
For circumferential degloving injuries of the hand with a large raw area, latissimus dorsi free flap in a wrapping fashion provides a reasonable alternative for coverage.
Dr. Chaitanya Dodakundi, Department of Trauma and Orthopedics, Hand and Microsurgery Unit, Rashid Hospital, Dubai Health, Dubai, United Arab Emirates. E-mail: chaitu123in@gmail.com
Abstract
Introduction: Circumferential multiplanar degloving injuries of hand and wrist are devastating injuries which can severely compromise what is salvageable for achieving a functional hand, ending in amputations if not well managed.
Case Report: We described a complete multiplanar degloving injury of hand in a 27-year-old Asian male due to a compressing machine, which was successfully salvaged with a complete free latissimus dorsi flap cover with skin graft for coverage.
Conclusion: An unconventional one-stage surgical option for soft-tissue coverage using a complete latissimus dorsi free flap ending in a reasonably functional two-fingered hand.
Keywords: Degloving, multiplanar, coverage.
Avulsion injuries of the hand and/or fingers are common industrial accidents which are seen in emergency on daily basis. However, complete degloving avulsion injuries of the hand are serious injuries which are less common, which cause considerable challenges to a hand surgeon in terms of obtaining a functional hand, with sensation and contour/esthetic appearance [1]. A majority of total hand degloving injuries are mechanical injuries, and the degree of injury is related to the force of tearing, extrusion, and rolling [2]. Surgical decision-making involves looking through a crystal ball with retaining what is viable, what is reconstructable, and what can be done to improve the hand function in the long term. Free flaps are a viable option [3,4], with other flaps have been described [5]. Groin flap and its modifications are considered a classical workhorse in degloving injuries [6,7]. We present a similar case of total circumferential degloving injury of hand with a viable middle intervening finger – which was challenging in retaining what was viable and what was reconstructable.
A 27-year-old male presented to us with complete degloving injury of the right hand, sustained when the hand was pulled by him reflexly while it was stuck in a compressing machine (for packing tissue paper). On examination, the hand was degloved from just proximal to wrist level with complete loosening of the whole integument except part of the skin covering the middle finger (Fig. 1). All fingers were degloved with doubtful viability. X-ray revealed fractures of proximal phalanges of the index, ring, and little fingers.(Fig. 1-d)

He was immediately taken up for emergency surgical exploration, fixation with k wires, and repair to restore what would be viable. After saline irrigation and fixation of phalangeal fractures, it was noted that the radial and ulnar arteries all the way to the carpal arch were intact and the veins draining hand were also intact but stretched with severe crushing when examined under microscope. Considering the vascularity improved after surgical fixation along with these findings, it was decided to observe how this would progress. However, from post-operative day 2 the hand was getting edematous and showing up signs of compromised vascularity (Fig. 2a and 2b).

He was managed with the removal of a few tight sutures after which the hand was showing signs of improved vascularity but ultimately – probably due to segmental intimal damages whole of the degloved hand had become necrotic and non-viable except the middle finger by 7th post operative day (Fig. 3a and 3b).
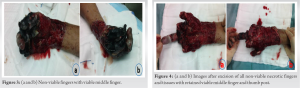
He was taken up for debridement and all the non-viable tissues were thoroughly debrided leaving a hand with retained middle finger and part of the thumb till interphalangeal joint (Fig. 4a and 4b).
Considering the presence of a viable middle finger and a thumb osteoligamentous framework available, he was taken up for coverage with a free latissimus dorsi flap with skin grafting (Fig. 5a to 5c). He underwent uneventful post-operative recovery and once the flap was settled he was taken up for debulking and first web deepening leaving a hand which was functionally able to hold things, write, and do his activities of daily living (Fig. 6a to 6c).

Clinical entity of degloving injury implies that the skin is lost but the musculoskeletal unit is intact, and hence the movements of the part can be preserved by a thoroughly well-planned reconstruction [8]. Multiple techniques are described in the literature for management of a total degloving injury of the hand ranging from Bilobed groin flaps, the combination of Groin and abdominal flap, compartmentalized abdominal flap and free anterolateral thigh flaps etc. [9] In all methods followed, the principles remain to provide thin, pliable and sensate skin that prevents contracture and stiffness, to allow the reconstructed tissue to heal quickly, to allow early mobilization, to provide skin durable enough to withstand a secondary surgical procedure and to create a result that is cosmetically acceptable [8]. What was peculiar in this case after stage debridement to retain what was viable and reconstructable was that the intervening middle finger with complete skin cover where attaching a pedicled skin flap/random flap becomes tricky considering the narrow skin edge for inset and the positioning to retain the fragile vascularity in the middle finger till the whole flap heals. Pocketing the degloved hand was not an option as the middle finger with viable skin could not allow this to be done. Hence, it was planned to do single-stage coverage with a free latissimus dorsi flap with skin graft which bought in its own vascularity after anastomosis with the donor vessels (radial artery and veins in forearm.) and did not depend on the vascularity of middle finger to heal. This large flap entailed complete coverage in a single stage with an uneventful post-operative recovery. He further underwent 1st web deepening around 6 months after flap settling and was able to have a two-fingered hand capable of holding a spoon, writing, and typing which helped him in his activities of daily living. At the last follow-up, even though objectively his sensory assessment was not substantial, he was able to sense through the flap items held in his hand probably due to the proprioceptive feedback from the finger joints, retained sensate middle finger, and abundant sensory nerve endings in the degloved hand. However, there are some fallacies which we would like to mention here in retrospect which included our failure to plan for an aggressive excision of the degloved segments in the form of excision of distal phalanges and flap cover which has been a method followed in multiplanar circumferential degloving injuries of hand [10]. In carefully selected patients with complete hand multiplanar degloving injury, this type of muscle flap also can be an option for coverage with providing a functionally salvageable hand, where the surgeon should try to see through the crystal ball what the hand would look like finally and counsel in detail the same to the patient.
An unconventional one-stage surgical option for soft-tissue coverage using a complete latissimus dorsi free flap ending in a reasonably functional two-fingered hand for a case of complete degloving with retained viable middle finger.
A complete degloving injury of the hand with partly retained viable fingers is a challenging case for any hand surgeon for providing coverage keeping in view the multiple reconstructive procedures needed in the future for providing a functional hand. By describing, this method of using a complete latissimus dorsi free flap for coverage in such cases, we would mention that this could also be an option in such difficult cases for coverage.
References
- 1.Heath PM, Jackson IT, Cooney WP 3rd, Morgan RG. Simultaneous bilateral staged groin flaps for coverage of mutilating injuries of the hand. Ann Plast Surg 1983;11:462-8. [Google Scholar | PubMed]
- 2.Wong LK, Nesbit RD, Turner LA, Sargent LA. Management of a circumferential lower extremity degloving injury with the use of vacuum-assisted closure. South Med J 2006;99:628-30. [Google Scholar | PubMed]
- 3.Vedder N, Hanel D. The mangled upper extremity. In: Wolfe SW, Hotchikiss RN, Pederson WC, Kozin SH, editors. Green’s Operative Hand Surgery. 6th ed. Philadelphia, PA: Elsevier; 2011. p. 1603-44. [Google Scholar | PubMed]
- 4.Pederson WC. Upper extremity microsurgery. Plast Reconstr Surg 2001;107:1524-37; discussion 1538-9, 1540-3. [Google Scholar | PubMed]
- 5.Hallock G. The utility of both muscle and fascia flaps in severe upper extremity trauma. J Trauma 2002;53:61-5. [Google Scholar | PubMed]
- 6.McGregor IA, Jackson IT. The groin flap. Br J Plast Surg 1972;25:3-16. [Google Scholar | PubMed]
- 7.Lister GD, McGregor IA, Jackson IT. The groin flap in hand injuries. Injury 1973;4:229-39. [Google Scholar | PubMed]
- 8.Krishnamoorthy R, Karthikeyan G. Degloving injuries of the hand. Indian J Plast Surg 2011;44:227-36. [Google Scholar | PubMed]
- 9.Lin TS. One-stage debulking procedure after flap reconstruction for degloving injury of the hand. J Plast Reconstr Aesthet Surg 2016;69:646-51. [Google Scholar | PubMed]
- 10.Kim MJ, Park BY. From mitten hand to five individual fingers: One-stage coverage using a deep inferior epigastric perforator free flap for an extensive degloving hand injury. J Reconstr Microsurg Open 2018;3:e28-31. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 From Hip Effusion to Hemophilia: Unveiling the Cause of Pain in 6-Month-Old Infant. A Case Report
January 1, 2026 From Hip Effusion to Hemophilia: Unveiling the Cause of Pain in 6-Month-Old Infant. A Case Report September 1, 2025 Suprapectineal Plate for Fixation of Both Columns of Complex Acetabular Fractures in a Single Sitting through Anterior Approach- Pushing the Boundaries with the New “Gold Standard”
September 1, 2025 Suprapectineal Plate for Fixation of Both Columns of Complex Acetabular Fractures in a Single Sitting through Anterior Approach- Pushing the Boundaries with the New “Gold Standard” January 1, 2025 Metallosis, Trunnionosis, and Head-stem Dissociation of the Exeter v40 Stem in a Metal-on-Metal Hip: A Unique Case
January 1, 2025 Metallosis, Trunnionosis, and Head-stem Dissociation of the Exeter v40 Stem in a Metal-on-Metal Hip: A Unique Case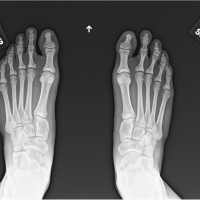 December 10, 2023 Short-term Follow-up of Patients Receiving Bio-integrative Screws for Lisfranc Injuries: A Case Series
December 10, 2023 Short-term Follow-up of Patients Receiving Bio-integrative Screws for Lisfranc Injuries: A Case Series