
Giant cell tumors in the distal tibiaa rare entity and limb salvage can be achieved effectively by excision and reconstruction by bone transport.
Dr. K Tarun Prashanth, Department of Orthopaedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai, Tamil Nadu, India. E-mail: tarun10007@gmail.com
Abstract
Introduction: Giant cell tumor (GCT) is a benign, locally aggressive neoplasm commonly affecting the ends of long bones. Treatment varies based on tumor stage and includes curettage, bone grafting, resection, wide excision, prosthetic reconstruction, radiation, and embolization. This case report presents a rare GCT of the distal tibia managed with wide excision and reconstruction with an Ilizarov ring fixator.
Case Report: A 36-year-old male presented with progressively enlarging right ankle swelling for 3 months, accompanied by dull, diffuse pain aggravated by weight-bearing. He reported significant weight loss over 6 months but no history of trauma. Radiographs confirmed the diagnosis and higher investigations were done to stage the disease. After a multidisciplinary discussion with surgical oncology, he underwent wide excision and bone transport using an Ilizarov ring fixator.
Results: The case was managed with the above-mentioned procedure, distraction was done for a period of 90 days, and the frame was removed after union at the docking site. Post-removal radiographs were done to confirm union at the distraction site and docking site. The patient gradually started weight-bearing in the limb.
Conclusion: Periarticular long bone tumors can be managed effectively with resection and bone transport. Although it has a few disadvantages, such as the long duration of external fixator and pin tract infections, it remains a reliable option for limb reconstruction, offering cost-effectiveness and proven long-term success.
Keywords: Giant cell tumor, distal tibia, ilizarov, bone transport, limb reconstruction.
Giant cell tumor (osteoclastoma) is a locally aggressive benign neoplasm representing around 4–5% of all primary bone neoplasms and more than 20% of benign primary bone tumors [1]. It usually affects young adults, and the peak incidence is seen at around 20–45 years of age. Giant cell tumors (GCTs) have a low metastatic potential but a high propensity to recur locally following treatment [2]. The primary areas of involvement are the ends of long bones, such as the distal femur, proximal tibia, proximal humerus, or distal radius [1-4]. Various management protocols have been employed based on the stage of the tumor, including curettage with chemical or physical agents, bone grafting, primary resection, wide excision and reconstruction with grafts or custom prosthesis, radiation therapy, or embolization [2,3,5].
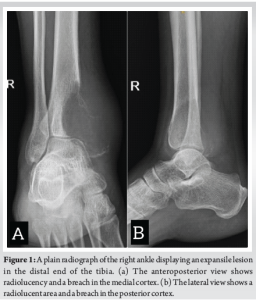
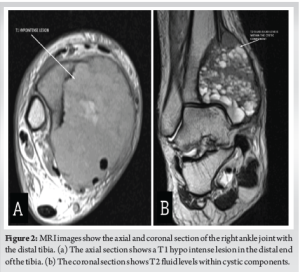
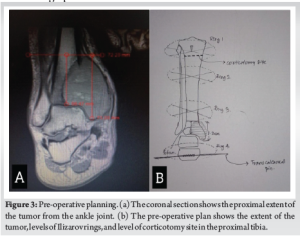
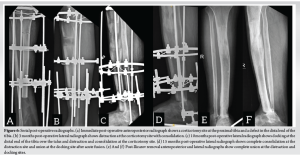
A 36-year-old male presented after noticing a gradually increasing swelling over his right ankle for the past 3 months. It was associated with a dull and diffuse type of pain which was aggravated with weight bearing. He denied a history of any previous trauma. He had noticed significant weight loss in the past 6 months. On clinical examination, there was a localized swelling of size 5 × 3 cm over the medial aspect of the ankle, which was tender, immobile, with ill-defined edges, and was bony hard in consistency. The range of movements in the ankle was minimally restricted in comparison with the contralateral side. There was no neurovascular deficit in the affected limb. Plain radiographs of the affected limb were done and showed an ill-defined, radiolucent, expansile lesion in the medial aspect of the distal end of the tibia, with a posteromedial cortical breach and a narrow zone of transition (Fig. 1a and b). Magnetic resonance imaging of the affected limb was performed and showed a T1 hypointense lesion of size 6.1 × 4.7 × 7.3 cm in the epi-metaphyseal region of the distal tibia (Fig. 2a), with multiple cystic areas and fluid levels (Fig. 2b) – suggestive of giant cell tumor of the distal tibia with secondary aneurysmal bone cyst formation. Biopsy was performed from the lesion, under ultrasound guidance, and showed osteoclast-like giant cells and neoplastic cells with ill-defined borders and eosinophilic cytoplasm, suggestive of giant cell tumor. Based on the radiographic appearance, the tumor was classified according to the Campanacci grading as Type III owing to the presence of ill-defined margins and a cortical breakthrough. After a thorough review of the literature and a multidisciplinary discussion with the surgical oncology team in assessing all the possible options of intervention, pre-operative planning was done, and the patient underwent wide excision of the tumor and was planned for bone transport with an Ilizarov ring fixator (Fig. 3a and b). The patient was positioned supine on the operating table with a primary surgeon on the right side and an image intensifier on the contralateral side. The skin incision was made over the posteromedial aspect, extending from the distal third of the leg to mid-foot (Fig. 4a). The flap was raised posteriorly (Fig. 4b), posterior compartment was dissected, and the great saphenous vein was isolated along its course. Tumor margins were identified, and tibia was osteotomized, giving a 3 cm clearance proximal to the tumor (Fig. 4c). Ligaments around the ankle were cut, and the distal end of the tumor was visualized. The tumor, along with the encased tibialis posterior, was removed in toto (Fig. 4d) and was sent for histopathological examination. A thorough wash was given, and the wound was closed. Three equidistant Ilizarov rings were fixed around the tibia proximal to the osteotomy site using tensioned wires and were interconnected with threaded rods. A half ring was fixed around the midfoot with tensioned wires and connected to the proximal rings (Fig. 5). Proximal tibial corticotomy was done at a level between the proximal and middle rings. Postoperatively, distraction was started from day 7, at the rate of 1mm/day, and was continued for a period of 90 days, resulting in a distraction of 90 mm at the corticotomy site, thereby filling the defect in the distal tibia. Serial radiographs were done to look for consolidation of the regenerate at distraction site and docking of the stump over the talus (Fig. 6a-c). 90 days later, once docking was complete (Fig. 6d), distraction was stopped, and the frame was retained for a period of 180 days, allowing for consolidation of regenerate at the distraction site. Once clinical and radiological signs of union were confirmed at the distraction site, acute docking was performed, and fusion at the ankle was done. The Ilizarov frame was then retained for a period of 6 months. After 6 months, once complete union was noticed at the docking site, the frame was (Fig. 6e and f). The patient was then gradually made to weight bear partially with a walker frame for a period of 4 weeks. Later he was allowed full weight-bearing walking, initially with a walker frame for 2 weeks, followed by an elbow crutch for 2 weeks and unassisted subsequently. He was last followed up 2½ years postoperatively and showed no clinical or radiological signs of recurrence. He was able to walk unassisted with a plantigrade foot. Dorsiflexion and plantarflexion at the ankle were not possible. Minimal passive inversion and eversion movements at the subtalar joint were preserved.


GCTs in the distal tibia are relatively rare, and surgery is the mainstay of treatment to reduce the risk of recurrence [10]. Management aims at a balance between adequate removal and restoration of limb function [10]. Treatment with isolated curettage has been associated with a high risk of recurrence. Hence, augmenting curettage with the use of adjuvants such as cryosurgery, phenol, or cement is recommended, followed by reconstruction with grafts or hydroxyapatite [9]. Tumors with extensive cortical destruction, requiring wide resection with tumor clearance, leave behind a void in long bones and weight-bearing joints, more commonly the knee or ankle joints. This requires reconstructive procedures to be performed, which aim at biomechanics, durability, infection resistance, biological healing, and restoring the functional aspect of the affected joint [6,10]. This can be achieved by reconstructing the joint with a custom-made prosthesis [8]. Although it requires a single surgical procedure and minimal hospitalization, high cost, longer rehabilitation and chances of infection have limited its widespread adoption [9]. Reconstruction of the periarticular bony defect by bone transport with an Ilizarov fixator is a viable alternative [7]. It involves an extended period of rehabilitation associated with patient non-compliance and prolonged duration of the external fixator. Nevertheless, it can be adopted and is an efficient mode of management owing to its low cost and its long-lasting outcome. Our case was managed successfully with the above-mentioned procedure, and complete biological healing was observed.
There are very few documented cases of Ilizarov-assisted reconstruction for GCTs in the distal tibia. Bone regeneration with distraction osteogenesis is a highly effective limb salvage procedure. Patients with defects of <10 cm are good candidates to undergo these procedures, and have proven to be an economical tool for reconstructing limbs.
GCTs affecting the distal tibia are a rare entity. Early detection with appropriate imaging and histopathological evaluation is crucial. The preferred treatment approach focuses on limb salvage. When periarticular regions of long bones are involved, wide resection combined with bone defect reconstruction using an Ilizarov fixator is a viable option for preserving the limb and achieving good functional outcomes.
References
- 1.Eckardt JJ, Grogan TJ. Giant cell tumour of bone. Clin Orthop Relat Res 1986;204:45-58. [Google Scholar | PubMed]
- 2.Van Der Heijden L, Dijkstra PS, Van De Sande MA, Kroep JR, Nout RA, Van Rijswijk CS, et al. The clinical approach toward giant cell tumour of bone. Oncologist 2014;19:550-61. [Google Scholar | PubMed]
- 3.Napoli R, Mukherjee A, Rossi M. Distal tibia giant cell tumour surgical treatment: A case report. Foot Ankle Surg Tech Rep Cases 2024;4:100352. [Google Scholar | PubMed]
- 4.Georgiev GP, Slavchev SA. Giant cell tumour of the distal tibia: Report of a rare case. J Clin Exp Invest 2013;4:512-6. [Google Scholar | PubMed]
- 5.Aktuglu K, Erol K, Vahabi A. Ilizarov bone transport and treatment of critical-sized tibial bone defects: A narrative review. J Orthop Traumatol 2019;20:22. [Google Scholar | PubMed]
- 6.Xie L, Huang Y, Zhang L, Si S, Yu Y. Ilizarov method and its combined methods in the treatment of long bone defects of the lower extremity: Systematic review and meta-analysis. BMC Musculoskelet Disord 2023;24:891. [Google Scholar | PubMed]
- 7.Aggarwal AN, Jain AK, Kumar S, Dhammi IK, Prashad B. Reconstructive procedures for segmental resection of bone in giant cell tumours around the knee. Indian J Orthop 2007;41:129-33. [Google Scholar | PubMed]
- 8.Reinke C, Bäcker H, Lotzien S, Schildhauer TA, Seybold D, Gessmann J. Arthrodesis of the infected knee joint with the Ilizarov external fixator: An analysis of 13 cases. Z Orthop Unfall 2020;158:58-74. [Google Scholar | PubMed]
- 9.Bari MM, Islam S, Shetu NH, Rahman W, Rahman M, Munshi MH, et al. Giant cell tumours (GCT) around knee-curettage and reconstruction by Ilizarov technique. MOJ Orthop Rheumatol 2015;3:239-42. [Google Scholar | PubMed]
- 10.Mankar VE, Agrawal SP. Limb reconstruction using the Ilizarov technique following giant cell tumour excision in the proximal tibia of a 19-year-old female: A case report. Cureus 2024;16:e57434. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Patient-specific Distal Tibia Prosthesis for Reconstruction in a Case of Recurrent Giant Cell Tumor – A Case Report
March 1, 2026 Patient-specific Distal Tibia Prosthesis for Reconstruction in a Case of Recurrent Giant Cell Tumor – A Case Report May 10, 2021 A Rare Case of Ewing’s-like Adamantinoma of Tibia Managed by Limb Salvage Surgery Using Long Segment Ilizarov Bone Transport: A Case Report and Review of Literature
May 10, 2021 A Rare Case of Ewing’s-like Adamantinoma of Tibia Managed by Limb Salvage Surgery Using Long Segment Ilizarov Bone Transport: A Case Report and Review of Literature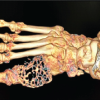 June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction
June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction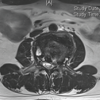 May 1, 2026 Combined Post-operative Denosumab and Oral Bisphosphonate Therapy Following Resection of Spinal Giant Cell Tumor: A Case Report
May 1, 2026 Combined Post-operative Denosumab and Oral Bisphosphonate Therapy Following Resection of Spinal Giant Cell Tumor: A Case Report