
The full endoscopic inter-laminar approach is a minimally invasive and effective treatment option for giant synovial cysts of the lumbar spine, providing symptom relief without the need for fusion and instrumentation
Dr. Mohammad Badra, Department of Orthopedic Surgery, Faculty of Medicine, Balamand University, Beirut, Lebanon, Department of Orthopedic Surgery and Traumatology, Clemenceau Medical Center, Johns Hopkins International, Beirut, Lebanon. E-mail: mbadra13@gmail.com
Abstract
Introduction: Synovial cysts of the lumbar spine are rare pathologies that can cause significant nerve root compression. Traditional surgical treatments often involve open laminectomy with medial facetectomy, which often lead to instability requiring fusion and instrumentation. We present a case of a giant synovial cyst at the L4–L5 level successfully treated using full endoscopic inter-laminar approach.
Case Report: A 69-year-old male presented with chronic low back pain and left leg radiculopathy. Imaging revealed a giant synovial cyst at L4–L5 level causing severe significant nerve root compression. The patient underwent a full endoscopic inter-laminar approach for total excision of the cyst. Postoperatively, the patient’s symptoms resolved, without cyst recurrence or instability at 1 year.
Conclusion: Endoscopic total excision of giant synovial cysts is a surgical option that can effectively address symptoms while minimizing the risk of segmental instability. This case demonstrates the feasibility and benefits of this minimally invasive approach.
Keywords: Synovial cyst, spine, endoscopy, fusion, instability.
Synovial cysts of the lumbar spine are uncommon pathologies occurring in approximately 6.5% of patients undergoing lumbar magnetic resonance imaging (MRI), with a majority resulting from degenerative changes in the facet joints [1]. It occurs most commonly at the L4–5 level of the lumbar spine [1], which is the most mobile segment and thus most susceptible to degenerative changes. Synovial cysts of the lumbar spine can cause back pain along with radicular symptoms secondary to nerve root compression [2]. The traditional and the standard surgical treatment of lumbar facet cysts is usually open laminectomy for excision of the cyst along with medial facetectomy which can cause further instability of the spinal segment [2,3]. Giant synovial cysts of the lumbar spine are rare pathologies and their excision requires more expansile approach with more bone removal and often requires additional fusion and instrumentation of the affected spinal segment [4]. We present here a case of giant synovial cyst of the lumbar spine at L4–5 level that was associated with stable degenerative spondylolisthesis that was excised totally using the full endoscopic inter-laminar approach. One-year follow-up radiographs showed no further progression of the spondylolisthesis and no recurrence of the synovial cyst.
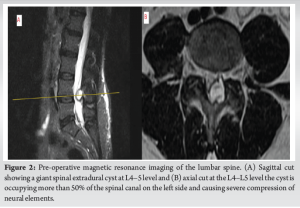
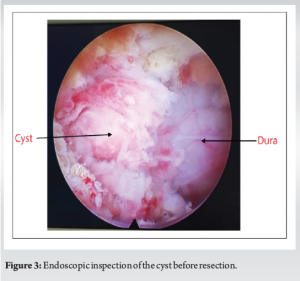
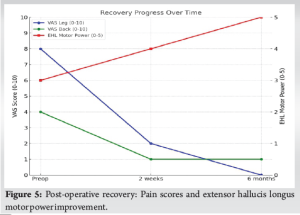
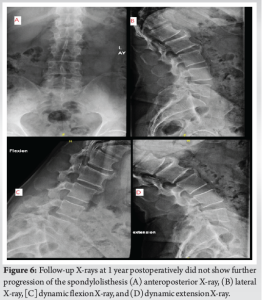
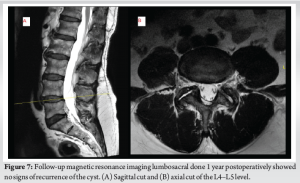
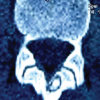
This 69-year-old male patient presented to our clinic at Clemenceau Medical Center with chronic history of low back pain that was exacerbated in the past 6 months and associated with the left leg radicular pain and numbness along the L5 dermatome. Physical examination showed weakness in the left foot dorsiflexion (4/5) and big toe (2/5). Pre-operative X-ray of the lumbosacral spine showed a Grade 1 degenerative spondylolisthesis at L4–5 that was stable on dynamic views (Fig. 1), and pre-operative MRI of the lumbar spine showed a giant spinal extradural cyst at L4–5 level occupying more than 50% of the spinal canal on the left side and causing severe compression of neural elements (Fig. 2). The surgical options including the possibility of decompression and fusion and instrumentation were discussed with the patient who refused the idea of the fusion procedure. The procedure was performed under general anesthesia while the patient was placed in a prone position. Under fluoroscopy control, the L4–5 interlaminar space on the left side was identified and marked. A 10 mm skin incision was made, and a 9.4 mm outer diameter dilator was inserted up to the ligamentum flavum followed by insertion of the beveled working sleeve with an outer diameter of 10.5 mm. The endoscope (Vertebris stenosis scope, Richard Wolf – Germany) was then introduced. A radiofrequency ablator was used to expose the upper lamina (L4), the lower lamina (L5), and the medial aspect of the facet joint. Using different types of endoscopic burrs and Kerrison punches, 3–4 mm of bone were resected from the L4–5 medial facet initially and then burring was carried out at the inferior aspect of the L4 lamina and superior aspect of the L5 lamina until sufficient exposure of the borders of the cyst can be clearly seen cranially, caudally, and laterally (Fig. 3). The cyst was resected totally in a piecemeal fashion. Endoscopic inspection of the dura and left L5 nerve root showed complete decompression of the neural elements (Fig. 4). The motor power of the patient’s extensor hallucis longus was 3/5 preoperatively, improving to 4/5 at 2 weeks and reaching 5/5 at 6 months. The visual analog scale (VAS) leg pain score was at 8/10 preoperatively, decreased significantly to 2/10 at 2 weeks, and resolved completely to 0/10 at 6 months. Similarly, the VAS back pain score was 4/10 preoperatively, which reduced to 1/10 at 2 weeks and remained stable at 1/10 at 6 months (Fig. 5). Follow-up dynamic X-rays of the lumbar spine 1 year postoperatively did not show further progression of the L4–5 spondylolisthesis (Fig. 6) and follow-up MRI done 1 year postoperatively did not show signs of recurrence of the cyst (Fig. 7). The mini-incision site immediately postoperatively (day 0) and at 2 weeks showed satisfactory healing with no signs of infection or complications (Fig. 8).



Synovial cysts of the lumbar spine are fluid-filled sacs that can cause radicular symptoms secondary to mechanical compression on the surrounding spinal nerves [5]. They develop from inflamed synovial lining of the degenerated facet joints and can vary widely in size from a small cyst (<5 mm in diameter) that is totally asymptomatic to a large (more than 1.5 cm in diameter) giant cyst that can cause major nerve compression resulting in pain, discomfort, and even cauda equina syndrome [6]. In our patient, the synovial facet cyst occupied more than 50% of the spinal canal and caused motor weakness in the foot dorsiflexion. Surgical treatment of symptomatic synovial cyst in the lumbar spine is controversial, ranging from simple cyst excision, either through open techniques or minimally invasive techniques to laminectomy with medial facetectomy along with fusion and instrumentation. Selection of the surgical approach usually depends on several factors, mainly the size of the cyst, its location within the spinal canal, and the presence or absence of instability [7]. Excision of large facet cysts through the traditional open technique sometimes entails full laminectomy with resection of a major part of the facet joint that might lead to segmental instability and subsequent fusion and instrumentation [4]. Full endoscopic excision of spinal extradural cysts has been well described in the literature [8-12]. A study on 74 patients with facet synovial cysts was followed up for up to 2 years following full-endoscopic inter-laminar and transforaminal technique. About 85% of the patients reported no leg pain, and 11% experienced occasional pain with a low complication rate [12]. Another study reported on 11 patients with lumbar synovial cyst treated using an endoscopic tubular retractor system. Preoperatively, instability in the form of G (Grade) 1 spondylolisthesis was noted in four patients. At follow-up, ten patients reported no leg pain (90.9%), and none of the patient required further surgical intervention or subsequent fusion procedure [8]. In another study, eight patients with symptomatic lumbar juxtafacet cyst were treated using the full endoscopic technique with excellent clinical outcome [9]. One study showed that minimally invasive surgery significantly alleviated leg pain and radicular symptoms compared to open surgery, while there were no notable differences in back pain or neurogenic claudication. Patients in the minimally invasive surgery group experienced shorter hospital stays and less post-operative pain. However, no significant disparities were observed in surgical duration, complication rates, cyst recurrence, or the need for fusion surgery [13]. Endoscopic total excision of large synovial facet cysts and minimal injury to the facet joint and subsequent segmental instability is considered technically challenging. In our case, total excision the cyst was performed with minimal bony resection from the medial facet and no further instability was detected in the 1-year follow radiographs. We believe that endoscopic total excision of giant synovial cyst is a valid surgical option that does not lead to segmental instability and subsequent fusion and instrumentation.
This case report demonstrates the successful full endoscopic excision of a giant synovial cyst at the lumbar spine without requiring additional fusion or instrumentation. Post-operative outcomes were favorable, with resolution of radicular pain, no recurrence of the cyst at 1-year follow-up and no instability. Therefore, endoscopic excision represents a valid and less invasive alternative to traditional open surgery, potentially avoiding the need for fusion and instrumentation in appropriately selected cases.
Endoscopic total excision of giant synovial cysts of the lumbar spine is a safe and effective surgical option that can effectively address symptoms while minimizing the risk of segmental instability. This minimally invasive approach offers a promising alternative to traditional open surgery for patients with this condition.
References
- 1.Janssen SJ, Ogink PT, Schwab JH. The prevalence of incidental and symptomatic lumbar synovial facet cysts. Clin Spine Surg 2018;31:E296-301. [Google Scholar | PubMed]
- 2.Khan AM, Girardi F. Spinal lumbar synovial cysts. Diagnosis and management challenge. Eur Spine J 2006;15:1176-82. [Google Scholar | PubMed]
- 3.Bruijn JD, Koning J. Compression of the ulnar nerve by an aneurysm. A case of late complication after a supracondylar fracture. Acta Orthop Scand 1992;63:223-4. [Google Scholar | PubMed]
- 4.Lyons MK, Atkinson JL, Wharen RE, Deen HG, Zimmerman RS, Lemens SM. Surgical evaluation and management of lumbar synovial cysts: The Mayo Clinic experience. J Neurosurg 2000;93:53-7. [Google Scholar | PubMed]
- 5.Velagapudi L, Matias CM, Elia C, Stolzenberg D, Largoza G, Feld R, et al. Spinal ganglion cyst presenting with radiculopathy: Diagnostic challenges and differential. Spinal Cord Ser Cases 2021;7:6. [Google Scholar | PubMed]
- 6.Czervionke LF. Synovial cyst. In: Czervionke LF, Fenton DS, editors. Imaging Painful Spine Disorders. Ch. 75. Philadelphia, PA: W. B. Saunders; 2011. p. 574-81. [Google Scholar | PubMed]
- 7.Boviatsis EJ, Stavrinou LC, Kouyialis AT, Gavra MM, Stavrinou PC, Themistokleous M, et al. Spinal synovial cysts: Pathogenesis, diagnosis and surgical treatment in a series of seven cases and literature review. Eur Spine J 2008;17:831-7. [Google Scholar | PubMed]
- 8.Oertel JM, Burkhardt BW. Endoscopic surgical treatment of lumbar synovial cyst: Detailed account of surgical technique and report of 11 consecutive patients. World Neurosurg 2017;103:122-32. [Google Scholar | PubMed]
- 9.Wu HH, Chu L, Zhu Y, Cheng CY, Chen CM. Percutaneous endoscopic lumbar surgery via the transfacet approach for lumbar synovial cyst. World Neurosurg 2018;116:35-9. [Google Scholar | PubMed]
- 10.Hellinger S, Lewandrowski KU. Clinical outcomes with endoscopic resection of lumbar extradural cysts. J Spine Surg 2020;6:S133-44. [Google Scholar | PubMed]
- 11.Wu HH, Wang GC, Sun LW, Chang KS, Yang JS, Chu L, et al. Symptomatic lumbar juxtafacet cyst treated by full endoscopic surgery. World Neurosurg 2019;130:e598-604. [Google Scholar | PubMed]
- 12.Komp M, Hahn P, Ozdemir S, Merk H, Kasch R, Godolias G, et al. Operation of lumbar zygoapophyseal joint cysts using a full-endoscopic interlaminar and transforaminal approach: Prospective 2-year results of 74 patients. Surg Innov 2014;21:605-14. [Google Scholar | PubMed]
- 13.Vergara P, Akhunbay-Fudge CY, Kotter MR, Charles Laing RJ. Minimally invasive versus open surgery for lumbar synovial cysts. World Neurosurg 2017;108:555-9. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Navigation-Assisted Endoscopic Excision of Lumbar Vertebral Osteoid Osteoma: A Case Report
May 1, 2026 Navigation-Assisted Endoscopic Excision of Lumbar Vertebral Osteoid Osteoma: A Case Report October 1, 2025 Glomus Tumour of Sciatic Nerve – A Rare Presentation Mimicking Sciatica
October 1, 2025 Glomus Tumour of Sciatic Nerve – A Rare Presentation Mimicking Sciatica August 1, 2026 A Case Report – K Wire as Guide in Endoscopic Plantar Fascia Release for Beginners
August 1, 2026 A Case Report – K Wire as Guide in Endoscopic Plantar Fascia Release for Beginners June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center
June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center