible facial scar, or injury to the facial nerve. The hallmark of our approach was a direct and generous exposure of the lesion permitting oncologically sound monobloc resection. Moreover, all important masticatory muscle attachments as well as the inferior alveolar nerve were preserved. This allowed excellent occlusion and masticatory function, without any bony reconstruction, and preserved normal dental and lip sensation. Since the approach was entirely non-mucosal with no salivary contamination, oral feeding could be started soon after surgery. Finally, the aesthetic result was most gratifying, with normal contour and inconspicuous scarring. Beyond doubt, the use of this approach must be highly selective. For routine exposure of the TMJ or for resection of benign pathologies [15] that can be removed in piece-meal fashion [16], fractures of the condyle [5,17], ankylosis of TMJ [18], and the traditional pre-auricular approach would be optimal. However, in dealing with large malignant lesions in the area of the condyle and sub-condylar area [19] where safety of the facial nerve cannot be assured, our new extended approach should find considerable usefulness. Since considerable variation exists in the pattern of facial arborization [20,21], the exact details would vary in each individual case. Finally, only a team familiar with parotid surgery and micro-neural repair must employ this approach.
All three cases, though rare, illustrate the usefulness of an approach that aims to protect the facial nerve while providing controlled access to the condyle, sub condylar area, ascending ramus of the mandible, and the deep and superior reaches of the parapharyngeal space for complex and uncommon malignant lesions. The completely extra-oral non-mucosal nature of the approach provided freedom from salivary contamination in a field studded with important neuro-vascular structures. Prompt healing permitted early oral feeds and radiation therapy. We advocate this approach for its relative simplicity, extensive access for oncologically safe resections and cosmetically inconspicuous scarring – all without damage to the facial nerve.
An extra-oral approach to the condyle and ramus of the mandible is described, which entails an extended Parotid incision. In highly selected indications, it permits oncologic resections without facial nerve damage or salivary contamination, with gratifying outcomes.
References
- 1.Strong EW, Spiro RH. Cancer of the oral cavity. In: Strong Suen EN, Spiro Myers EN, editors. Cancer of the Head and Neck. New York: Churchill Livingstone; 1981. p. 301-41. [Google Scholar | PubMed]
- 2.LaFerriere KA, Sessions DG, Thawley SE, Wood BG, Ogura JH. Composite resection and reconstruction for oral cavity and oropharynx cancer. A functional approach. Arch Otolaryngol 1980;106:103-10. [Google Scholar | PubMed]
- 3.Al-Kayat A, Bramley P. A modified pre-auricular approach to the temporomandibular joint and malar arch. Br J Oral Surg 1979;17:91-103. [Google Scholar | PubMed]
- 4.Garcia Y Sanchez JM, Davila Torres J, Pacheco Rubio G, Gómez Rodríguez CL. Bat wing surgical approach for the temporomandibular joint. J Maxillofac Oral Surg 2015;14:875-81. [Google Scholar | PubMed]
- 5.Li H, Zhang G, Cui J, Liu W, Dilxat D, Liu L. A modified preauricular approach for treating intracapsular condylar fractures to prevent facial nerve injury: The supratemporalis approach. J Oral Maxillofac Surg 2016;74:1013-22. [Google Scholar | PubMed]
- 6.Santos GS, Nogueira LM, Sonoda CK, de Melo WM. Using endaural approach for temporomandibular joint access. J Craniofac Surg 2014;25:1142‐3. [Google Scholar | PubMed]
- 7.Obwegeser HL. Temporal approach to the TMJ, the orbit, and the retromaxillary-infracranial region. Head Neck Surg 1985;7:185-99. [Google Scholar | PubMed]
- 8.Qiu YT, Yang C, Chen MJ, Qiu WL. Can a novel surgical approach to the temporomandibular joint improve access and reduce complications? J Oral Maxillofac Surg 2016;74:1336-42. [Google Scholar | PubMed]
- 9.Kreutziger KL. Surgery of the temporomandibular joint. I. Surgical anatomy and surgical incisions. Oral Surg Oral Med Oral Pathol 1984;58:637-46. [Google Scholar | PubMed]
- 10.Sohrabi M, Esmaeelinejad M. Surgical approaches to the temporomandibular joint. In: Emes Y, Aybar B, Dergin B, editors. Temporomandibular Joint Pathology- Current approaches and Understanding. London, England: Intech Open; 2018. p. 185-98. [Google Scholar | PubMed]
- 11.Idle MR, Lowe D, Rogers SN, Sidebottom AJ, Speculand B, Worrall SF. UK temporomandibular joint replacement database: Report on baseline data. Br J Oral Maxillofac Surg 2014;52:203-7. [Google Scholar | PubMed]
- 12.Al-Mahdi AH. Zigzag temporal incision with preauricular incision extension as a variant approach to the temporomandibular joint. J Craniofac Surg 2016;27:e605-6. [Google Scholar | PubMed]
- 13.Politi M, Toro C, Cian R, Costa F, Robiony M. The deep subfascial approach to the temporomandibular joint. J Oral Maxillofac Surg 2004;62:1097‐102. [Google Scholar | PubMed]
- 14.Cantù G, Bimbi G, Colombo S, Compan A, Gilardi R, Pompilio M, et al. Lip-splitting in transmandibular resections: Is it really necessary? Oral Oncol 2006;42:619-24. [Google Scholar | PubMed]
- 15.Park SH, An JH, Han JJ, Jung S, Park HJ, Oh HK, et al. Surgical excision of osteochondroma on mandibular condyle via preauricular approach with zygomatic arch osteotomy. Maxillofac Plast Reconstr Surg 2017;39:32. [Google Scholar | PubMed]
- 16.Yang XJ Jr., Yang C, Chen MJ, Zhang XH, Qiu YT, He DM, et al. Preauricular transcondylar approach for basal cell adenoma of parotid coexist with ganglion cyst of the ipsilateral temporomandibular joint. J Craniofac Surg 2011;22:e23-6. [Google Scholar | PubMed]
- 17.Liao HT, Wang PF, Chen CT. Experience with the transparotid approach via a mini-preauricular incision for surgical management of condylar neck fractures. J Craniomaxillofac Surg 2015;43:1595-601. [Google Scholar | PubMed]
- 18.Makiguchi T, Yokoo S, Kosugi K. Transparotid approach for the treatment of condylar osteochondroma and ankylosis of the temporomandibular joint. J Craniofac Surg 2015;26:e582-4. [Google Scholar | PubMed]
- 19.Zitsch RP 3rd, Patenaude B, Tidmore T. An extraoral parapharyngeal space approach via vertical ramus osteotomy. Am J Otolaryngol 2007;28:330-3. [Google Scholar | PubMed]
- 20.Davis RA, Anson BJ, Budinger JM, Kurth LR. Surgical anatomy of the facial nerve and parotid gland based upon a study of 350 cervicofacial halves. Surg Gynecol Obstet 1956;102:385-412. [Google Scholar | PubMed]
- 21.McCormack LJ, Cauldwell EW, Anson BJ. The surgical anatomy of the facial nerve. Surg Gynecol Obstet 1945;80:620. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 March 10, 2023 Chronic Neglected Scapho-capitate Syndrome: A Rare Case Report with Management
March 10, 2023 Chronic Neglected Scapho-capitate Syndrome: A Rare Case Report with Management October 10, 2016 Localized Tetanus in an Adult Patient: Case Report
October 10, 2016 Localized Tetanus in an Adult Patient: Case Report March 1, 2026 Hanky-in-the-Pocket Inlay Technique for Managing Incidental Dural Tears in Lumbar Unilateral Biportal Endoscopy Using Collagen Matrix- Technical Note with Case Series
March 1, 2026 Hanky-in-the-Pocket Inlay Technique for Managing Incidental Dural Tears in Lumbar Unilateral Biportal Endoscopy Using Collagen Matrix- Technical Note with Case Series January 1, 2026 Intratendinous Lipoma of Biceps Long Head: A Case Report and Current Concepts Review of Musculoskeletal Lipomas
January 1, 2026 Intratendinous Lipoma of Biceps Long Head: A Case Report and Current Concepts Review of Musculoskeletal Lipomas