
Internal fixation is indicated in patients with traumatic scapula fractures with intrathoracic interposition.
Dr. Liam Ortega, Department of Orthopaedics and Sports Medicine, Mercy Health St. Vincent Medical Center, 2409 Cherry Street, Suite #10, Toledo, OH 43608, USA. E-mail: Lortega@mercy.com
Abstract
Introduction: Scapula fractures are infrequently operated on due to the high union rate and well-preserved motion despite a large degree of angular deformity. Scapula fractures with intrathoracic interposition are rare and typically require open reduction due to an increased risk of pleural injury from the interposed segment. While there are several reports of intrathoracic interposition of scapular fractures requiring open reduction, only one case involved subsequent fragment fixation in an adult.
Case Report: Here, we present a 60-year-old male truck driver who fell from a 3-foot height and sustained a comminuted scapula body fracture with intrathoracic interposition of the lateral column adjacent to the pleural space. Following open reduction and internal fixation of the displaced fragment, the patient had satisfactory pain relief and no respiratory compromise during the acute hospital admission. The patient returned to full work duties without limitations or functional deficits as a heavy laborer.
Conclusion: This case report describes a unique case and operative indication for open reduction and internal fixation of scapula fractures. Following open reduction of the interposed fragment, internal fixation should be considered to reduce the risk of further displacement and to optimize post-operative outcomes.
Keywords: Scapula fractures, intrathoracic interposition, open reduction and internal fixation, operative indication.
Scapula fractures account for <5% of shoulder girdle injuries and carry a 10% risk of mortality due to the high energy mechanism and commonly associated thoracic and head injuries [1]. Open reduction and internal fixation (ORIF) is often performed when the scapular body is angulated >40° or if there is 2 cm medialization of the lateral column [2]. When the fracture includes the following characteristics, surgery is a reasonable option: (1) displaced fractures in the glenoid, (2) displaced fractures of the glenoid neck, and (3) double disruptions of the superior shoulder suspensory complex when one or more elements of the scapula are significantly displaced [3]. Scapula fracture with intrathoracic interposition is a unique variant that typically involves penetration of the thoracic cavity by the lateral column fragment. The scapular body exhibits varying thickness, thinner at the center and thicker at the periphery, which may be why the lateral column apex is responsible for intrathoracic interposition [4]. Often, cardiothoracic surgeons are relied on when there is penetration of the thoracic cavity adjacent to, into, or through the pleural space. A review of the literature found six instances where an orthopedic surgeon surgically managed this scapula fracture variant, including three cases in adults [1, 2, 5-8]. Open reduction was performed in each case, although only one utilized internal fixation with a plate and screw construct [2]. Of those without internal fixation, 50% reported needing to repeat surgery or had difficult post-operative periods due to pain or delayed healing [1,7]. This report describes a comminuted scapula body fracture with intrathoracic interposition of the lateral column adjacent to the pleural space. Although the displaced fracture fragment was extrapleural, its intrathoracic interposition risked causing pleural injury and potential respiratory compromise. The position of the fragment would not promote healing, function, or pain relief if left untreated. Moreover, if treated without internal fixation after extrication of the fracture segment, there is potential that the impaired soft tissue envelope would allow the segment to displace back to its intrathoracic position, resulting in a painful nonunion or impaired functional capacity.
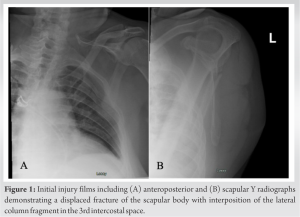
A 60-year-old male truck driver fell from a 3-foot height onto his left shoulder. The patient denied hitting his head, having loss of consciousness, or any new numbness or tingling in his left upper extremity. On arrival at the emergency department, the patient was hemodynamically stable and saturating well on room air. Radiographs were obtained in the emergency department and demonstrated a left scapula body fracture with a portion of it interposed between the third and fourth rib (Fig. 1).
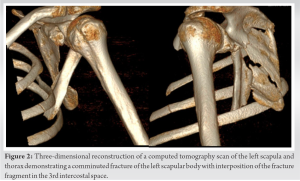
Computed tomography (CT) scan further confirmed an interposed fracture segment of the scapula within the 3rd intercostal space (Fig. 2),
with axial scans confirming a small pleural effusion but no pneumothorax or hemopneumothorax (Fig. 3).

A thoracostomy tube was placed by the trauma surgery service on the ipsilateral side at the location of the 4th intercostal space at the anterior axillary line. The patient was neurovascularly intact to the left upper extremity and hemodynamically stable before operative intervention.
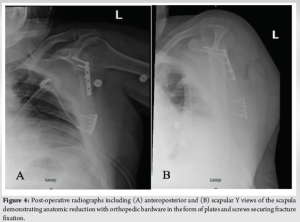
Cardiothoracic surgery was aware of this surgery and was on standby at our Level I trauma center. In the prone position, a standard approach to the lateral border of the scapula was performed. Interval between the infraspinatus and teres minor was used to access the lateral column and main fracture segment. Caudally, the lateral column segment was visualized, lodged between the third and fourth ribs. The segment was slowly extricated with a pointed reduction clamp. During and after the removal of the interposed fracture segment, vitals were assessed and found to be stable. The remaining procedure was executed using two 2.7 mm flexible mini-fragment plates, one plate at the cranial portion of the lateral column inferior to the glenoid, and the second plate along the caudal aspect near the inferior angle of the scapula (Fig. 4). Incision was closed in a layered fashion. The patient was placed in a sling for 2 weeks followed by a progressive motion program, without pushing, pulling, or lifting for 6–8 weeks.
The chest tube was removed on post-operative day 3 and the patient was discharged with adequate pain control achieved with oral medications. The patient returned to work as a heavy laborer without functional limitations or deficits at 8-week post-operative. At the patient’s last televisit follow-up 17-month post-operative, the patient had full painless shoulder range of motion compared to the contralateral extremity.
While there is a low occurrence of scapula fractures, they are often due to high energy mechanisms and occur concomitantly with other injuries such as ipsilateral rib and clavicle fractures, chest wall injuries, pelvic fractures, and head injuries. About 90% of patients with scapular fractures also have an associated life-threatening injury [7]. Often, the scapula fracture can be missed on initial chest radiographs. Subsequently, fixation is performed in a delayed fashion due to factors related to surgical clearance or because the scapula fracture was a late diagnosis. Scapular intrathoracic interposition has been cited 9 times in the literature [1-10]. Six cases involved scapular fractures and required open reduction of the interposed fragment within the chest wall. Of those, internal fixation was performed in only two cases, involving a plate and screw construct in an adult [2] and an absorbable suture in a 10-year-old [5]. Porte et al. [1] describe a case of a scapula fracture in a 30-year-old female with interposition of the fragment in the 4th intercostal space. In their case, the fracture fragment was removed from the 4th intercostal space by means of open reduction. Notably, there was no internal fixation of the fracture fragment to the body of the scapula. On follow-up, the fragment had displaced into the 4th intercostal space, and there was heterotopic ossification between the fragment, the surrounding ribs, and the main scapular body. A second surgery with the application of a composite mesh was needed to prevent further ossification. Van Schie-van der Weert et al. [7] describe a case of a comminuted scapula fracture with intrathoracic interpositioning of a large fragment in the 5th intercostal space. The fracture fragment was removed with no applied internal fixation. This patient was discharged on hospital day 10, which was double the length of stay seen in our case. Furthermore, this patient required an epidural catheter for pain control, while the patient in our case required minimal oral narcotic medication. This suggests that fracture fixation at the time of reduction may decrease post-operative pain and reduce the hospital length of stay. Our case highlights another indication for ORIF of the scapula. Radiographs and CT scans should be heavily scrutinized for interposition within the intercostal space, as well as intrathoracic positioning of the fragment that could compromise respiratory function. The patient was last evaluated 17 months postoperatively through televisit, which demonstrated full painless shoulder range of motion, and a full return to work as a heavy laborer. While there are several reports of intrathoracic interposition of scapular fractures, only one case involved fragment fixation in an adult. Although it would be possible to perform percutaneous extrication of the fragment alone, open techniques are intuitively safer and provide the opportunity to apply internal fixation strategies that ultimately improve functional and radiographic outcomes, in addition to reducing pain and hospital length of stay.
Conventionally, scapula fractures have largely been treated non-operatively. There is an expanding list of indications to fix the scapula, and intrathoracic interposition of the lateral column fragment should be considered to prevent future malreduction and non-union, reduce hospital stay length, and provide a reliable functional outcome.
Without internal fixation, there is potential for the fracture segment to displace back to its intrathoracic position, resulting in malunion, increased acute or chronic pain, or impaired functional capacity.
References
- 1.Porte AN, Wirtzfeld DA, Mann C. Intrathoracic scapular impaction: An unusual complication of scapular fractures. Can J Surg 2009;52:E62-3. [Google Scholar | PubMed]
- 2.Schwartzbach CC, Seoudi H, Ross AE, Hendershot K, Robinson L, Malekzadeh A. Fracture of the scapula with intrathoracic penetration in a skeletally mature patient. A case report. J Bone Joint Surg Am 2006;88:2735-8. [Google Scholar | PubMed]
- 3.Goss TP. Scapular fractures and dislocations: diagnosis and treatment. J Am Acad Orthop Surg 1995;3:22-33. [Google Scholar | PubMed]
- 4.Nettrour LF, Krufky EL, Mueller RE, Raycroft JF. Locked scapula: Intrathoracic dislocation of the inferior angle. A case report. J Bone Joint Surg Am 1972;54:413-6. [Google Scholar | PubMed]
- 5.Park HY, Jang HJ, Sur YJ. Scapular body fracture and concomitant inferior angle apophyseal separation with intrathoracic displacement: A case report. J Pediatr Orthop B 2017;26:429-32. [Google Scholar | PubMed]
- 6.Shin SJ, Wang SI, Kim JR. Lung injury caused by greenstick fracture of the scapular body in a 6-year-old boy. Skeletal Radiol 2016;45:555-8. [Google Scholar | PubMed]
- 7.van Schie-van der Weert EM, van Laanen JH, Kraan GA, de Vries MR. Intrathoracic displacement of a scapular fracture: A case report. J Bone Joint Surg Am 2012;94:e16. [Google Scholar | PubMed]
- 8.Blue JM, Anglen JO, Helikson MA. Fracture of the scapula with intrathoracic penetration. A case report. J Bone Joint Surg Am 1997;79:1076-8. [Google Scholar | PubMed]
- 9.Demirkiran ND, Kar A. Pure intrathoracic scapular dislocation. Am J Orthop (Belle Mead NJ) 2016;45:E29-30. [Google Scholar | PubMed]
- 10.Lee RS, Dooley JF. Intrathoracic dislocation of the inferior pole of the scapula following thoracotomy. Acta Chir Belg 2012;112:450-2. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Column Involvement as a Predictor of Early Functional Outcome and Complications in Proximal Tibia Fractures: A Prospective Study
June 1, 2026 Column Involvement as a Predictor of Early Functional Outcome and Complications in Proximal Tibia Fractures: A Prospective Study December 1, 2025 Total Hip Replacement after Acetabular Fracture Fixation: Surgical Challenges, Techniques, and Outcomes
December 1, 2025 Total Hip Replacement after Acetabular Fracture Fixation: Surgical Challenges, Techniques, and Outcomes October 1, 2025 Non-union of Talus Fracture in a 34-Year-Old Male Managed with Open Reduction and Internal Fixation Using Cancellous Cannulated Screws: A Case Report
October 1, 2025 Non-union of Talus Fracture in a 34-Year-Old Male Managed with Open Reduction and Internal Fixation Using Cancellous Cannulated Screws: A Case Report October 1, 2025 Comparative Study of Minimally Invasive Plate Osteosynthesis Versus Open Reduction and Internal Fixation in the Treatment of Distal Fibular Fractures
October 1, 2025 Comparative Study of Minimally Invasive Plate Osteosynthesis Versus Open Reduction and Internal Fixation in the Treatment of Distal Fibular Fractures