
In rare and complex scapulothoracic disruptions involving both scapular and acromial fractures, a multistructural approach using dual-column scapular plating and acromial tension band osteosynthesis can achieve excellent anatomical restoration and functional outcomes.
Dr. Avik Kumar Naskar, Department of Orthopaedics, Indira Gandhi Government Medical College and Hospital, Nagpur, Maharashtra, India. E-mail: avik7933@gmail.com
Abstract
Introduction: Scapulothoracic disruptions with associated scapular and acromial fractures are extremely rare and complex injuries, with limited guidance available in the current literature regarding their combined surgical management. These injuries can severely impair shoulder stability and function, necessitating anatomical reconstruction to restore biomechanics.
Case Report: We present the case of a 43-year-old male who sustained a high-energy trauma resulting in a type 1 scapulothoracic disruption (Zelle’s classification), including fractures of the scapular body, lateral border, and acromion process. Surgical intervention involved dual-column reconstruction plate fixation of the scapula and tension band osteosynthesis for the acromion. Postoperative rehabilitation led to excellent radiological union and full functional recovery, with return to all activities by 4 months.
Conclusion: This case highlights the importance of anatomical fixation in restoring both scapulothoracic and glenohumeral mechanics. Dual-column plating provided stable scapular reconstruction, while acromial fixation ensured deltoid reattachment and preservation of shoulder abduction. The combined approach yielded a favorable clinical outcome in a rare injury pattern and was successfully delivered free of cost under a government-funded healthcare scheme. Biomechanically sound surgical constructs and guided post-operative rehabilitation are a key to optimal recovery in such complex injuries.
Keywords: Scapular fractures, shoulder injuries, acromial fractures, tension band wiring, shoulder girdle injuries.
Scapulothoracic disruptions are severe injuries usually resulting from high-energy trauma. They may involve the scapular body, spine, lateral border, and acromion and are often associated with chest wall or clavicular injuries. These injuries compromise shoulder mechanics and require stable reconstruction to prevent chronic dysfunction. While isolated scapular plating and acromial fixation have been described individually, there is limited documentation of cases managed with both dual-column scapular plating and acromion tension band wiring in the same setting. To the best of our knowledge, this is the only case report presenting such a scenario demonstrating excellent radiographic and functional results following comprehensive surgical intervention.
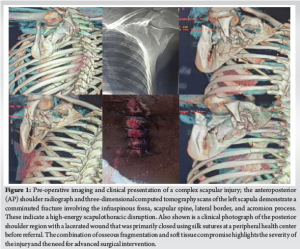
A 43-year-old right-hand-dominant male was brought to our institute following a high. Initial evaluation revealed extensive scapulothoracic injury with displaced fractures of the left (non-dominant side) scapular body, lateral column, and acromion process (Fig. 1) without any vascular or neurological deficits (Type 1, Zelle et al. [1]). Computed tomography scans confirmed significant disruption of the scapular architecture with lateral displacement of more than 2 cm and shortening, as well as fracture of the acromion (Fig. 2).

Informed consent was taken from the patient and his relatives, following which he underwent surgical stabilization. Through the Judet approach, after elevating the infraspinatus muscle from the infraspinous fossa and retracting it laterally, the posterior aspect of the scapula was exposed in its entirety. After securing the suprascapular nerve and artery at the spinoglenoid notch, anatomical reduction of the scapular body and lateral column was achieved and fixed with 3.5 mm reconstruction plates in a dual-column configuration (Fig. 3). The acromion fracture was separately addressed through superior scapular approach. Tension band wiring was done using two 2 mm Kirschner wires and a 1.5 mm stainless steel wire wound in a figure-of-eight fashion to achieve compression and restore the deltoid insertion (Fig. 4).
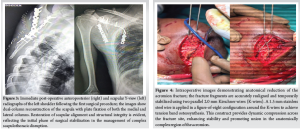
Post-operative rehabilitation included early passive motion followed by active-assisted range of motion at 4 weeks. At 4 months, the patient demonstrated active shoulder abduction up to 120° (Fig. 5), minimal pain (Visual Analogue Scale 1/10), and radiographic evidence of fracture union (Fig. 6). The University of California, Los Angeles Shoulder Score following a questionnaire was found to be 34/35 and the Constant–Murley score was 95/100, again confirming an excellent outcome [2,3].

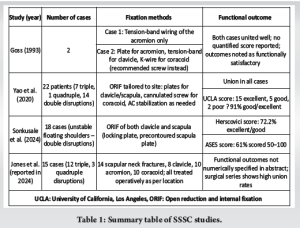
Scapular plating is commonly indicated in cases of medial/lateral column disruption, >25 mm displacement, or angulation >45° [4,5]. Acromial fractures are typically treated conservatively but may require tension band wiring or plating when displaced or impeding shoulder motion [6-8]. To the best of our knowledge, no reports exist describing the combined use of dual-column plating and acromial fixation in the same patient. Goss introduced the concept of the superior shoulder suspensory complex (SSSC) and emphasized the need for restoration of all its components to prevent instability [9,10]. This case supports this biomechanical principle by treating both the lateral scapular border and acromion, which are integral to the SSSC [Table 1].
Jain et al. reported good outcomes using tension band wiring in isolated acromion fractures [11], while Herrera et al. found dual-column scapular fixation yielded better functional recovery compared to single-plate constructs in complex fractures [12].
Qalib et al. reported good outcome in a displaced acromion fracture treated with three cannulated cancellous screws perpendicular to the fracture [13]. Hollensteiner et al. concluded that double plating approach with two locking plate constructs bore good results in Levy type III acromion fractures [14]. Bauer et al. reported a durable result after double plating of entire scapular spine and acromion with concurrent reverse shoulder arthroplasty in a case of rotator cuff arthropathy with scapular spine fracture [15]. Hsiue et al. demonstrated an excellent outcome of dual plating of the acromion along with arthroscopic capsulolabral repair in a patient with an acromion fracture with first-time anterior shoulder dislocation. A 2.7 mm variable angle distal clavicle plate was used along the superior aspect of scapular spine up to the acromion and a 3.5 mm reconstruction plate was placed posteriorly in their report [16]. However, concurrent fixation of scapular body, lateral border, and acromion has not been extensively documented, making this case noteworthy in the field of complex trauma. Successful shoulder function depends on the integrity of the scapular body, lateral border, acromion, and surrounding musculature. Disruption of multiple components, as seen in this case, requires an individualized surgical strategy aimed at restoring anatomy and biomechanics. The dual-column scapular plating ensured proper restoration of the scapular contour and glenoid alignment, while acromial fixation maintained deltoid lever arm function. The combination prevented scapular winging and shoulder weakness – common complications in scapulothoracic injuries. Rehabilitation played a critical role in achieving excellent outcomes, considering this was the patient’s non-dominant arm, emphasizing the importance of early mobilization post-stabilization.
This case demonstrates that a comprehensive surgical approach combining scapular dual-column plating and acromion tension band osteosynthesis can lead to excellent radiological union and functional recovery in patients with complex scapulothoracic disruption. Surgeons should consider early and anatomical reconstruction of all disrupted components of the shoulder girdle in high-energy injuries to optimize outcomes.
Timely anatomical fixation using dual-column scapular plating and acromial tension band wiring, combined with structured rehabilitation, can restore shoulder function and stability within a short time in rare scapulothoracic disruptions with associated fractures.
References
- 1.Zelle BA, Pape HC, Gerich TG, Garapati R, Ceylan B, Krettek C. Functional outcome following scapulothoracic dissociation. J Bone Joint Surg Am 2004;86:2-8. [Google Scholar | PubMed]
- 2.Amstutz HC, Sew Hoy AL, Clarke IC. UCLA anatomic total shoulder arthroplasty. J Orthop Trauma. 2006 Sep;20(8 Suppl):S139–40. doi:10.1097/01.bot.0000238810.95222. [Google Scholar | PubMed | CrossRef]
- 3.Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res 1987;214:160-4. [Google Scholar | PubMed]
- 4.Ada JR, Miller ME. Scapular fractures. Analysis of 113 cases. Clin Orthop Relat Res 1991;269:174-80. [Google Scholar | PubMed]
- 5.Zlowodzki M, Bhandari M, Zelle BA, Kregor PJ, Cole PA. Operative versus nonoperative treatment of scapula fractures: A meta-analysis. J Orthop Trauma 2009;23:579-85. [Google Scholar | PubMed]
- 6.Hill BW, Anavian J, Jacobson AR, Cole PA. Surgical management of isolated acromion fractures: Technical tricks and clinical experience. J Orthop Trauma 2014;28:e107-13. [Google Scholar | PubMed]
- 7.Ogawa K, Naniwa T. Fractures of the acromion and the lateral scapular spine. J Shoulder Elbow Surg 1997;6:544-8. [Google Scholar | PubMed]
- 8.Hardegger FH, Simpson LA, Weber BG. The operative treatment of scapular fractures. J Bone Joint Surg Am 1984;66:725-31. [Google Scholar | PubMed]
- 9.Goss TP. The scapula: Coracoid, acromial, and avulsion fractures. Am J Orthop (Belle Mead NJ) 1996;25:106-15. [Google Scholar | PubMed]
- 10.Goss TP. Double disruptions of the superior shoulder suspensory complex. J Orthop Trauma 1993;7:99-106. [Google Scholar | PubMed]
- 11.Jain P, Atram V, Mittal A, Arora C. Tension band wiring in a rare case of isolated acromion fracture: A case report. Int J Res Orthop 2022;8:761-4. [Google Scholar | PubMed]
- 12.Herrera DA, Anavian J, Tarkin IS, Armitage BA, Schroder LK, Cole PA. Clinical outcomes of surgical treatment of displaced scapular fractures. J Shoulder Elbow Surg 2009;18:431-6. [Google Scholar | PubMed]
- 13.Qalib YO, Medagam SR, Dachepalli S. Ipsilateral fractures of the acromion and coracoid processes of the scapula. Chin J Traumatol 2024;27:121-4. [Google Scholar | PubMed]
- 14.Hollensteiner M, Sandriesser S, Rittenschober F, Hochreiter J, Augat P, Ernstbrunner L, et al. Single or double plating for acromial type III fractures: Biomechanical comparison of load to failure and fragment motion. J Clin Med 2022;11:3130. [Google Scholar | PubMed]
- 15.Bauer S, Traverso A, Walch G. Locked 90°-double plating of scapular spine fracture after reverse shoulder arthroplasty with union and good outcome despite plate adjacent acromion fracture. BMJ Case Rep 2020;13:e234727. [Google Scholar | PubMed]
- 16.Hsiue P, Chiou D, Shi B, Ahlquist S, Jensen A, Cheung E. Acromion fracture associated with traumatic first time anterior shoulder dislocation: A case report. JSES Rev Rep Tech 2023;4:284-90. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 A Prospective Study of Comminuted Patellar Fractures Treated with Different Fixation Modalities: Functional Outcomes and Complications
June 1, 2026 A Prospective Study of Comminuted Patellar Fractures Treated with Different Fixation Modalities: Functional Outcomes and Complications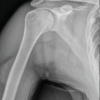 June 1, 2026 Traumatic Asymmetric Bilateral Shoulder Dislocation: The First Case Report in Mexico
June 1, 2026 Traumatic Asymmetric Bilateral Shoulder Dislocation: The First Case Report in Mexico March 1, 2026 A Rare Case of Combined Tibial Plateau Fracture with Tibial Tuberosity Avulsion Injury: Case Report
March 1, 2026 A Rare Case of Combined Tibial Plateau Fracture with Tibial Tuberosity Avulsion Injury: Case Report October 1, 2024 Comparative Study of Inferior Pole of Patella Fracture Treated with Transosseous Technique using Modified Krackow’s Technique Versus Traditional Anterior Tension Band Wiring
October 1, 2024 Comparative Study of Inferior Pole of Patella Fracture Treated with Transosseous Technique using Modified Krackow’s Technique Versus Traditional Anterior Tension Band Wiring