
An irreducible shoulder dislocation may not always require open surgery; it can also be done under arthroscopy.
Dr. Hari Krishna Yadoji, Department of Orthopedics, Citizens Specialty Hospital, Nallagandla, Hyderabad, Telangana, India. E-mail: drharikrishna20@gmail.com
Abstract
Introduction: The shoulder is the most mobile joint and also the most commonly dislocated joint in our body. Anterior dislocation of the shoulder is more common than posterior and inferior dislocation. Anterior dislocation of the shoulder can be easily reduced by the Stimson technique, traction-counter traction technique, etc. Reducing an acute anteriorly dislocated shoulder is usually easy, but in some instances, it can be difficult due to the interposition of the long head of the biceps, subscapularis, or impacted Hill-Sach. This is a case report of a patient with 10 days old irreducible anterior dislocation of the shoulder. Magnetic resonance imaging (MRI) shows the anterior capsule trapped between the humeral head and glenoid, which does not allow the shoulder to be relocated. This case report highlights the possibility of anterior capsule entrapment in the glenohumeral joint with the subscapularis being intact and that it can be managed by arthroscopy, which has fewer complications than open surgery.
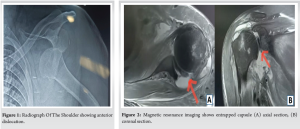
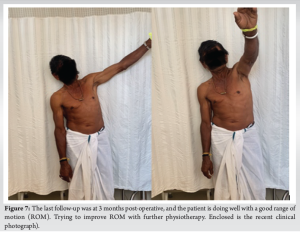
Case Report: A 55-year-old male came with irreducible anterior dislocation of his left shoulder after a slip and fall on his outstretched hand. There was a history of attempts to reduce the dislocation in another hospital but failed to reduce it even under sedation. An MRI of the left shoulder shows that the anterior capsule got entangled between the humeral head and glenoid, as shown in Fig. 1 and 2, and is not allowing the humerus head to reduce. There are reports of the irreducible anterior dislocated shoulder due to interposition of the subscapularis muscle, long head of biceps, greater tuberosity fracture fragment, etc., and are managed by open surgery. In our case report, we managed to disengage the entrapped anterior capsule by arthroscopy after a trial of closed reduction under general anesthesia.
Conclusion: Irreducible shoulder dislocation is not a common problem. There are many pathologies that result in the irreducibility of shoulder dislocation; anterior capsule entrapment is one such pathology. Open surgery is not the only solution to address these pathologies; we can treat them by arthroscopy technique, which can address all associated pathologies with minimal complications, unlike open surgery.
Keywords: Irreducible shoulder dislocation, arthroscopy, entrapped capsule in shoulder.
The shoulder is the most mobile joint and also the most commonly dislocated joint in our body [1]. The greater mobility of the shoulder comes at the price of being most vulnerable to dislocation [2]. Anterior dislocation of the shoulder is more common than posterior and inferior dislocation [2]. Reducing an acute anteriorly dislocated shoulder is usually easy, but in some instances, it can be difficult due to the interposition of the subscapularis muscle or tendon [3,4], the tendon of the long head of the biceps [5,6], the glenoid labrum [6], a loose bony fragment from the glenoid [7], and the greater tuberosity fracture fragment [8].
A 55-year-old male came with irreducible anterior dislocation of the left shoulder after a slip and fall on his outstretched hand. There was a history of attempts to reduce the dislocation in another hospital but failed to reduce it even under sedation. The X-ray shows a dislocated shoulder as in Fig. 1. Magnetic resonance imaging (MRI) of the left shoulder (based on literature, we anticipated a soft tissue entrapment could be the reason for irreducibility, so we ordered an MRI, which is more informative than 3D computed tomography scan) shows anterior capsule got entangled between the humeral head and glenoid as in Fig. 2a and b, and is not allowing the humerus head to reduce. There are reports of the irreducible anterior dislocated shoulder due to interposition of the subscapularis muscle, long head of biceps, greater tuberosity fracture fragment, etc., and are managed by open surgery. In our case report, we managed to disengage the entrapped anterior capsule by arthroscopy after a trial of closed reduction under general anesthesia.
Surgical technique
Under general anesthesia, an attempt at closed reduction was done, but we were unable to reduce the dislocation. We planned for arthroscopy, and the patient was positioned in the right decubitus position. Using a standard posterior portal (2 cm inferior and 1 cm medial to posterolateral corner of acromion), diagnostic arthroscopy was done. A large capsule was found entrapped between the glenoid and humerus head, as shown by an arrow in Fig. 3. As the capsule was obstructing the view, we were unable to make an anteroinferior (rotator interval) portal, so we made an anterosuperior portal. With the posterior portal as a viewing portal, tried to reduce the capsule with a Wisinger rod from the anterosuperior portal, but the attempt was in vain. We shifted the viewing portal to the anterosuperior portal and tried to reduce the capsule with a Wisinger rod from the posterior portal, as in Fig. 4. With some difficulty, and we were able to reduce it. We established the anteroinferior/interval portal and once again performed the diagnostic arthroscopy. We found the subscapularis tendon to be normal, the anterior capsule, along with the middle glenohumeral ligament, was torn from the humeral side, and the patient had a supraspinatus complete tear. The anterior labrum was normal, and there was a small, shallow Hill-Sach. With the given findings on arthroscopy, we planned to perform anterior capsule repair and supraspinatus repair arthroscopically. The anterior capsule was repaired with an all-suture anchor of 1.8 mm, as in Fig. 5, and the supraspinatus was repaired to greater tuberosity with two anchors in a single row. Post-operative X-ray shows reduced shoulder dislocation, as in Fig. 6. After surgery, the patient was immobilized with a shoulder immobilizer. The patient is under supervised physiotherapy protocol. (The last follow-up was at 3 months post-operative; the patient is doing well with a good range of motion [ROM]. Trying to improve ROM with further physiotherapy. We are enclosing the recent clinical photograph) (Fig. 7).


Shoulder dislocation is the most commonly dislocated joint in our body [9], with the incidence of 1st-time anterior dislocation ranging from 8 to 8.2/100,000 population/year, and the prevalence is about 2% [10]. An acutely dislocated shoulder is usually easily reduced by closed reduction techniques [11]. Irreducibility of the acutely dislocated shoulder is rare [9]. The reported causes of an irreducible shoulder dislocation include interposition of the subscapularis muscle or tendon [3,4], the tendon of the long head of the biceps [5,6], a loose bony fragment from the glenoid [7], and the greater tuberosity fracture fragment [8]. Anterior shoulder dislocations are sometimes associated with rotator cuff tears, especially in older patients. The incidence of rotator cuff tear in patients older than 40 years is up to 30%, and among those older than 60 years, is up to 80% [12]. Whenever you find it difficult to reduce an anterior shoulder dislocation, advise an MRI of the shoulder as it can help you diagnose both bony and soft-tissue pathologies with a single investigation and guide us in planning further management. There are case reports on different pathologies behind the irreducibility of an anterior dislocated shoulder such as the interposition of subscapularis muscle or tendon, the tendon of the long head of the biceps, the glenoid labrum, and the greater tuberosity fracture fragment, which are managed by open surgery. This case report highlights the possibility of anterior capsule entrapment in the glenohumeral joint with the subscapularis being intact and that it can be managed by arthroscopy, which has fewer complications than open surgery. In open surgery, if we use the anterior deltopectoral approach, subscapularis/long head of biceps pathology can be addressed, but supraspinatus/infraspinatus pathologies cannot be addressed easily. If we use the deltoid split approach, pathologies of greater tuberosity or supraspinatus/infraspinatus can be addressed, but pathologies of subscapularis/long head of biceps cannot be addressed easily. To address additional pathologies during open surgery, we may require additional incisions, which can lead to complications such as poor healing of skin sutures and stiffness. The advantage of arthroscopy is that associated pathologies can also be treated easily with minimal complications.
Irreducible shoulder dislocation is not a common problem. There are many pathologies that result in the irreducibility of shoulder dislocation; anterior capsule entrapment is one such pathology. Open surgery is not the only option to address these pathologies; we can treat them by arthroscopy technique which can address all associated pathologies with minimal complications, unlike open surgery.
Irreducible anterior dislocation is not a common problem we see in our practice but it needs early detection and treatment to avoid complications. Identification of obstacles resisting closed relocation is important and MRI and arthroscopy can help to identify it. Arthroscopic treatment is both safe and other associated pathologies can be treated at the same time.
References
- 1.Ilahi OA. Irreducible anterior shoulder dislocation with fracture of the greater tuberosity. Am J Orthop (Belle Mead NJ) 1998;27:576-8. [Google Scholar | PubMed]
- 2.Wen DY. Current concepts in the treatment of anterior shoulder dislocations. Am J Emerg Med 1999;17:401-7. [Google Scholar | PubMed]
- 3.Kuhnen W, Groves RJ. Irreducible acute anterior dislocation of the shoulder: Case report. Clin Orthop Relat Res 1979;139:167-8. [Google Scholar | PubMed]
- 4.Lam SJ. Irreducible anterior dislocation of the shoulder. J Bone Joint Surg Br 1966;48:132-3. [Google Scholar | PubMed]
- 5.Inao S, Hirayama T, Takemitsu Y. Irreducible acute anterior dislocation of the shoulder: Interposed bicipital tendon. J Bone Joint Surg Br 1990;72:1079-80. [Google Scholar | PubMed]
- 6.Seradge H, Orme G. Acute irreducible anterior dislocation of the shoulder. J Trauma 1982;22:330-2. [Google Scholar | PubMed]
- 7.Mihata T, Doi M, Abe M. Irreducible acute anterior dislocation of the shoulder caused by interposed fragment of the anterior glenoid rim. J Orthop Sci 2000;5:404-6. [Google Scholar | PubMed]
- 8.Oni OO. Irreducible acute anterior dislocation of the shoulder due to a loose fragment from an associated fracture of the greater tuberosity. Injury 1983;15:138. [Google Scholar | PubMed]
- 9.Gudena R, Iyengar KP, Nadkarni JB, Loh W. Irreducible shoulder dislocation-a word of caution. Orthop Traumatol Surg Res 2011;97:451-3. [Google Scholar | PubMed]
- 10.Khiami F, Gérometta A, Loriaut P. Management of recent first-time anterior shoulder dislocations. Orthop Traumatol Surg Res 2015;101:S51-7. [Google Scholar | PubMed]
- 11.Day MS, Epstein DM, Young BH, Jazrawi LM. Irreducible anterior and posterior dislocation of the shoulder due to incarceration of the biceps tendon. Int J Shoulder Surg 2010;4:83-5. [Google Scholar | PubMed]
- 12.Bayoumy MA, Said HG, Abdelkawi AF, Fetih TN. Treatment of irreducible traumatic anterior shoulder dislocation caused by subscapularis tendon interposition. Arthrosc Tech 2017;6:e737-41. [Google Scholar | PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study June 1, 2026 Standardized Preparation and Multi-Site Application of Leukocyte-Poor Platelet-Rich Plasma in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Technical Note with Early Functional Outcomes
June 1, 2026 Standardized Preparation and Multi-Site Application of Leukocyte-Poor Platelet-Rich Plasma in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Technical Note with Early Functional Outcomes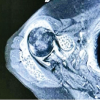 June 1, 2026 Secondary Synovial Chondromatosis of the Shoulder Associated with Rotator Cuff Tear: Diagnostic Challenge and Arthroscopic Management – A Case Report
June 1, 2026 Secondary Synovial Chondromatosis of the Shoulder Associated with Rotator Cuff Tear: Diagnostic Challenge and Arthroscopic Management – A Case Report May 1, 2026 Simultaneous Anterior Cruciate Ligament Avulsion Fracture with Bilateral Posterior Meniscal Root Tears of the Knee: A Case Report
May 1, 2026 Simultaneous Anterior Cruciate Ligament Avulsion Fracture with Bilateral Posterior Meniscal Root Tears of the Knee: A Case Report