
Prompt intervention of proximal femur ABCs with prophylactic fixation is necessary to prevent traumatic/atraumatic fractures following removal of the tumor and helping the patient to get back to his activities of daily living early.
Dr. Kartik Prashant Pande, Department of Orthopaedics, Grant Medical College, Mumbai, Maharashtra, India. E-mail: kartik.pande0393@gmail.com
Abstract
Introduction: Aneurysmal bone cyst is a benign, most often non-neoplastic lesion affecting the bone. Malignant transformation is reported in certain cases, although rare. It commonly occurs in young adults with around 75% of the cases occurring in the first two decades and 95% occurring in the first 3 decades. The management depends on the individual case parameters with ABC occurring in a weight-bearing area of a bone warranting an aggressive treatment plan with the consideration of preventing a pathological fracture.
Case Report: A 20-year-old male patient with no other comorbidities presented to us with complaints of atraumatic right hip pain of 9-month duration. On preliminary clinical examination and imaging studies with X-rays, CT scan, and MRI, the patient was diagnosed to have an aneurysmal bone cyst (ABC) of the right proximal femur. The patient was operated with intra-lesional excision with extended curettage and prophylactic fixation with DHS plating and kept on yearly follow-up. 10-year follow-up showed complete resolution of the lesion and implant removal was done after that.
Conclusion: As is clear from this case, the treatment of an aneurysmal bone cyst needs to individualized based on the patient’s age, complaints, and tumor behavior in terms of its aggressiveness, size, and its extent. Often, en bloc excision with extensive curettage is required along with bone grafting and prophylactic fixation to support the bone graft and to prevent a pathological fracture and further recurrence. Implant removal if indicated should be done after complete resolution of the lesion, patient willingness, and any other medical indication.
Keywords: ABC, DHS, en bloc excision, extended curettage, pathological fracture, implant removal.
Aneurysmal bone cyst is a benign, most often non-neoplastic lesion affecting the bone. Malignant transformation is reported in certain cases, although rare [1]. It is actually a misnomer as it is neither an aneurysm nor a truly cystic lesion as these are not lined by endothelial cells [2]. It commonly occurs in young adults with around 75% of the cases occurring in the first two decades and 95% occurring in the first 3 decades [3]. ABCs are seen mainly during childhood and in young adults with mean age being 13 years. Approximately 90% of the lesions are found before the age of 30. The male:female ratio of affection is around 1: 1.16 with females being slightly more affected than males [4]. These tumors have a predilection for metaphysis of a long bone including femur, tibia/fibula, and also upper extremity. However, ABCs are also known to afflict the entire skeleton given that they can present in the spine, pelvis, clavicle, foot, fingers, and sacrum. ABCs are usually solitary and are currently believed to be arising either as a primary tumor (translocation driven) or secondary lesions arising adjacent to osteoblastomas, chondroblastomas, or giant cell tumors [3,5]. The characteristic presentation of ABCs is pain and swelling over the affected area with or without a pathological fracture. Diagnosis is based on a thorough history taking, clinical examination, and imaging techniques such as X-ray, CT scan, and/or MRI. Even though all this is suggestive of ABC, confirmatory diagnosis will always be given by histopathological examination of the lesion either by incisional or excisional biopsy. The management depends on the individual case parameters with ABC occurring in a weight-bearing area of a bone warranting an aggressive treatment plan with the consideration of preventing a pathological fracture. ABC in the proximal femur is considered an aggressive lesion and accordingly needs an aggressive response due to the high rate of recurrence in this region and the risk of pathological fracture [6].
A 20-year-old male patient with no other commorbidities and working at a call center presented to us with complaints of atraumatic right hip pain of 9-month duration. The pain was insidious in onset and gradually progressive with time. It was of dull aching character which aggravated on exertion and not on activities of daily living and relieved on rest and on taking analgesics. 6 months after this, the patient started having pain during activities of daily living with major disability being pain during climbing stairs and on sitting cross-legged or squatting. The pain was relieved on rest and taking an increased dosage of analgesics. There was no history of night pain or fever with any other significant history. There was no history of any autoimmune disorder and subsequent steroid intake or a history of chronic alcohol consumption. On preliminary clinical examination, the only positive findings were tenderness on deep palpation and an antalgic gait. The Harris hip score was calculated [7]. It is a questionnaire consisting of ten items in 4 domains each. The 4 domains are pain, function, absence of deformity, and range of motion [8]. On presentation, it was calculated to be 76 (fair). Upon an initial imaging with X-ray pelvis with both hips, it revealed an eccentrically located cystic lesion circumscribed by a layer of thin cortical bone in the right proximal femur (Fig. 1).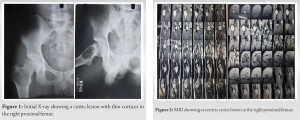
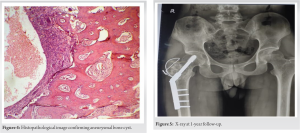
MRI was done for further evaluation (Fig. 2) which showed the characteristic “fluid-fluid” [9,10] levels which here represents the layering of blood of different densities atop one another, also, a hyperintense lesion in the proximal end of the shaft of the right femur with internal septations on T2-weighted image and hypointense on the T1-weighted image which was suggestive of an aneurysmal bone cyst.
Without further delay, anticipating a pathological fracture which ABCs are known to cause [11] leading to an acute increase in the symptoms, the patient was operated with intra-lesional excision, followed by high-speed burr with extended curettage, with phenol irrigation and prophylactic fixation with DHS plating with bone grafting (autograft plus allograft) and kept on regular follow up depicted here in the serial X-rays repeated every 3 years. Harris hip score was evaluated at every follow-up. 10-year follow-up showed complete resolution of the lesion at the end of which, implant removal was done, with full retainment of the functional range of motion attained 1 year after the surgical removal of the lesion.
Surgical procedure
After taking appropriate fitness for surgery, the patient was taken up for surgery. The patient was placed in a supine position over the operating traction table. Induced under all aseptic precautions and under spinal and epidural anaesthesia. Scrubbing, panting, and draping were done. A lateral incision was taken over the shaft starting from the tip of the greater trochanter extending 5 cm distal to it. Blunt dissection done up to the tensor fascia lata was done which was cut. The vastus lateralis was split in a L-shaped pattern and retracted, soft tissue was cleared to expose the bone. Excision of the cystic lesion along with extended curettage was done with phenol irrigation. A high-speed burr was used to augment the extended curettage. On intra-operative assessment following removal of the lesion, it was found that lateral wall had become papery thin with an unstable greater trochanter with a bone void large enough for us to warrant bone grafting. Anticipating a pathological post-operative fracture upon physiological loading following weight bearing over the limb by the patient, a prophylactic fixation was done with 130° dynamic hip screw plating along with tension band wiring of the greater trochanter to stabilise it (Fig. 3). Iliac crest bone graft as an autograft along with an allograft was added to augment the stability. The excised sample was sent for histopathological examination. Microscopically, it showed RBCs, hemosiderin deposits filling cystic-like spaces bounded by septae consisting of fibroblasts, spindle cells, calcification, and some scattered multi-nucleated giant cells. All these features were suggestive and confirmatory of an aneurysmal bone cyst (aka unicameral bone cyst) (Fig. 4).
Post-operative care
In the post-operative period, the patient was kept on complete bed rest for 2 weeks till suture removal; however, hip and knee range of motion exercises were started from post-operative day 3. Wound status was assessed by a check dress on post-operative day 3 and 7 and was found to be healthy. IV antibiotics were continued for 7-day post-operative. Suture removal was done after 2 weeks following surgery and the patient was discharged uneventfully. Following discharge, the patient has kept walker mobilization with partial weight bearing over the operated limb for 8 weeks. Hip and knee range of motion exercises were continued. From 2-month post-operative to 9-month post-operative, the patient was mobilized with partial to gradually increasing full weight bearing as tolerated when at the end of 1-year post-operative follow-up, the patient had gained full range of motion at the right hip which was painless.

ABC, though a non-neoplastic lesion can be locally aggressive and its pressure effects, can be detrimental to the bone, especially in the weight-bearing bones such as the proximal femur, which is one of the common sites for this lesion, thereby warranting an equally effective and aggressive treatment plan which involves surgical intervention [12]. Several treatment modalities have been described for ABC, such as curettage, curettage with bone grafting, or cementing, extended curettage with phenol irrigation, arterial embolization, adjuvant cryotherapy or radiotherapy, bone marrow injections, demineralized bone matrix applications, and segmental or en bloc resections. En bloc resection has the biggest advantage in that it is associated with the lowest recurrence rate, which is as low as 0% [13]. Here, we have a male patient who presented to us at 20 years of age with right-sided proximal femur aneurysmal bone cyst confirmed on histopathological examination. The patient was operated with an intra-lesional excision, extended curettage, high-speed burr, auto plus allograft with prophylactic fixation with dynamic hip screw plating with tension band wiring of the greater trochanter. The decision regarding prophylactic fixation with DHS plating was taken based on Mirels Classification for risk stratification of pathological fracture [14]. It is based on 4 domains, namely site of lesion, nature of lesion, size of the lesion, and pain. Minimum score is 4 and maximum is 12. Based on this, our patient had a Mirels score of 11. A score of >= 9 warrants prophylactic surgical fixation to prevent a pathological fracture [15,16]. The patient was first followed up after discharge at 1-year post-operative period when X-ray and CT scan were repeated (Fig. 5 and 6). The patient used walker for mobilization for 1 year following which he started walking without support with minimal complaints of pain while excessive exertion. Harris hip score was 82 (good) at 1-year follow-up and the patient had attained full range of motion at the right hip joint. After this, the patient was kept at 3-year follow-up with X-rays repeated at each follow-up which showed evidence of recurrence or of any implant failure (Fig. 7). The Harris hip score was calculated at each follow-up, which was seen to be improving thus correlating with the x-ray findings. It was 88, 92, and 95, respectively, with the last two being in the excellent category at 7 and 10-year follow-up, respectively. Implant removal was planned for the patient after the last follow-up based on patient willingness, through the same surgical approach (Fig. 8). The patient was kept partial weight bearing with walker assistance for 4 weeks following implant removal followed by full weight bearing with walker for another 4 weeks. At 6-month follow-up post-implant removal, CT scan was repeated along with X-rays, which showed complete resolution of the lesion, full consolidation with no evidence of recurrence. The patient attained painless full range of motion across the right hip joint with the Harris hip score being 96 (excellent) (Fig. 9-11). Historically, the management of ABC as described by Jaffe and Lichtenstein is curettage and reconstructing the defect with bone graft remains the mainstay of modern treatment. But as described sites such as proximal femur are prone to recurrence. Other methods such as en bloc excision of the lesion associated with lowest recurrence rates, when augmented with the use of radiotherapy which was used in the past give an even better result. However, both these methods are associated with problems. En bloc excision causes significant morbidity to the patient given the void it creates, namely post-operative pain, muscle weakness, decreased range of motion, and limb length discrepancies) [17]. Radiotherapy is usually used for malignancies but has provided satisfactory results in the treatment of ABCs, especially in cases that have recurred and are inoperable. However, Marcove et al. reported one case of radiation-induced sarcoma [18]. Papagelopoulos et al. also observed one case of radiation-induced sarcoma when he studied 52 patients with spinal ABCs treated with radiation [19].

Current-day treatment of ABC advocated by many is curettage with or without bone graft. To augment this procedure, high-speed burr has been described by one study done by Gibbs et al., [20] where 40 patients showed nearly 90% control rate after a median 7.2-year follow-up, following curettage, without the use of phenol, liquid nitrogen, or any other adjuvant. Burr works by mechanical disruption of the lesion to the level of the bone circumscribing the lesion. Phenol also used as adjuvant in extended curettage has been effectively used as a means to sterilize or wash the lesion following curettage, believed to be removing the remaining neoplastic cells [21]. Capanna et al., in a retrospective study, reported a 7% recurrence rate following curettage and phenol versus 41 % with curettage alone [22]. Bitzan et al. reported that curettage and phenol therapy advocated in 9 patients had no recurrences. As is clear here, considering all the aspects, intra-lesional excision, with extended curettage with phenol, high-speed burr, with auto plus allograft with prophylactic fixation with DHS plating led to no recurrence after 10-year follow-up, with no graft and implant failure, with no functional disability.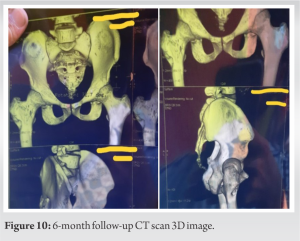

As is clear from this case, the treatment of an aneurysmal bone cyst needs to be individualized based on the patient’s age, complaints, and tumor behavior in terms of its aggressiveness, size, and its extent. Often, intra-lesional excision with extended curettage is required along with bone grafting and prophylactic fixation to support the bone graft and to prevent a pathological fracture and further recurrence. Other methods such as high-speed burr augment our outcome. Implant removal if indicated should be done after complete resolution of the lesion, patient willingness, and any other medical indication.
The treatment of ABCs, though individualized, mainly focuses on curettage and bone grafting. Other methods such as phenol irrigation, high-speed burr, and prophylactic fixation though case specific should be used to prevent recurrence and morbidity in the form of pathological fractures. We recommend that proximal femur ABCs should be treated as aggressive tumors and should treated be accordingly to get a favorable outcome as seen above in case followed up for 10 years.
References
- 1.Brindley GW, Greene JF Jr., Frankel LS. Case reports: Malignant transformation of aneurysmal bone cysts. Clin Orthop Relat Res 2005;438:282-7. [Google Scholar | PubMed]
- 2.Copley L, Dormans JP. Benign pediatric bone tumors. Evaluation and treatment. Pediatr Clin North Am 1996;43:949-66. [Google Scholar | PubMed]
- 3.Bonakdarpour A, Levy WM, Aegerter E. Primary and secondary aneurysmal bone cyst: A radiological study of 75 cases. Radiology 1978;126:75-83. [Google Scholar | PubMed]
- 4.Leithner A, Windhager R, Lang S, Haas OA, Kainberger F, Kotz R. Aneurysmal bone cyst. A population based epidemiologic study and literature review. Clin Orthop Relat Res 1999;363:176-9. [Google Scholar | PubMed]
- 5.Martinez V, Sissons HA. Aneurysmal bone cyst. A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61:2291-304. [Google Scholar | PubMed]
- 6.Rahman MA, El Masry AM, Azmy SI. Review of 16 cases of aneurysmal bone cyst in the proximal femur treated by extended curettage and cryosurgery with reconstruction using autogenous nonvascularized fibula graft. J Orthop Surg (Hong Kong) 2018;26: [Google Scholar | PubMed]
- 7.Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end‐result study using a new method of result evaluation. J Bone Joint Surg Am 1969;51:737-*55. [Google Scholar | PubMed]
- 8.Nilsdotter A, Bremander A. Measures of hip function and symptoms: Harris hip score (HHS), hip disability and osteoarthritis outcome score (HOOS), Oxford hip score (OHS), Lequesne index of severity for osteoarthritis of the hip (LISOH), and American Academy of Orthopedic Surgeons (AAOS) hip and knee questionnaire. Arthritis Care Res (Hoboken) 2011;63 S11:S200-7. [Google Scholar | PubMed]
- 9.Revel MP, Vanel D, Sigal R, Luboinski B, Michel G, Legrand I, et al. Aneurysmal bone cysts of the jaws: CT and MR findings. J Comput Assist Tomogr 1992;16:84-6. [Google Scholar | PubMed]
- 10.Mahnken AH, Nolte-Ernsting CC, Wildberger JE, Heussen N, Adam G, Wirtz DC, et al. Aneurysmal bone cyst: Value of MR imaging and conventional radiography. Eur Radiol 2003;13:1118-24. [Google Scholar | PubMed]
- 11.Park HY, Yang SK, Sheppard WL, Hegde V, Zoller SD, Nelson SD, et al. Current management of aneurysmal bone cysts. Curr Rev Musculoskelet Med 2016;9:435-44. [Google Scholar | PubMed]
- 12.Kapoor C, Shah M, Soni R, Patwa J, Merh A, Golwala P. Aneurysmal bone cyst of the proximal femur and its management - a case report. Cureus 2017;9:e991. [Google Scholar | PubMed]
- 13.Cole WG. Treatment of aneurysmal bone cysts in childhood. J Pediatr Orthop 1986;6:326-9. [Google Scholar | PubMed]
- 14.Mirels H. Metastatic disease in long bones. A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop Relat Res 1989;249:256-64. [Google Scholar | PubMed]
- 15.Jawad MU, Scully SP. In brief: Classifications in brief: Mirels’ classification: Metastatic disease in long bones and impending pathologic fracture. Clin Orthop Relat Res 2010;468:2825-7. [Google Scholar | PubMed]
- 16.Rockwood CA, Bucholz RW, Court-Brown CM, Heckman JD, Tornetta P. Rockwood and Green’s Fractures in Adults. Philadelphia, PA: Lippincott Williams & Wilkins; 2010. [Google Scholar | PubMed]
- 17.Flont P, Kolacinska-Flont M, Niedzielski K. A comparison of cyst wall curettage and en bloc excision in the treatment of aneurysmal bone cysts. World J Surg Oncol 2013;11:109. [Google Scholar | PubMed]
- 18.Marcove RC, Sheth DS, Takemoto S, Healey JH. The treatment of aneurysmal bone cyst. Clin Orthop Relat Res 1995;311:157-63. [Google Scholar | PubMed]
- 19.Papagelopoulos PJ, Currier BL, Shaughnessy WJ, Sim FH, Ebsersold MJ, Bond JR, et al. Aneurysmal bone cyst of the spine. Management and outcome. Spine (Phila Pa 1976) 1998;23:621-8. [Google Scholar | PubMed]
- 20.Gibbs CP Jr., Hefele MC, Peabody TD, Montag AG, Aithal V, Simon MA. Aneurysmal bone cyst of the extremities. Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-8. [Google Scholar | PubMed]
- 21.Capanna R, Sudanese A, Baldini N, Campanacci M. Phenol as an adjuvant in the control of local recurrence of benign neoplasms of bone treated by curettage. Ital J Orthop Traumatol 1985;11:381-8. [Google Scholar | PubMed]
- 22.Bitzan P, Windhager R, Lang S, Richling B, Kotz R. Incidence of recurrence of aneurysmal bone cysts following surgical treatment and adjuvant therapy with phenol. Z Orthop Ihre Grenzgeb 1995;133:422-8. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes
June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes June 1, 2026 Giant Cell Tumor of the Metacarpal Treated with Non-Vascularized Bone Graft: A Case
June 1, 2026 Giant Cell Tumor of the Metacarpal Treated with Non-Vascularized Bone Graft: A Case May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management
May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management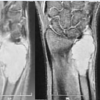 May 1, 2026 Journey and Roadblocks in the Management of Aneurysmal Bone Cysts in Patients with Unusual Presentations
May 1, 2026 Journey and Roadblocks in the Management of Aneurysmal Bone Cysts in Patients with Unusual Presentations