
Giant cell tumors should be considered a cause of loose bodies in the joint when there is a history of neighboring bone being treated for the same pathology and all such loose bodies removed should undergo histopathological examination.
Dr. MLV Sai Krishna, Department of Orthopaedics, Aayush Hospitals, Eluru, Andhra Pradesh, India. E-mail: krishna.mlv.sai@gmail.com
Abstract
Introduction: Loose bodies in the knee joint are relatively common and the common causes are transchondral fractures, synovial chondromatosis, osteochondritis dissecans, meniscal injury, and osteoarthritis. Neoplastic growths from synovium have been reported to have presentations mimicking loose bodies or meniscus tears.
Case Report: We report the case of an unusual cause of loose body in the knee joint of a 35-year-old male who reported for follow-up 3 years after the surgical management of giant cell tumor (GCT) of the distal femur. He had symptoms of loose bodies in the joint without any complaint specific to the operative site. Imaging revealed loose bodies within the joint which were removed arthroscopically. Histopathology showed the loose bodies as GCT. The patient had relief of symptoms after removal and the patient has no evidence of recurrence at the primary site or in the knee joint
Conclusion: GCTs should be considered a cause of loose bodies in the joint when there is a neighboring bone affected by GCT and all such loose bodies removed should undergo histopathological examination
Keywords: Knee, giant cell tumor, recurrence, loose bodies, arthroscopy.
Loose bodies in the knee joint are relatively common, and when freely mobile (unstable), they are prone to get entrapped between the articular surfaces causing intermittent joint locking, limitation of motion, pain, intra-articular effusion, and erosion of articular cartilage. The common causes of loose bodies in the knee joint taking into account the disease frequency include transchondral fractures, synovial chondromatosis, osteochondritis dissecans, and meniscal injury [1,2]. Osteoarthritis is a common cause of loose bodies in the old age [3]. A giant cell tumor (GCT) is a benign but locally aggressive bone tumor affecting the metaphyse-oepiphyseal region of the long bone. The distal femur is the most common site affected followed by proximal tibia [4]. Although the tumor commonly involves the subchondral bone intra-articular extension of GCT remains exceptional, even in cases with pathologic fracture [5], extended curettage and void filling with bone graft or acrylic cement is the standard treatment and is associated with a local recurrence rate of 10–20% [6]. We report the case of unusual cause of loose body in the knee joint which occurred 3 years after surgical management of GCT of distal femur.
A 35-year-old male presented to the follow-up clinic with complaints of something moving in the anterior aspect of his right knee joint. On examination, a firm non-tender mobile mass was palpable on the anterior aspect of the knee joint medial to the patellar ligament. Radiographs revealed a radio-opaque loose body on the anterior aspect medial to the patellar ligament.

Another radio-opaque loose body was present on the anterior aspect of the suprapatellar pouch which was asymptomatic for the patient (Fig. 1). He had undergone extended curettage and bone cementing for a Campanacci grade 1 GCT of the right distal femur 4 years back. The patient had an uneventful recovery after the surgery and returned to his profession. He did not have any pain or swelling at the operative site. There was no clinical or radiological feature suggestive of recurrence of the tumor. On arthroscopy of the right knee joint, the synovium, articular cartilage, menisci, and cruciate ligaments were found to be intact. Just distal to the inferior pole of the patella, a flattened loose body was found attached to the anterior medial capsule (Fig. 2).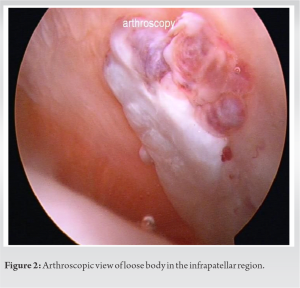
There was no donor site defect in the femur, tibia, or patella. The loose body was dissected with the help of punches and shaver from the capsule and then it was removed through the anteromedial portal. Another firm nodule was seen in the suprapatellar pouch covered with synovium (Fig. 3).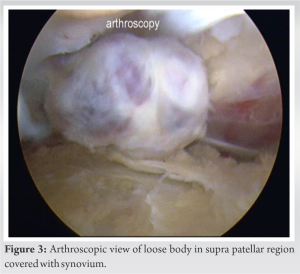
The synovium was resected with a shaver and the loose body was removed from the supero-medial portal. The loose bodies looked nodular and gray-black and firm in consistency. On dividing the loose body with a scalpel, it showed a bright red color (Fig. 4). Histopathology revealed it to be a GCT (Fig. 5). The patient had an uneventful recovery after the removal of loose bodies and is free of recurrence in the distal femur and knee joint 2 years post-loose body removal.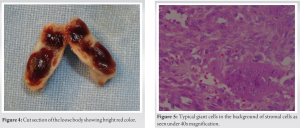
GCT is a common tumor in South-east Asia and is most commonly located around the distal femur [7]. The most accepted treatment for this tumor is extended curettage and bone grafting or cement packing. The rate of recurrences of this tumor ranges from 10% to 20% and most of the recurrence occur within the first 2 years [5]. These recurrences occur at the original site and are evident clinically in swelling and pain. Radiologically, it shows destruction of bone, expansion of bone, breach of cortex, and soft-tissue mass. The recurrences occur at the original site and the most accepted reason for this is the incomplete removal of the tumor. In our case, the original site, the distal femur, did not have any clinical or radiological signs of recurrence of the tumor. The complaint was localized to the knee joint cavity and not the distal femur. This kind of recurrence has not been reported before. The possible mechanism for this spillage of tumor cells during the initial surgery and these cells multiplied to form “loose bodies” in the joint. Such kind of tumor spillage is very difficult to control during manual curettage and extended curettage with a burr. Lavage with copious amounts of saline after the surgery can wash away such tumor cell spillage and prevent recurrence. We could not find any similar case reported in the literature. Although neoplastic growths from synovium have been reported to have presentations mimicking loose bodies or meniscus tears, the neoplasms of bone have not been reported as a cause of loose bodies in the joint [8,9,10]. Although GCTs of the bone and tenosynovial GCT have similarities in their nomenclature with similar macroscopic appearance, they are two clinically distinct entities and we could not find any literature regarding their simultaneous occurrence [11]. In our patient apart from the loose bodies and the prior history of surgery, there were no other complaints. During arthroscopic removal of these loose bodies, they had to be dissected from the underlying and overlying synovium using punch and shaver. During this procedure, it is difficult to limit and control the spill of the tumor cells from these loose bodies. Although there has been no recurrence after this removal of loose bodies, we are not sure whether open removal of this kind of loose bodies would have been a better option.
GCTs should be considered a cause of loose bodies in the joint when there is a neighboring bone affected by GCT and all such loose bodies removed should undergo histopathological examination.
Loose bodies in the knee joint are relatively common. Neoplastic growths from synovium have been reported to have presentations mimicking loose bodies or meniscus tears and even neoplastic growths of the neighboring bones should be included in the differentials and all such loose bodies should undergo histopathology.
References
- 1.Dandy DJ, O’Carroll PF. The removal of loose bodies from the knee under arthroscopic control. J Bone Joint Surg Br 1982;64:473-4. [Google Scholar | PubMed]
- 2.Zmerly H, Moscato M, Akkawi I. Assessment and management of loose bodies in the knee joint and related disease: A narrative review. Curr Rheumatol Rev 2022;18:12-9. [Google Scholar | PubMed]
- 3.Ahn JH, Yoo JC, Lee SH. Arthroscopic loose-body removal in posterior compartment of the knee joint: A technical note. Knee Surg Sports Traumatol Arthrosc 2007;15:100-6. [Google Scholar | PubMed]
- 4.Unni KK, Inwards CY. Dahlin’s Bone Tumors: General Aspects and Data on 10,165 Cases. Philadelphia, PA: Lippincott Williams & Wilkins; 2009. [Google Scholar | PubMed]
- 5.Turcotte RE. Giant cell tumor of bone. Orthop Clin North Am 2006;37:35-51. [Google Scholar | PubMed]
- 6.Klenke FM, Wenger DE, Inwards CY, Rose PS, Sim FH. Recurrent giant cell tumor of long bones: Analysis of surgical management. Clin Orthop Relat Res 2011;469:1181-7. [Google Scholar | PubMed]
- 7.Sung HW, Kuo DP, Shu WP, Chai YB, Liu CC, Li SM. Giant-cell tumor of bone: Analysis of two hundred and eight cases in Chinese patients. J Bone Joint Surg Am 1982;64:755-61. [Google Scholar | PubMed]
- 8.Naranje S, Mittal R. Knee locking and pain mimicking lateral meniscal tear due to unusual location of localized pigmented villonodular synovitis: A diagnostic surprise. Eur J Orthop Surg Traumatol 2011;21:131-3. [Google Scholar | PubMed]
- 9.Kanagawa H, Niki Y, Matsumoto H, Kosaki N, Enomoto H, Morioka H, et al. Localized pigmented villonodular synovitis presenting as a loose body following minor trauma in the knee: A case report. Knee 2007;14:395-7. [Google Scholar | PubMed]
- 10.Woods C Jr., Alade CO, Anderson V, Ashby ME. Pigmented villonodular synovitis of the knee presenting as a loose body. A case report. Clin Orthop Relat Res 1977;129:230-1. [Google Scholar | PubMed]
- 11.Kropivšek L, Pižem J, Mavčič B. Giant cell tumor of bone versus tenosynovial giant cell tumor - similarities and differences. Int J Surg Pathol 2022;30:596-605. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Secondary Synovial Chondromatosis of the Shoulder Associated with Rotator Cuff Tear: Diagnostic Challenge and Arthroscopic Management – A Case Report
June 1, 2026 Secondary Synovial Chondromatosis of the Shoulder Associated with Rotator Cuff Tear: Diagnostic Challenge and Arthroscopic Management – A Case Report May 1, 2026 Simultaneous Anterior Cruciate Ligament Avulsion Fracture with Bilateral Posterior Meniscal Root Tears of the Knee: A Case Report
May 1, 2026 Simultaneous Anterior Cruciate Ligament Avulsion Fracture with Bilateral Posterior Meniscal Root Tears of the Knee: A Case Report April 1, 2026 Bucket Handle Tear of the Medial Meniscus with a New Magnetic Resonance Imaging Sign: The “Head in the Sand Sign” – A Case Report
April 1, 2026 Bucket Handle Tear of the Medial Meniscus with a New Magnetic Resonance Imaging Sign: The “Head in the Sand Sign” – A Case Report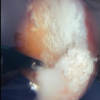 February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report
February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report