
Extra skeletal chondromas can have unusual behavior and generate problems associated with size and mechanical compression.
Dr. Daniel Felipe Kafury, School of Medicine, Universidad Icesi, Cl.18 #122-135, Santiago de Cali, 760032, Colombia. E-mail: danielkafury123@gmail.com
Abstract
Introduction: Extra skeletal chondromas are a subtype of chondroma that constitutes approximately 1.5% of soft tissue tumors; they do not affect the periosteum, cortex, or synovial tissue. They are frequently found in hands and are generally smaller than 3 cm in diameter; few cases are reported larger than 10 cm in diameter.
Case Report: A 59-year-old female patient with a history of tumor of 12 cm in diameter in the interdigital region between the first and second of the left hand of 9 years of evolution with involvement of the thumb opposition, with magnetic resonance imaging findings with isointensity in T1 and hyperintensity in T2, without enhancement to gadolinium, She is taken to an excisional biopsy where there is evidence of adherence to the sensory branch of the median nerve, with report of extra skeletal chondroma pathology, with follow-up 1 year post-surgery with total recovery of functionality without evidence of recurrence, additionally tumor with clinical and imaging suggestive of enchondroma in the fifth finger of the left hand and in the frontal region.
Conclusions: We present an unusual clinical case of extra skeletal chondroma of 12 cm in diameter with compromised mobility of the first finger and adherence to the sensory branch of the median nerve, accompanied by suggestive enchondromas in the fifth finger of the same hand and frontal region, without pathological findings of Ollier’s disease, malignancy, or recurrence at 1 year of follow-up. We intend to highlight the importance and magnitude, to which extraskeletal chondromas can reach, without being considered benign tumors, they can have important effects due to their mechanical compression.
Keywords: Extraskeletal chondroma, soft tissue, chondromas, soft tissue chondroma.
Chondroma is a benign tumor originating from hyaline cartilage, it has four variations if it originates from the intramedullary portion of the bone, it is called enchondroma, if it originates from the periosteum it is called periosteal chondroma, multiple enchondromatosis is called Ollier’s disease, finally, if it originates from the connective tissue without affecting bone cortex, synovial tissue or periosteum it is called extra skeletal chondroma [1,2]. Extraskeletal chondroma makes up approximately 1.5% of soft tissue neoplasms, it is characterized by being a slow-growing tumor that can be associated with pain and/or sensitivity with a predilection to the male gender, in general, they have an excellent prognosis and malignant transformation is sporadic [3]. They are characterized by being smaller than 3 cm in diameter and are most frequently located in the periarticular region of the hands or feet [4]. The hypothesis of the predilection for hands is described as the high amount of trauma, micro traumas, and injuries to which they are exposed, genetic mutations in the IDH1 or IDH2 genes, or even the lower temperature to which they are exposed as they are part of the appendicular skeleton [1,5,6]. The treatment with evidence of better results is surgical excision, radical surgeries are not required, and the local recurrence rate is 10–18% of the cases [7]. We present a case of interest of a patient with an extra skeletal chondroma in the hand of 12 cm in diameter with compression of the sensory branch of the median nerve, of 9 years of evolution, additionally with enchondroma in the fifth finger of the same hand and in the frontal region, without evidence of malignancy or Ollier’s disease, the case report is made with 1-year follow-up and is accompanied by a critical review of the literature.
A 59-year-old female patient with no relevant history presenting a mass between the first and second finger of the left hand of approximately 9 years of evolution with slow and progressive growth, at the beginning asymptomatic but at the time of consultation with the imposition by the opposition of the first finger and feeling of tension in the affected area. Denies symptoms suggestive of peripheral nerve disorders or pain. Furthermore, reports a slowly growing mass on the fifth finger of the left hand without limitation of the mobility of the phalanx, without pain or associated inflammatory signs. On physical examination, a tumor of 12 cm in diameter with involvement of the tenar region and the dorsal region of the hand was evidenced in the left hand in the interdigital crease between the first and second fingers (Fig. 1). On palpation the mass was soft, immobile, and non-painful without local inflammatory signs; initial biochemistry was taken with no blood chemistry alterations.

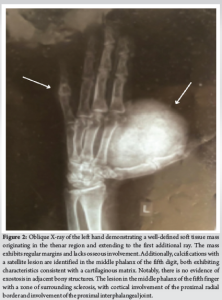
An X-ray of the hand showed a radiopaque mass of 5.0 × 4.5 cm with slight internal calcification on the palmar side of the fifth proximal phalanx, without changes in the bony cortices, additionally lytic image in the proximal third of the middle phalanx of the fifth finger with sclerotic borders, polylobulated pattern, without periosteal or soft tissue reaction (Fig. 2).
Due to the non-specific changes, it was decided to take a nuclear magnetic resonance, where an isointense image in T1 (W1) was evidenced between the first and second finger, with hyperintense signals in T2 (W1) without enhancement after gadolinium.
Given the findings it was considered to carry out an excisional biopsy surgical procedure, the procedure was performed under general anesthesia, the skin was incised and dissected by planes, the median and ulnar digital nerves, arteries, and veins were identified and protected. Then, it was identified that the tumor was markedly adhered to the A1 pulley and sensitive branch of the median nerve, no contact between the tumor and the bone was identified (Fig. 3) so proceeded to remove the tumor, resect redundant skin, and close by planes without complications.

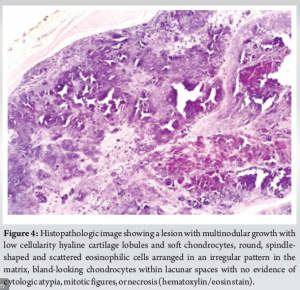
Samples were sent to pathology with a pathological diagnosis of extra skeletal chondroma (Fig. 4), 1 year of follow-up after surgery without evidence of recurrence of the tumor, with complete improvement of mobility in the first and second fingers.
The chondroma is a benign hyaline cartilaginous tumor, Henderson et al. described that despite benign and of slow growth it can trigger pathological fractures, nerve compressions, or even in a low proportion can have malignant transformation or develop Ollier’s disease [8]. These tumors constitute a minor portion of the incidence of soft tissue tumors and most of them are enchondromas, so extra skeletal chondromas are rare and little described, Bovee et al. describe that most of them are <3 cm. Cardia et al. define it as a soft tissue chondroma with no connection to the cortex, bone marrow, periosteum, or synovial tissue [9]. In an epidemiological review, Dahlin and Salvador found a slight preference for the male gender [3], although other authors such as Nazarova et al. have found no differences between genders [1]. Similarly, Nazarova et al. in a study of characterization of extra skeletal chondroma with a sample of 73 patients found that 40% were found in the hands and/or fingers, 19% in the head, and 16.4% in the feet [1]. Histopathologically, Chung and Enzinger, describe that extra skeletal chondroma is a benign proliferation of chondrocytes in a hyaline cartilage matrix arranged in lobules associated with fibrosis, ossification and myxoid areas, in immunohistochemistry positive staining is described for S-100 protein, vimentin and is characterized by low Ki 67 positivity (<3%) [10]. It is important to differentiate between extra skeletal chondroma and chondrosarcoma using features such as cellular atypism and the level of cord-like cellular arrangement. However, some chondromas have a cellular density and binucleated cells like those of chondrosarcomas, making differentiation difficult. The first-line treatment of extra skeletal chondroma is surgical excision; Nouh et al. describe a recurrence rate after this management of 10–18% [7]. In the present case report, an extra skeletal chondroma of unusual growth >10 cm is presented, with an unusual complication such as the compression of a sensitive branch, it is taken to surgical resection with the finding of severe adhesion with the A1 pulley, subsequently, the clinical follow-up is performed at 1 year of evolution with an improvement of the functionality of the affected hand and without evidence of recurrences. The case is considered of relevance because the clinical presentation is unusual, it is proposed to study genetic factors that may predispose the abnormal growth of extraskeletal chondromas, to study the long-term recurrence rates in these chondromas with abnormal growth, the rates of complications and associated nerve compressions.
The extraskeletal chondroma is a subtype of chondroma with low incidence and little described in the literature, characterized by its size <3 cm and low recurrence rates. However, the present case report presents an extra skeletal chondroma >10 cm with compression to a sensitive branch and severe adhesion to the A1 pulley, it is considered necessary to perform genetic and immunohistological extension studies to determine if there are differences that explain the unusual growth, similarly, long-term follow-up is proposed to evaluate associated recurrence rates.
It is proposed that atypical presentations of extra skeletal chondroma be subjected to additional genetic and immunohistochemical studies to define additional characteristics, and it is also proposed to perform strict follow-up.
References
- 1.Nazarova NZ, Umarova GS, Vaiman M, Abba M, Foonberg M, Mametov K, et al. The distribution of chondromas: Why the hand? Med Hypotheses 2020;143:110132. [Google Scholar | PubMed]
- 2.Bahnassy M, Abdul-Khalik H. Soft tissue chondroma: A case report and literature review. Oman Med J 2009;24:296-9. [Google Scholar | PubMed]
- 3.Dahlin DC, Salvador AH. Cartilaginous tumors of the soft tissues of the hands and feet. Mayo Clin Proc 1974;49:721-6. [Google Scholar | PubMed]
- 4.Bovee JV, Hogendoorn PC. Cartilage-forming tumours of bone and soft tissue and their differential diagnosis. Curr Diagn Pathol 2001;7:223-34. [Google Scholar | PubMed]
- 5.Roessner A, Smolle M, Schoeder V, Haybaeck J. Cartilage tumors: Morphology, genetics, and current aspects of target therapy. Pathologe 2020;41:143-52. [Google Scholar | PubMed]
- 6.Saiji E, Pause FG, Lascombes P, Cerato Biderbost C, Marq NL, Berczy M, et al. IDH1 immunohistochemistry reactivity and mosaic IDH1 or IDH2 somatic mutations in pediatric sporadic enchondroma and enchondromatosis. Virchows Arch 2019;475:625-36. [Google Scholar | PubMed]
- 7.Nouh MR, Amr HA, Ali RH. Imaging of rare appendicular non-acral soft-tissue chondromas in adults with histopathologic correlation. Acta Radiol 2018;59:700-8. [Google Scholar | PubMed]
- 8.Henderson M, Neumeister MW, Bueno RA Jr. Hand tumors: II. Benign and malignant bone tumors of the hand. Plast Reconstr Surg 2014;133:814e-21e. [Google Scholar | PubMed]
- 9.Cardia R, Favazzi CM, Fenga D, Rosa MA, Ieni A. A large extraskeletal chondroma: An unusual location in the lower extremity, huge extraskeletal chondroma: An unusual localization in the leg. J Orthop Case Rep 2019;9:74-7. [Google Scholar | PubMed]
- 10.Chung EB, Enzinger FM. Chondroma of soft parts. Cancer 1978;41:1414-24. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2024 Soft-tissue Chondroma Masquerading as Chondroid Syringoma – A Case Report
September 1, 2024 Soft-tissue Chondroma Masquerading as Chondroid Syringoma – A Case Report April 1, 2025 Extra-Axial Soft Tissue Chordoma of Hand: A Rare Case Report
April 1, 2025 Extra-Axial Soft Tissue Chordoma of Hand: A Rare Case Report January 28, 2015 Plagiarism- Cut it at the roots
January 28, 2015 Plagiarism- Cut it at the roots November 1, 2025 Incidence and Functional Impact of Malrotation after Intramedullary Nailing of Femoral Shaft Fractures: A Prospective Computed Tomography-based Observational Study
November 1, 2025 Incidence and Functional Impact of Malrotation after Intramedullary Nailing of Femoral Shaft Fractures: A Prospective Computed Tomography-based Observational Study