
In rare cases like aneurysmal bone cysts, particularly those involving the femoral head,a trapdoor osteotomy stabilized with bone grafting yields excellent functional and radiological outcomes, presenting a viable treatment option alongside the conventional curettage and bone grafting techniques.
Dr. Raunak Dhawale, Senior Resident , Department of Orthopaedics, Government Medical College and Hospital , Nagpur 43GW+CR2, Hanuman Nagar, Ajni Rd, Nagpur, Maharashtra 440003, India. E-mail: drraunak.dhawale@gmail.com
Abstract
Introduction : Aneurysmal Bone Cyst (ABC) is a benign, non neoplastic, expansile lesion of bone characterized by channels of blood and spaces separated by fibrous septae . ABC of femoral head is an extremely rare condition and is difficult to treat as the surgical approach is a dilemma .
Case report: We hereby report a case of aneurysmal bone cyst in femoral head of a 19 year old female patient .To preserve the vascularity of the femoral head , we approached the lesion by ganz safe surgical dislocation of the affected femoral head, trapdoor procedure of femoral head followed by curettage and bone grafting . The patient was followed up for 6 months & at latest follow up , lesion has healed completely & patient is walking pain free .
Conclusion: In rare cases like ABC of femoral head, a trapdoor osteotomy of femoral head with bone grafting followed by stabilization of the bone graft and osteotomy gives excellent functional and radiological outcomes.
Keywords : aneurysmal bone cyst, safe surgical dislocation, trapdoor procedure, bone grafting, femoral head
The nature, characteristics, and best treatment strategy for aneurysmal bone cysts are still unknown despite a more than 60-year description history [1 ]. Patients seem to develop these lesions more frequently throughout their first twenty years of life [2,3] and females appear to develop lesions slightly more frequently than males [2]. The femur, tibia, humerus, spine, and pelvis are the main sites of occurrence, according to a literature [3]. These tumours are typically metaphyseal or diaphyseal and are frequently positioned eccentrically, which is a crucial radiographic feature [3]. The lesions exhibits substantial cortical thinning over the site with little to no bone development. Recurrence rates continue to range from 5% to more than 40% [4]. The accepted modalities of treatment are curettage and the placement of a bone graft or polymethylmethacrylate . Sclerosing agents, bone substitutes, and other agents have been used by various authors but have been found to be less successful than traditional curettage in various trials [5]. ABC of femoral head is a rare condition encountered amongst the variety of locations.
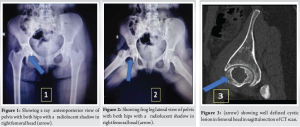
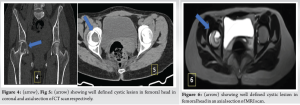
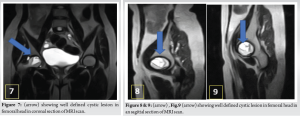
A 19-year-old female came walking into the out patient department with complaints of right hip pain since a year. There was no history of fall. On further examination she had anterior joint line tenderness and painful rotations of hip, abduction was normal .On radiological examination Fig.1, Fig.2 a radiolucent shadow was noted in the right femoral head. CT scan was done and a well-defined cystic lesion was confirmed in the antero-medial part of femoral head across various sections Fig.3, Fig.4, Fig.5; & similar findings were noted on MRI Scan as well Fig.6, Fig.7, Fig.8, Fig.9.
Because of the rare location of the cyst, biopsy was very difficult and some imaging features were suggestive of a benign cystic lesion, definitive surgical procedure was planned. With the patient under general anaesthesia, in left lateral position, Anterolateral approach to right hip was taken. Incision was taken starting just in front of GT, TFL reflected on either side Fig.10, Fig.11. A step cut trochanteric flip osteotomy of greater trochanter was done , joint capsule was exposed & cut in Z fashion followed by safe surgical dislocation of femoral head preserving its vascularity .

A trapdoor was created over the affected area of femoral head Fig.12, Fig.13. The trapdoor cartilage was elevated and a sort of window was created at the affected part of femoral head to access the lesion. The lesion was seen extending upto the calcar region & a thorough curettage was done. The size of the lesion was approximately 3.2 x 2.4 x4 cm (Anteroposterior x Mediolateral x Superoinferior). A sample of the removed tissue was sent for histopathological examination. Ipsilateral tricortical bone graftfrom iliac crest was prepared in adequate fashion to fit in the femoral head defect & packed around with cancellous bone graft.

It was held in place with a single herbert screw & the cartilage was put back over the defect. The hip was reduced, capsule closed, the greater trochanteric osteotomy was fixed with two 6.5mm cannulated cancellous screws across osteotomy site Fig.14, Fig.15. Post operative radiograph were done Fig.16, Fig.17. The histopathology report was confirmed the clinical suspicion of Aneurysmal bone Cyst. The patient was mobilised post operatively with non weight bearing mobilization with walker for 3 months with passive, active assisted hip range of motion exercises, then shifted to partial weight bearing with walker for 1 month, and later full weight bearing. The patient was followed up for 2 years, had good radiological union & a decent range of motion. Fig. 18, Fig. 19, Fig. 20 CT scan of right hip at 1 year follow up showing complete consolidation of osteotomy site and femoral head bone grafting site in Coronal, Axial and Sagittal sections respectively. Fig. 21, Fig.22 Showing complete consolidation of osteotomy site and femoral head bone grafting site with head contour maintained as seen in anteroposterior and frog leg lateral view respectively.


Fig. 23 showing active hip flexion of 90 degree at 2 years follow up. Fig. 24 showing patient standing independently at 2 years follow up. The patient did not want any further surgery for removal of the two 6.5 mm cannulated cancellous screws after complete consolidation of the osteotomy site.
ABC is primarily seen in children and adolescents with 80% cases occurring in patients less than 20 years age. When determining the extent of the lesion and making the diagnosis, CT and MRI are frequently helpful. An open biopsy with frozen section is frequently required prior to final treatment [2,3,6]. Both long and short tubular bones exhibit a predominance of ABC at the metaphyseal region. Only 30% of patients had ABC that only affected the metaphysis, 28% had metadiaphyseal, 24% had epi-metaphyseal, 10% had ABC that only affected the diaphysis, and 8% had ABC that affected the entire tubular bone [7]. The association between ABC and physis in long and short tubular bones has been investigated in light of the typical metaphyseal position and young age of the patients. The physis was crossed in 23% of individuals with an open physis which is rare for bone tumours. The physeal scar was crossed in 68% of cases following closure [7]. Wide excision with or without radiation therapy, curettage (intralesional excision), curettage with postoperative radiation therapy, wide amputation with radiation therapy, and many other forms of treatment were utilised and documented. When necessary, bone grafting was carried out [7]. According to Qi Cheng et al, a modified trapdoor approach was used in patients with femoral head Osteonecrosis and ARCO stage III, in which an autologous tricortical iliac block graft mixed with morselized bone was implanted following thorough debridement broken cartilage and necrotic subchondral bone were no longer replanted, which was associated with superior clinical and radiographic results than the light bulb method. For 67 hips, the clinical success rate (good or excellent outcome) was 92.5% [8]. Other known treatment modalities as per literature are high speed burr, en bloc excision, argon beam coagulation, arterial embolization, radiotherapy, cementing, use of phenol, percutaneous doxycycline, sclerotherapy, cryosurgery, curopsy, adjuvant radiotherapy and bisphosphonate medical therapy [9]. In a study published by Skubitz et al where a 27 year old man had a large sacral aneurysmal bone cyst was treated with Inj. Denosumab 120mg every month for a year after an initial dose, it healed completely and patient had pain relief in 2 months and showed radiological improvement within a year [10]. We utilised a similar trapdoor approach to overcome the challenges in our case. Our patient was a 19 year old female, the physis was already closed and the lesion was present in the weight bearing area of femoral head. The step cut trochanteric flip osteotomy helped in a better exposure of the hip and to preserve the vascularity of the femoral head. It was later fixed to allow the abductor function. The lesion was confirmed to be ABC on intra operative specimen of curettage sent for histopathology. In literature there has been mention of proximal femur ABC but no specific mention of ABC of femoral head. Since the weight bearing area of the femoral head was involved, it was essential to not only do thorough curettage of the lesion but also fill the void with bone grafting and ipsilateral iliac crest tricortical bone grafting with cancellous bone packing around the graft was a good available option. The herbert screw stabilised the graft was buried as the same time to allow the trapdoor of cartilage cover was made to sit back onto window created, thus getting the trapdoor back in its original place.
Treatment for aneurysmal bone cysts is difficult because they are aggressive benign tumours and have high recurrence rates. Curettage and bone grafting are the mainstay of care. In rare scenarios like ABC of femoral head, we recommend the use of trapdoor osteotomy of femoral head stabilized with bone grafting in the form of allograft or autograft for excellent functional and radiological outcomes.
Aneurysmal bone cysts (ABC) pose therapeutic challenges due to their aggressive nature and high recurrence rates. While curettage and bone grafting remain standard modalities of treatment, cases involving the femoral head necessitate nuanced approaches. Our study advocates for trapdoor osteotomy coupled with bone grafting, showcasing promising functional and radiological outcomes. This strategy, though rare, offers a viable alternative to conventional methods, particularly in complex ABC presentations. By incorporating meticulous surgical techniques and personalized grafting solutions, such as allograft or autograft, orthopaedicians can achieve optimal patient outcomes. This underscores the importance of tailored interventions in managing ABCs, emphasizing the role of comprehensive treatment strategies in addressing complex bone pathologies. Also intraoperative complications like blood loss, inadequate bone grafting and stabilizing implants for the the graft and the osteotomy are of utmost importance.
References
- 1.Jaffe HL, Lichtenstein L: Solitary unicameral bone cyst: With emphasis on the roentgen picture, the pathologic appearance and the pathogenesis. Arch Surg 44:1004-1025, 1942 [Google Scholar | PubMed]
- 2.Campanacci M: Aneurysmal bone cyst, in Campanacci M (ed): Bone and Soft Tissue Tumors (ed 2). New York, NY, Springer Verlag, 1999, pp 812-840 [Google Scholar | PubMed]
- 3.Dorfman HD, Czerniak B: Cystic lesions, in Dorfman HD, Czerniak B (eds): Bone Tumors. St Louis, MO, Mosby, 1998, pp 855-912 [Google Scholar | PubMed]
- 4.Ozaki T, Hillmann A, Lindner N, et al: Aneurysmal bone cysts in children. J Cancer Res Clin Oncol 122:767-769, 1996 [Google Scholar | PubMed]
- 5.Topouchian V, Mazda K, Kamze B, et al: Aneurysmal bone cysts in children: Complications of fibrosing agent injections. Radiology 232:522-526, 2004 [Google Scholar | PubMed]
- 6.Mahnken AH, Nolte Ernsting CC, Wildberger JE, et al: Aneurysmal bone cyst: Value of MR imaging and conventional radiogra- phy. Eur Radiol 13:118-124, 2003 [Google Scholar | PubMed]
- 7.Aneurysmal bone cyst : A clinicopathological Study of 238 cases Ariel M. Vergel De Dios , MD , Jeffrey R. Bond , MD et all , CANCER June 15 1992 , Volume 69 , No. 12 [Google Scholar | PubMed]
- 8.Qi Cheng , Feng – chao Zhao et al : Modified trapdoor procedures using autogenous tricortical iliac graft without preserving the broken cartilage for treatment of osteonecrosis of the femoral head: a prospective cohort study with historical controls , Journal of Orthopaedic Surgery and Research volume 15, Article number: 183 (2020) [Google Scholar | PubMed]
- 9.Current management of aneurysmal bone cysts Howard Y Park , Sara K. Yang, et al 2016 Dec; 9(4): 435- Published online 2016 Oct 24. doi: 10.1007/s12178-016-9371-6 [Google Scholar | PubMed | CrossRef]
- 10.Response of Aneurysmal Bone Cyst to Denosumab . Skubitz, Keith M. MD*; Peltola, Justin C. MD†; Santos, Edward R. MD‡; Cheng, Edward Y. MD‡ Spine 40(22):p E1201-E1204, November 15, 2015. | DOI: 10.1097/BRS.0000000000001027 [Google Scholar | PubMed | CrossRef]







Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Aneurysmal Bone Cyst Presenting as a Pathological Subtrochanteric Femur Fracture in an Adolescent: A Case Report
May 1, 2026 Aneurysmal Bone Cyst Presenting as a Pathological Subtrochanteric Femur Fracture in an Adolescent: A Case Report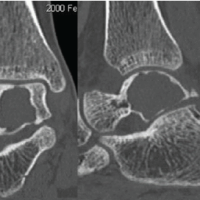 September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report
September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes
June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management
May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management