
The double endobutton technique is highly effective in managing acute type III and V AC joint dislocations, restorating the normal anatomy of the AC joint and yielding excellent functional outcomes for patients
Dr. Anubhav Sharma, Department of Orthopedics, Dayanand Medical College and Hospital, 2785/1 Gurdev Nagar, Ludhiana 141001, Punjab, India. E-mail: dranubhavsharma@gmail.com
Abstract
Introduction: Acromioclavicular (AC) joint injuries are frequently encountered in orthopedic practice and makeup about 12% of shoulder injuries. Endobutton technique has shown promising results for Rockwood type III AC injuries, but literature is still scarce from Indian Subcontinent. This study aimed to find functional outcomes in Rockwood type III and V AC joint dislocations managed with double endobutton technique.
Materials and Methods: The present retrospective study included thirteen patients with acute AC joint dislocation with duration of <7 days. In 10 cases (76.92%), the Rockwood grade was grade III, and in 3 (23.08%) cases, was grade V. All patients had significant instability and were operated using double endobutton technique. The functional outcomes of the patients were evaluated through Constant Murley score (CMS), simple shoulder test, American Shoulder and Elbow surgeons (ASES) score, AC joint instability (ACJI) score, and TAFT score, noted at baseline and at 1-year follow-up.
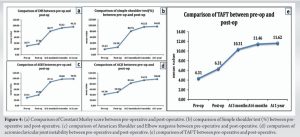
Results: Compared to pre-operative scores, at post-operative follow-up of 1 year, there were significant improvements in the CMS (96.31 ± 2.81 vs. 30.77 ± 4.28, P < 0.0001), simple shoulder test (96.81 ± 4.2 vs. 19.23 ± 7.9, P < 0.0001), ASES (98.92 ± 1.04 vs. 29.31 ± 3.25, P < 0.0001), ACJI (98.08 ± 2.53 vs. 41.38 ± 6.99, P < 0.0001), and TAFT score (11.62 ± 0.51 vs. 4.31 ± 0.95, P < 0.0001). There was no recurrence of instability, or any other complications noted at the end of 1 year.
Conclusion: The double endobutton technique proved effective in treating acute type III and V AC joint dislocations, yielding good functional outcomes.
Keywords: Acute acromioclavicular joint dislocation, coracoclavicular ligament, double endobutton, Rockwood classification, shoulder.
The acromioclavicular (AC) joint injuries are frequently encountered in orthopedic practice and makeup about 12% of shoulder injuries [1]. In spite of being common, there is no universally agreed upon approach to diagnosing and treating them, which makes them one of the most contentious shoulder injuries [2]. Initially, Tossy et al. [3] categorized AC joint injuries into types I, II, and III for treatment purposes. Later, Rockwood et al. [4] expanded on this classification, introducing types IV, V, and VI. This expansion acknowledged a range of complete AC dislocations [5]. The Rockwood classification system plays a crucial role in helping surgeons accurately diagnose AC joint injuries and is widely referenced in literature to determine whether non-operative or operative management is appropriate [6]. Expectant treatment can effectively resolve Rockwood type I and II injuries, whereas surgical intervention is typically necessary for Rockwood types IV, V, and VI ACD cases. However, the decision regarding operative treatment for type III injuries remains controversial which is one of the most common encountered injury types [7]. Many biomechanical investigations in the past few years have contributed to the advancement of surgical methods aimed at stabilizing the AC joint complex using fixation methods that mimic the natural anatomical structure more closely [8-10]. At present, several surgical options are successful in treating type III injuries, such as clavicular hook plate fixation (CHPF), tension band fixation using Kirschner wires, coracoclavicular (CC) ligament reconstruction, and others. However, surgical complications such as internal fixation loosening, post-operative shoulder pain, limited joint movement, and recurrence of joint dislocation after internal fixation removal remain significant concerns [7]. One technique gaining popularization is the endobutton technique, which has shown promising results and deserves wider adoption [11]. Using double-endobutton reconstruction for AC dislocation patients has significantly decreased post-operative complications and has been effective for AC dislocations, especially Rockwood type III injuries [12,13]. Efforts are continuously made to enhance double-endobutton reconstruction, focusing on streamlining surgical procedures, reinforcing internal fixation, minimizing complications, and improving the functional outcomes [7]. The present study aimed to investigate the functional outcomes of double endobutton technique treatment of Rockwood type III and V AC joint dislocations in our hospital. (Fig. 1).

The present retrospective study was conducted in the Department of Orthopedics at a tertiary care hospital in Punjab, India, for a duration of 1 year, after due approval from the institutional ethics committee and review board. (Fig. 2)
Inclusion criteria
- Patients with acute ACD with duration of <7 days
- Shoulder injury on one side
- Rockwood type III or V injury (diagnosed by computed tomography or magnetic resonance imaging [MRI])
- Patients with follow-up of 1 year.
Exclusion criteria
- Those with serious associated injuries (clavicular fracture, coracoid fracture); open shoulder injuries which would be infected easily; brachial plexus injuries
- Patients had anatomic variation of coracoid in shoulder.
Patients were enrolled in the study after taking written informed consent. The complete demographic details (such as age and gender), personal and clinical history, and injured side were taken. The mean age of the study subjects was 30.46 ± 6.3 years. Out of the total thirteen patients, eleven (84.62%) were males and two (15.38%) were female. Right side was injured in eleven (84.62%) cases, while the left side was affected in two (15.38%) cases. In ten cases (76.92%), the Rockwood grade was classified as grade III, while in three cases (23.08%), it was classified as grade V. All cases underwent open reduction and fixation using double endobutton suspensory technique using a direct longitudinal incision extending from coracoid process to lateral 1/3rd part of clavicle. Post-operative all patients were subjected to a three-phase rehabilitation regimen and given shoulder immobilizer for a minimum of the first 3 weeks, with initiation of pendulum movements, supine assisted forward flexion of shoulder, elbow and forearm active range of motion, scapula retraction, and depression exercises in PHASE I of the rehabilitation program. Once patient achieves 90° of passive shoulder flexion and 30° of passive external rotation (0–6 weeks), PHASE II is initiated with active side lying external rotation, and prone rowing along with shoulder extension is initiated. Active TheraBand strengthening of shoulder rotations, biceps curls, and serratus punch is also initiated (7–12 weeks). In Phase III (13–18 weeks), mobility and strengthening are continued with additional closed kinetic chain exercise of wall pushups. Most patients achieved functional arc by end of 8–12 weeks of the rehabilitation regimen. The functional outcomes of the patients were evaluated through scores such as Constant‑Murley score (CMS) [14], simple shoulder test [15], American Shoulder and Elbow surgeons (ASES) [16], AC joint instability (ACJI) [17], and TAFT [18], which were noted both at baseline and at 1-year follow-up.
Statistical analysis
The presentation of the categorical variables was done in the form of number and percentage (%). On the other hand, the quantitative data with normal distribution were presented as the means ± standard deviation. Repeated measure analysis of variance was used for comparison across follow-up. The data entry was done in the Microsoft Excel spreadsheet, and the final analysis was done with the use of Statistical Package for the Social Sciences software, IBM manufacturer, Chicago, USA, version 25.0. For statistical significance, P < 0.05 was considered statistically significant.

All patients had a minimum of 1-year follow-up in the records. CMS scores increased from a pre-operative mean of 30.77–96.31, at 1-year post-operation (96.31 ± 2.81) (P < 0.0001). Similarly, the mean simple shoulder test improved at 1 year (96.81 ± 4.2), in comparison to 6 months (95.53 ± 4.31), 3 months (80.76 ± 7.12), post-operation (26.28 ± 6.65), and pre-operation values (19.23 ± 7.9). The ASES score also increased from 29.31 pre-operatively to 98.92 at 1 year. ACJI also increased from 41.38 pre-operative to 98.08 at 1 year. In addition, the TAFT score displayed notable advancement, escalating from 4.31 pre-operative to 11.62 at 1-year follow-up (Table 1 and Fig. 4a-e). Out of 13 patients, 1 patient had painful arc at the time of last follow-up which was evaluated and diagnosed with partial thickness supraspinatus tear for which ultrasound (USG)-guided corticosteroid was administered later and 1 patient had surgical site dehiscence which was conservatively managed with regular dressings and delayed suture removal was done.

The endobutton technique, designed to reconstruct the CC ligament and restore normal AC joint function, has become a standard procedure in clinical management [19] Struhl [20] first introduced the double endobutton technique in 2007, aiming to reduce joint subluxation and fractures. His work illustrated that stability in the AC joint could be preserved by positioning a suture button construct between the coracoid process and the distal clavicle, offering superior strength and stiffness compared to the natural ligament [19]. Our study found significant functional improvement in patients with AC dislocations as assessed by different scoring scales (P < 0.0001). Similar findings were noted in the study by Das et al., [21] as at the follow-up of 1 year, CMS improved postoperatively compared to preoperatively (95.4% vs. 35.2%, P < 0.001). The good functional scores achieved in the study were attributed to the meticulous surgical technique as well as intensive post-operative rehabilitation programEvery patient underwent surgery within a week of their injury, which contributed to the positive outcome as early surgery is known to yield better results, reduce infection risks, avoid more invasive procedures, minimize graft-related issues, and eliminate the need for distal end clavicle removal [21]. This was in accordance with the findings of Zhang et al. [7] as at 1 year postoperatively, the functional scores, i.e., CMS (100 vs. 50), University of California at Los Angeles shoulder rating scale (32 vs. 15), ASES (80 vs. 50), oxford shoulder score (18 vs. 42), and CC‑interval (16 vs. 7) were better as compared to pre-operative values (P < 0.05). Thereby signifying the importance of early and precise surgical management in such patients. Even in the study by Wang et al., [22] at the follow-up of 2 years, there was improvement in CMS compared to pre-operative values (93.27 ± 1.59 vs. 69.73 ± 3.29, P < 0.001). In an Indian study by Dey et al., [23] on twenty patients who underwent double endobutton technique, constant shoulder score was excellent in ten (50%) cases and good in eight (40%) cases. The mean post-operative CSS was 88.15 ± 10.15. Similarly, improvement in the mean Constant score was seen in the study by Hu et al. [24] postoperatively at the at the final follow-up compared to pre-operative values (94.0 ± 0.73 vs. 45.5 ± 2.0). In another study, Hu et al. [25] investigated the clinical efficacy of double endobutton reconstruction of the CC ligament combined with repair of the AC ligament in stage I ACD cases, reporting good early results. Struhl et al. [26] compared the stability of a novel closed-loop double-endobutton construct with a commercially available cortical button system, finding good stability with the closed-loop double-endobutton construct in both axial and superior directions. Sharma et al. [27] also supported our results and found a post-operative follow-up CMS of 91.17 using mini-invasive double endobutton in patients with acute AC joint dislocation grade III and V. In addition, Struhl and Wolfson [28] conducted a long-term follow-up study on 31 patients who underwent the closed-loop double-endobutton technique for acute and chronic ACD (Rockwood type III), the CMS was 98; the study reported this technique as a low-profile that maintained a stable AC joint while allowing for strong soft tissue healing. The findings were also supported by Satishkumar et al., [29] and Goel et al. [30]. Double endobutton technique – with its good efficacy and safety; certainly, better than CHPF technique in terms of functional outcomes [7] – is being further improvised with the modified closed double endobutton technique. The advantages of double end button technique are the distribution of physiological loads across two surfaces rather than solely on the suture, reducing the likelihood of suture failure [21]. In addition, burying the endobutton beneath soft tissues prevents skin irritation and eliminates the need for additional surgery to remove hardware [29]. Overall, this technique achieves a functional and anatomically accurate reconstruction of the CC ligament without the need for extensive joint dissection [28]. But, given its intricacy, the surgical duration is certainly prolonged – but it remains insignificant in comparison to the advantages offered by it [31-33]. In our study, only one patient had surgical wound dehiscence at post-operative day 14, managed with regular dressings and extended oral antibiotics. One patient had painful arc at the end of the rehabilitation program, for which MRI was done and was diagnosed with partial tear supraspinatus tear. USG-guided corticosteroid was injected for the same, with patient having full recovery at the final follow-up.
Limitation of study
The study had a limited sample size and a relatively short follow-up duration. Moreover, the study did not compare the double endobutton technique and other surgical techniques. Since our study is a retrospective study, we could not collect the data of the normal side.
The closed loop double endobutton technique proved effective in treating acute type III AC joint dislocations, yielding good functional outcomes. This technique can be applied to both open surgeries and arthroscopic procedures, eliminating the necessity for a secondary removal procedure. It is a simple yet highly effective technique, consistently yielding successful results in stabilizing the AC joint and facilitating physiological healing in acute injuries.
The double endobutton technique effectively restores the normal CC distance and the AC joint anatomy and can be used arthroscopically as well. It has the potential to improve functional outcomes and patient satisfaction compared to other surgical techniques.
References
- 1.Kim AC, Matcuk G, Patel D, Itamura J, Forrester D, White E, et al. Acromioclavicular joint injuries and reconstructions: A review of expected imaging findings and potential complications. Emerg Radiol 2012;19:399-413. [Google Scholar | PubMed]
- 2.Tauber M. Management of acute acromioclavicular joint dislocations: Current concepts. Arch Orthop Trauma Surg 2013;133:985-95. [Google Scholar | PubMed]
- 3.Tossy JD, Mead NC, Sigmond HM. Acromioclavicular separations: Useful and practical classification for treatment. Clin Orthop Relat Res 1963;28:111-9. [Google Scholar | PubMed]
- 4.Rockwood CJ, Williams G, Young D. Disorders of the acromioclavicular joint. In: Rockwood CJ, Matsen FA III, editors. The Shoulder. 2nd ed. Philadelphia, PA: WB Saunders; 1998. p. 483-553. [Google Scholar | PubMed]
- 5.Guy DK, Wirth MA, Griffin JL, Rockwood CA Jr. Reconstruction of chronic and complete dislocations of the acromioclavicular joint. Clin Orthop Relat Res 1998;347:138-49. [Google Scholar | PubMed]
- 6.Gorbaty JD, Hsu JE, Gee AO. Classifications in brief: Rockwood classification of acromioclavicular joint separations. Clin Orthop Relat Res 2017;475:283-7. [Google Scholar | PubMed]
- 7.Zhang L, Zhou X, Qi J, Zeng Y, Zhang S, Liu G, et al. Modified closed-loop double-endobutton technique for repair of rockwood type III acromioclavicular dislocation. Exp Ther Med 2018;15:940-8. [Google Scholar | PubMed]
- 8.Von Heideken J, Bostrȍm Windhamre H, Une-Larsson V, Ekelund A. Acute Surgical treatment of acromioclavicular dislocation type V with a hook plate: Superiority to late reconstruction. J Shoulder Elbow Surg 2013;22:9-17. [Google Scholar | PubMed]
- 9.Wellmann M, da Silva G, Lichtenberg S, Magosch P, Habermeyer P. Instability pattern of acromioclavicular joint dislocations type Rockwood III: Relevance of horizontal instability. Orthopade 2013;42:271-7. [Google Scholar | PubMed]
- 10.Kezunović M, Bjelica D, Popović S. Comparative study of surgical treatment of acromioclavicular luxation. Vojnosanit Pregl 2013;70:292-7. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management
August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management August 1, 2026 Outcome Analysis of Loop Endobutton Repair for Acromioclavicular Joint Dislocation
August 1, 2026 Outcome Analysis of Loop Endobutton Repair for Acromioclavicular Joint Dislocation June 1, 2026 Prospective Evaluation of Clavicle Fracture Osteosynthesis: Patient Satisfaction, Clinical, and Radiological Outcomes with Clavipectoral Fascial Plane Block
June 1, 2026 Prospective Evaluation of Clavicle Fracture Osteosynthesis: Patient Satisfaction, Clinical, and Radiological Outcomes with Clavipectoral Fascial Plane Block March 1, 2026 Pull Out Suture Technique for Fixing Coronoid Fractures using a Single Lateral Extensor Digitorum Communis Split Approach and Fiberwire Endobutton Fixation by Retrograde Drilling – A Case Series
March 1, 2026 Pull Out Suture Technique for Fixing Coronoid Fractures using a Single Lateral Extensor Digitorum Communis Split Approach and Fiberwire Endobutton Fixation by Retrograde Drilling – A Case Series