
• To evaluate the effectiveness of TENS in treating midshaft clavicle fracture • To assess the functional outcome using Constant-Murley score • To assess the complications associated with TENS
Dr. Pradeep E, Professor, Department of Orthopaedics and Traumatology, Chettinad Hospital and Research Institute, Kelambakkam, Tamil Nadu, India. Email ID – dr_prad87@yahoo.co.in.
Abstract
Introduction: Clavicle fractures are a common traumatic injury, often treated conservatively. However, displaced midshaft fractures present risks of complications such as delayed union and malunion. Surgical intervention, including open reduction and internal fixation and titanium elastic nailing system (TENS), offers better outcomes for these fractures. This study evaluates the effectiveness of TENS in treating midshaft clavicle fractures. Functional recovery was assessed using the Constant-Murley score, while radiological outcomes tracked fracture union.
Aim and Objective: The study aimed to evaluate the effectiveness of TENS in treating midshaft clavicle fractures, assess functional recovery using the Constant-Murley score, and analyze associated complications.
Materials and Methods: A descriptive cross-sectional study was conducted on 35 patients aged 16–60 with middle-third clavicle fractures, treated with TENS at Chettinad Hospital between August 2022 and April 2024. Functional outcomes were assessed using the Constant-Murley score, and radiographs were taken to evaluate fracture union.
Results: Results showed favorable outcomes with TENS, including a mean union time of 4.55 months and a mean Constant score of 81.7 after 6 months. Complications were minimal, including infection, intraoperative blood loss, and hardware irritation. TENS demonstrated its value as a minimally invasive, effective option for displaced midshaft clavicle fractures, providing both cosmetic and early functional benefits.
Conclusion: The study demonstrated that TENS is a safe and effective treatment for displaced midshaft clavicle fractures, offering faster recovery, improved functional outcomes, fewer complications, and better cosmetic results, fulfilling its objective of assessing TENS effectiveness.
Keywords: Clavicle fracture, midshaft clavicle fracture, titanium elastic nailing system, functional outcomes, minimally invasive surgery.
The clavicle serves as a vital link between the thorax and shoulder girdle, aiding in shoulder movement. Due to its superficial location, clavicle fractures are a frequent traumatic injury, often resulting from both low- and high-energy impacts. These fractures represent 5–10% of all fractures and nearly 44% of shoulder-related injuries [1,2]. The middle third of the clavicle, due to its structural vulnerability, is the most common site for fractures, accounting for 80% of cases, with over half of these fractures being displaced [3]. Historically, clavicle fractures were primarily managed nonoperatively using methods such as slings or figure-of-eight bandages. Early studies reported non-union rates below 1% with conservative care [4,5]. However, these findings were often based on non-standardized studies, which included patients of different ages and fracture types, as well as pediatric cases where natural healing and remodeling abilities are stronger [6,7]. More recent research has shown that non-union rates can be as high as 15%, with some patients experiencing poor functional outcomes even when fractures heal. In addition, malunion has been identified as a distinct complication, contributing to unsatisfactory results. These findings suggest that displaced midshaft clavicle fractures should not always be managed conservatively, as the outcomes can vary significantly. In recent years, surgical intervention has gained popularity as a more reliable option, particularly for displaced fractures as surgical intervention has less non-union and malunion rates. Surgical options include open reduction and internal fixation (ORIF) using plates and screws, and intramedullary fixation with devices like the Titanium elastic nailing system (TENS). While ORIF with plating is considered the gold standard, it is associated with complications such as large incisions, extensive soft-tissue damage, increased blood loss, and potential nerve or vessel injury. Additional concerns include infection, cosmetic scarring, and stress shielding after plate removal, which may result in refracture [8,9]. In contrast, TENS, first introduced in 2002, offers several advantages, including smaller incisions, less soft-tissue disruption, and load-sharing fixation, which allows micromotion at the fracture site, promoting callus formation. Despite some risks, such as hardware irritation or implant migration [10], TENS has demonstrated good clinical and functional outcomes. The study focuses on addressing the challenges of managing displaced midshaft clavicle fractures. Conservative treatments often result in complications such as non-union or malunion, while plating procedures involve significant tissue disruption and visible scarring. TENS presents a less invasive alternative, aiming to enhance recovery, minimize complications, and provide better cosmetic results. By assessing functional recovery through the Constant-Murley score, along with radiological outcomes and associated complications, this research seeks to determine the effectiveness of TENS as a superior treatment method for such fractures.
In this descriptive study, participants who had displaced middle third clavicle fractures treated with TENS at Chettinad Hospital and Research Institute from August 2022 to April 2024 were approached. From which 35 patient aged between 16–60 years with a follow-up period of minimum of 6 months were included in the study. Two different surgeons performed all the surgeries.
Inclusion criteria
- Fracture middle third of clavicle
- Age >16 <60
- Tenting/compromised skin
- Polytrauma with ipsilateral rib fracture
- ROBINSON type 2A1, 2A2, 2B1, and 2B2 (TYPE 2 – Middle clavicle: A – cortical alignment A1 – non-displaced A2 – angulated B-displaced fracture 13 B1– consists of simple or single butterfly fragment B2 – is a comminuted or segmental fracture) [11].
Exclusion criteria
- Patients with pre-existent morbidity concerning arm, shoulder, or hand
- Moderate to severe head injury
- Bilateral clavicle fractures
- Fractures with associated neurovascular injury
- Pathological fracture
- Fracture >3 weeks
- ROBINSON type 1 and 3 (medial and distal third clavicle fractures).
Surgical technique
General anesthesia or a regional block is administered. The patient is positioned supine with a sandbag placed in the inter-scapular region for support. A skin incision measuring 1–2 cm is made approximately 1.5 cm lateral to the sternoclavicular joint. Using a 2.5 mm drill bit, a hole is created in the anterior cortex of the clavicle, which is then widened with a small bone awl (Fig. 1). A titanium elastic nail, sized between 2 and 2.5 mm in diameter (depending on the patient’s medullary diameter), is then secured in a universal chuck with a T-handle. The nail is advanced toward the fracture site using oscillating motions (Fig. 1). If closed reduction is unsuccessful, an additional small incision of 2–3 cm is made directly over the fracture site to manipulate the fragments. The nail is then advanced into the lateral fragment of the clavicle. After achieving the desired placement, the nail is cut off at the entry point, leaving about 1 cm for potential future removal (Fig. 1). The skin is then sutured closed without the need for a drain.

Post-operative care
Patients were protected by a standard sling for comfort after surgery, and pendulum exercises were permitted in the initial post-operative period. Patients were allowed as much unrestricted shoulder movement as feasible during the post-operative period. Sutures were removed on the 12th post-operative day. Overhead activity was restricted for 3 weeks. When radiological union was detected, strengthening workouts were initiated.
Assessment
Under the guidance of an orthopedician, anteroposterior shoulder views were taken to make sure that the patient was in standard position-rays which were taken immediately postoperatively and at 6 weeks, 3 months, and 6 months postoperatively. During these follow-ups, a clinical evaluation was conducted to assess pain levels, shoulder joint range of motion, and muscle strength. Radiological assessments were performed by obtaining serial X-rays to evaluate fracture union. Union was considered successful when bridging trabeculations were visible across three of the four cortices at the fracture site. In addition, any alterations in alignment or signs of implant migration or failure were documented. The Constant-Murley score evaluates shoulder strength, range of motion, and pain during routine activities. Excellent (100–86 points), good (85–71 points), satisfactory (70–56 points), and poor (below 56 points) are the four categories for the Constant score [12]. TENS removal was performed after 1 year once radiological signs of union were observed, and the patient had achieved functional improvement. A record of complications was documented during each follow-up period (Fig. 2). TENS removal done after 1 year once patient had radiological sign of union and functionally improved.

Total of 35 patients were evaluated in this study, as summarized in Table 1. In our study, maximum of the study participants was in the age group of 20–30 years (39%). The mean age of the study participants was observed to be 37.1 ± 11.5 years with an age range of 19–56 years. Majority of the study participants were male (78%), while 22% of them were female. Maximum of the study participants suffered injury by road traffic accidents (RTA) (92.7%), while 7.3% of them suffered injury by accidental fall and 65% of the study participants had injury on the right side followed by left (34.1%). According to Robinson classification, 53.7% of the study participants were classified as 2B1 and 46% were classified as 2B2. Mean hospital stay was 7.2 days. The mean time of union was 4.55 months (18 weeks) ranging from 2 to 6 months (4–24 weeks). One among 35 patients had delayed union and one out of total of 35 patients had malunion. Pre-operative mean constant score was 9.8. Six weeks post-operative mean constant score was 66.1. Three months post-operative mean constant score was 78.8. Six months post-operative mean constant score was 81.7. Complications were seen in eight patients. Two patients had post-operative infection, two had implant breakage, three had hardware irritation, one had delayed union, and one had malunion.
Clavicle fractures are commonly treated non-surgically. In a 1997 study by Hill et al. involving 242 patients with clavicle fractures, 27% had fractures in the middle third of the clavicle. These patients were treated conservatively and followed for an average of 38 months. Of these, 31% reported poor outcomes due to significant shortening or non-union [13]. Similarly, in a 1998 study by Nordqvist and Petersson, non-operative treatment of 71 midclavicular fractures resulted in almost 50% healing with at least 5 mm shortening and malunion [2]. Davis, in 2004, also reported poor outcomes following non-surgical treatment of displaced middle-third fractures. Specifically, Robinson Type 2B1 and 2B2 fractures are now considered indications for surgical intervention [4]. Patients who underwent early surgical fixation for clavicle fractures had better outcomes, including higher postoperative constant scores, faster pain relief, quicker return to activity, and higher satisfaction rates [14]. ORIF using plate osteosynthesis can present challenges such as larger incisions, greater soft-tissue disruption, increased blood loss, and longer surgery times. There is also a higher risk of infection, neurovascular injury, cosmetic scarring, and the potential for refracture due to stress shielding after plate removal. However, intramedullary implants, such as TENS, offer advantages such as smaller incisions, reduced tissue damage, and load-sharing fixation, which allow for micromotion and promote callus formation, making it a less invasive and more effective option for treating displaced midshaft clavicle fractures. Studies show that correcting significant clavicular shortening (over 20 mm) is critical for better functional outcomes. Intramedullary implants, due to their biomechanical compatibility and minimally invasive nature, provide improved healing by allowing for better adaptation to clavicular tension and enhancing callus formation [15]. In this study, clavicle fractures were more common in males (78%) compared to females (22%), consistent with the findings of Jan et al., Mohammed et al., and Dhoju et al. [16,17,18]. Most participants were between 20 and 30 years old (39%), with a mean age of 37.1 years, which is similar to Elidrissi et al.’s and Javali et al.’s study where the mean age was 34 years and 38 year, respectively [19]. RTAs were the most frequent cause of fractures in this study, accounting for 92.7% of cases, while 7.3% resulted from accidental falls. These findings are in line with a study by Postacchini et al., where RTAs accounted for 47% of clavicle fractures, falls on outstretched hands for 33%, and rest of the 10% sports related injury, work related, and unknown, and similarly, in study by Shakeel and Sreenivasa, 80% patient had clavicle fracture due to RTA [20]. The average time to union in this study was 18 weeks, with one case of delayed union and one case of malunion. This compares with findings from Kadakia et al., where 38 patients treated with TENS had an average union time of 11.3 weeks, Fu where union occurred in 11.58 weeks and in Danish study, the mean time for radiological union 19.6 ± 6.67 week [21-23]. The functional outcome was measured using the Constant score, with an average score of 81.7 at 6 months postoperatively. In Kumar et al. study, mean constant score was 80.32, while in Fu study and Idris and Subash study, the mean Constant score was 93.3 and 93.3 ± 2.7, respectively [24,25]. In terms of complications, 5.71% of participants developed infections post-surgery, 5.71% experienced implant breakage, and 8.57% reported hardware irritation. One patient had delayed union, and another had malunion. Similarly, Altamimi et al.’s 2008 study found that hardware-related complications, such as local irritation, hardware prominence, wound infection, and implant failure, were common in the operative group [26]. In a study by Smekal et al., involving 60 patients treated with elastic intramedullary nailing, 10% had severe complications, including deep infections, non-union, implant failure, and post-removal fractures [27]. Minor complications included superficial infections, keloid scars, dysesthesia near the scar, and implant loosening leading to loss of reduction. Complications are an inherent aspect of any medical procedure, yet in our study, the occurrence of such adverse events was minimal. While complications cannot be entirely avoided, the frequency and severity of these events were sufficiently low to not significantly impact the overall outcomes or the interpretation of the study’s result.
The study concluded that the TENS is a highly effective, minimally invasive option for treating displaced midshaft clavicle fractures. It demonstrated significant improvements in functional recovery, as evidenced by increased Constant-Murley scores, and offered faster fracture union with fewer complications. TENS also provided better cosmetic outcomes, shorter recovery times, and early mobilization compared to traditional methods like plating. The findings highlight TENS as an excellent alternative for achieving both functional and esthetic benefits, making it a preferred treatment for displaced midshaft clavicle fractures. This aligns with the study’s objective of evaluating TENS effectiveness and complications.
Limitations
This study has a few limitations. Being a single-center study limits broader applicability, and the absence of a control group prevents direct comparisons with alternative treatments.
TENS is an effective, minimally invasive treatment for midshaft clavicle fractures, providing rapid recovery and improved functionality while minimizing complications compared to traditional surgical methods.
References
- 1.Bajuri MY, Maidin S, Rauf A, Baharuddin M, Harjeet SJ. Functional outcomes of conservatively treated clavicle fractures. Clinics (Sao Paulo) 2011;66:635-9. [Google Scholar | PubMed]
- 2.Nordqvist A, Petersson C. The incidence of fractures of the clavicle. Clin Orthop Relat Res 1994;300:127-32. [Google Scholar | PubMed]
- 3.Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg 2002;11:452-6. [Google Scholar | PubMed]
- 4.Davis RB. From aphorisms to APACHE: Medicine’s brave new world. Perspect Biol Med 1994;37:237-43. [Google Scholar | PubMed]
- 5.Neer CS 2nd. Nonunion of the clavicle. J Am Med Assoc 1960;172:1006-11. [Google Scholar | PubMed]
- 6.Nordqvist A, Redlund-Johnell I, von Scheele A, Petersson CJ. Shortening of clavicle after fracture: Incidence and clinical significance, a 5-year follow-up of 85 patients. Acta Orthop Scand 1997;68:349-51. [Google Scholar | PubMed]
- 7.Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD, Evidence-Based Orthopaedic Trauma Working Group. Treatment of acute midshaft clavicle fractures: Systematic review of 2144 fractures: On behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma 2005;19:504-7. [Google Scholar | PubMed]
- 8.McKee MD, Wild LM, Schemitsch EH. Midshaft malunions of the clavicle. J Bone Joint Surg Am 2003;85:790-7. [Google Scholar | PubMed]
- 9.Kulshrestha V. Primary plating of displaced mid-shaft clavicular fractures. Med J Armed Forces India 2008;64:208-11. [Google Scholar | PubMed]
- 10.Frigg A, Rillmann P, Perren T, Gerber M, Ryf C. Intramedullary nailing of clavicular midshaft fractures with the titanium elastic nail: Problems and complications. Am J Sports Med 2009;37:352-9. [Google Scholar | PubMed]
- 11.Robinson CM. Fractures of the clavicle in the adult: Epidemiology and classification. J Bone Joint Surg Br 1998;80:476-84. [Google Scholar | PubMed]
- 12.Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res 1987;214:160-4. [Google Scholar | PubMed]
- 13.Hill JM, McGuire MH, Crosby LA. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-8. [Google Scholar | PubMed]
- 14.McKee MD, Pedersen EM, Jones C, Stephen DJ, Kreder HJ, Schemitsch EH, et al. Deficits following nonoperative treatment of displaced midshaft clavicular fractures. 2006;88:35-40. [Google Scholar | PubMed]
- 15.Leppilahti J, Jalovaara P. Migration of Kirschner wires following fixation of the clavicle--a report of 2 cases. Acta Orthop Scand 1999;70:517-9. [Google Scholar | PubMed]
- 16.Dhoju D, Shrestha D, Parajuli NP, Shrestha R, Sharma V. Operative fixation of displaced middle third clavicle (Edinburg Type 2) fracture with superior reconstruction plate osteosynthesis. Kathmandu Univ Med J (KUMJ) 2011;9:286-90. [Google Scholar | PubMed]
- 17.Mohammed E, Mahadane H, Mechchat A, Shimi M, Elibrahimi A, Elmrini A. Functional outcome of midclavicular fracture fixation utilising a reconstruction plate. Malays Orthop J 2013;7:6. [Google Scholar | PubMed]
- 18.Jan I, Ganai AA, Shafiki M. Titanium elastic nail system (TENS) in displaced clavicle midshaft fractures. Nat J Clin Orthop 2023;7:1-4. [Google Scholar | PubMed]
- 19.Javali V, Praveen Kumar Reddy P. Titanium elastic intramedullary nailing for midclavicular fractures: Clinical outcomes. Indian J Orthop Surg 2017;3:73-7. [Google Scholar | PubMed]
- 20.Shakeel MA, Sreenivasa N. Surgical management of midshaft clavicle fracture by titanium elastic nailing system. Indian J Orthop Surg 2021;7:140-8. [Google Scholar | PubMed]
- 21.Kadakia AP, Rambani R, Qamar F, McCoy S, Koch L, Venkateswaran B. Titanium elastic stable intramedullary nailing of displaced midshaft clavicle fractures: A review of 38 cases. Int J Shoulder Surg 2012;6:82-5. [Google Scholar | PubMed]
- 22.Fu B. Minimally invasive intramedullary nailing of clavicular fractures by a new titanium elastic nail. Acta Orthop Traumatol Turc 2016;50:494-500. [Google Scholar | PubMed]
- 23.Danish M. Tens nailing in fracture clavicle-a case series. Trauma Int 2022;8:17-20. [Google Scholar | PubMed]
- 24.Kumar H, Banga RK, Boparai R, Singh J. Evaluation the outcomes of flexible intramedullary nailing fixation of displaced midshaft clavicle fractures. Indian J Orthop Surg 2017;3:197-201. [Google Scholar | PubMed]
- 25.Idris M, Subash Y. Is TENS a good treatment option in midshaft clavicle fractures? A Prospective study of 30 patients. Ann Roman Soc Cell Biol 2021;25:4149-55. [Google Scholar | PubMed]
- 26.Altamimi SA, McKee MD, Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures: Surgical technique. J Bone Joint Surg Am 2008;90:1-8. [Google Scholar | PubMed]
- 27.Smekal V, Irenberger A, El Attal R, Oberladstaetter J, Krappinger D, Kralinger FJ. Elastic stable intramedullary nailing is best for mid-shaft clavicular fractures without comminution: Results in 60 patients. Injury 2011;42:324-9. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report
July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report July 1, 2026 Early Mobilization with Mechanical Axis Preservation: A Prospective Outcome Analysis of Titanium Elastic Nailing in Femoral Shaft Fractures of School-Aged Children
July 1, 2026 Early Mobilization with Mechanical Axis Preservation: A Prospective Outcome Analysis of Titanium Elastic Nailing in Femoral Shaft Fractures of School-Aged Children July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes
July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes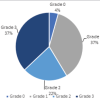 June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center
June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center