
Combined anterior latissimus dorsi and teres major (aLDTM) tendon transfer is an effective and safe joint preserving treatment option for anterosuperior irreparable rotator cuff tears (ASIRCTs) in one-arm patients.
Dr. Chang Hee Baek, Department of Orthopaedic Surgery, Yeosu Baek Hospital, Yeosu, Republic of Korea. E-mail: yeosubaek@gamail.com
Abstract
Introduction: One-arm patients experience a severe burden on the shoulder joint during daily activities, which lead to rotator cuff tears or degenerative joint disease over time. While anterosuperior irreparable rotator cuff tears (ASIRCTs) cause severe shoulder pain and functional impairments, surgeons face challenges due to the lack of a clear treatment protocol. Recently, combined anterior latissimus dorsi and teres major (aLDTM) tendon transfer has emerged as a reasonable treatment option for ASIRCTs. However, there are currently no studies on aLDTM tendon transfer as a joint preserving treatment for ASIRCTs in one-arm patients.
Case Report: Totally three one-arm patients were treated with aLDTM tendon transfer for ASIRCTs. The mean age was 55.3 ± 2.1 years old, and all patients were male. Two patients had paralytic limb weakness due to brachial plexus injury and one patient had a one-arm weakness due to burn injury. Three patients showed improvement in clinical outcomes including visual analog scale score, patient reported outcome measurements, active range of motion (aROM), and aROM strength without progression of arthritis or any complications.
Conclusion: Based on these results, it has been confirmed that aLDTM tendon transfer is an effective and safe joint preserving treatment option for ASIRCTs in one-arm patients.
Keywords: One-arm patients, irreparable rotator cuff tears, anterior latissimus dorsi and teres major tendon transfer.
Patients with an amputation or paralysis of the contralateral upper limb (one-arm patients) rely on their healthy arm for daily activities [1]. One-arm patients rely on their healthy one arm, which can lead to overuse injuries such as rotator cuff tears or degenerative joint disease [1]. This can lead to rotator cuff tears or degenerative joint disease over time. This may lead to the need for shoulder surgery in one-arm patients [1]. However, shoulder surgery in these patients may raise special concerns. Since shoulder surgery and the rehabilitation process can limit daily activities, patients may require assistance from others for essential tasks and mobility [1]. In addition, even after surgery, the operated shoulder may be subjected to significant pressure and tension, increasing the risk of complications such as retear of the repaired rotator cuff or loosening of the reverse shoulder arthroplasty (RSA) component [1]. Therefore, this makes the decision for surgery more challenging, as the risks of complications and post-surgical limitations must be carefully considered. Anterosuperior irreparable rotator cuff tears (ASIRCTs), which involve the supraspinatus and subscapularis tendons, can result in severe pain and restricted shoulder motion, significantly impairing daily activities [2]. Although relatively uncommon and less frequently documented in literature, ASIRCTs remain a therapeutic challenge for orthopedic surgeons. Available surgical options as a joint preserving treatment options include arthroscopic debridement, partial cuff repair, biceps rerouting, superior capsular reconstruction, and tendon transfers [3,4,5]. However, these approaches often produce limited and gradually diminishing clinical improvements over time [6]. Recently, combined anterior latissimus dorsi and teres major (aLDTM) tendon transfer has gained attention as a potential treatment alternative for ASIRCTs [6]. Clinical reports have demonstrated notable reductions in pain and functional gains – particularly in internal rotation (IR) – following this procedure [6]. These improved outcomes are believed to stem from the biomechanical benefits conferred by the aLDTM tendon transfer technique [7]. To our best knowledge, there was only one study have reported clinical outcomes of RSA in one-arm patients [1]. However, there are currently no studies on joint-preserving treatment, such as aLDTM tendon transfer in one-arm patients with ASIRCTs. Therefore, this case report presented the clinical outcomes of combined aLDTM tendon transfer as a joint-preserving treatment in one-arm patients with ASIRCTs.
This case report reviewed the three one-arm patients who underwent aLDTM tendon transfer for ASIRCTs between 2020 and 2022 (minimum 2 years follow-up). One-arm patients were defined as those who rely on the ipsilateral arm due to a non-functional contralateral upper limb, which is limited in daily activities due to conditions such as amputation, palsy, or paralysis. Written informed consent was obtained from the patients. The criteria used to diagnose ASIRCTs included: (1) extensive rotator cuff tears involving both the subscapularis and supraspinatus tendons; (2) substantial tendon retraction and shortening to the level of the glenoid, corresponding to Patte stage III on magnetic resonance imaging (MRI); (3) advanced fatty degeneration in the affected tendons, classified as Goutallier grade 3 or 4; (4) a structurally preserved or reparable infraspinatus tendon with Goutallier grade 2 or lower; and (5) intraoperative confirmation that tendon mobilization was insufficient to allow reattachment to the humeral head footprint, even after thorough soft-tissue release (Fig. 1).
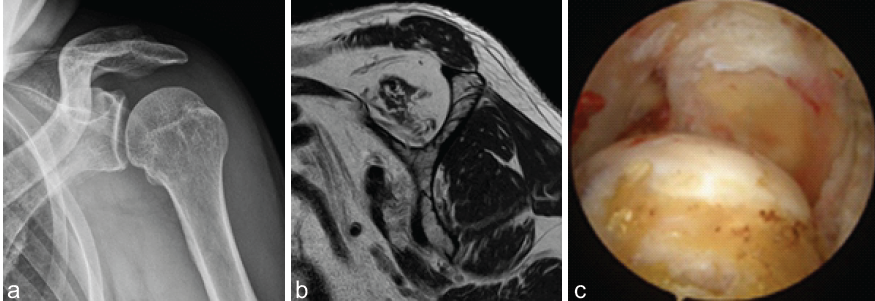
Figure 1: The diagnosis of anterosuperior irreparable rotator cuff tears. (a) An anteroposterior plane radiograph of the left shoulder shows minimal arthritis in the left shoulder joint (Hamada I). (b) A pre-operative T1-weighted oblique magnetic resonance imaging of the left shoulder demonstrates severe fatty infiltration of the subscapularis and supraspinatus tendons. (c) A diagnostic arthroscopic image of the left shoulder indicates relatively intact glenoid and humeral cartilage, and an empty footprint of the subscapularis and supraspinatus.
The surgical indications for aLDTM tendon transfer in ASIRCTs were as follows: (1) symptomatic cases marked by persistent shoulder pain and functional impairment impacting daily life; (2) failure to achieve improvement through conservative therapy for a minimum of six months; (3) minimal or early-stage glenohumeral arthritis (Hamada grade I or II); and (4) absence of neurological impairments or infectious conditions (Fig. 2).
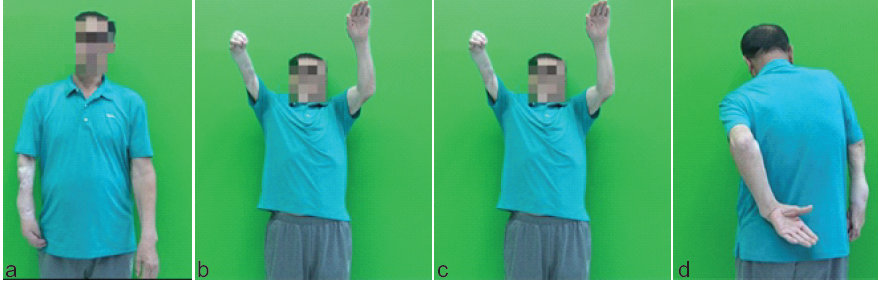
Figure 2: Pre-operative clinical photo of one-arm patient with anterosuperior irreparable rotator cuff tears. (a) A left one-arm patient due to a burn injury of the right arm. The patient exhibits loss of active forward elevation (b), abduction (c), and internal rotation (d).
Totally three one-arm patients were treated with aLDTM tendon transfer for ASIRCTs. The mean age was 55.3 ± 2.1 years old, and all patients were male two patients had paralytic limb weakness due to brachial plexus injury and one patient had a one-arm weakness due to burn injury. Mean follow-up periods were 32.0 ± 6.0 months. The demographic characteristics are described in Table 1.
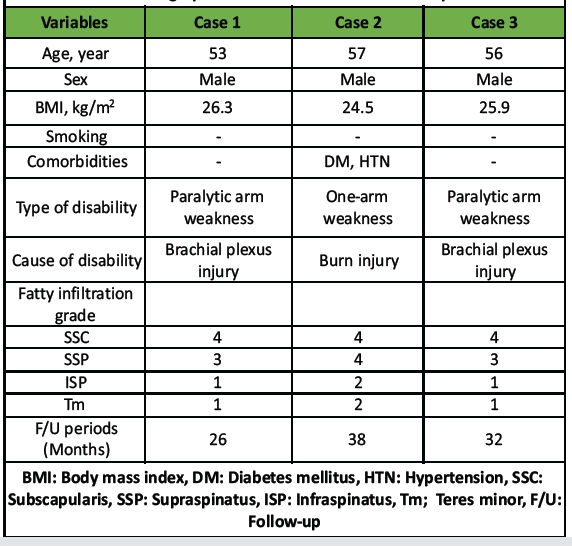
Table 1: Demographic and clinical characteristics of patients
The detailed surgical techniques for aLDTM tendon transfer have been previously described in our earlier publications [6]. Patients were positioned in the beach chair posture under general anesthesia for the surgical procedure. On intraoperative confirmation of ASIRCTs, the latissimus dorsi (LD) and teres major (TM) tendons were harvested. A skin incision was made along the deltopectoral interval, extending from the coracoid process to the inferior border of the pectoralis major. The LD and TM tendons were detached together from their humeral insertion using a periosteal technique, without attempting to separate the two tendons individually. To allow for adequate mobilization and excursion of the combined tendon unit, the surrounding adhesions were carefully released in a blunt fashion. A triple-loaded suture anchor was inserted approximately 2–3 cm distal to the greater tuberosity (GT), lateral to the bicipital groove. Using a 16G spinal needle, the six sutures from the anchor were passed through the tendon ends of the harvested LD and TM. With the shoulder positioned in full IR and approximately 45° of abduction (ABD), the sutures were tied to maintain appropriate physiological tension. The combined LDTM tendon was then fixed just lateral to the bicipital groove and distal to the lateral aspect of the GT using three lateral anchors. This placement allowed for a diagonal and tensioned positioning of the transferred tendon while minimizing the risk of axillary nerve compression (Fig. 3).
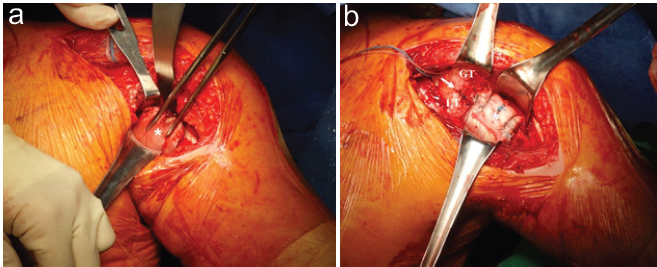
Figure 3: Intraoperative photo of combined anterior latissimus dorsi and teres major tendon transfer. (a) The latissimus dorsi (LD) and teres major (TM) tendons (asterisk) are shown after release of the pectoralis major tendon (δ). (b) The combined LDTM tendon (asterisk) was fixed just lateral to the biceps groove (arrow) and distal to the lateral edge of the GT using three lateral anchors. LT, lesser tuberosity; GT, greater tuberosity
Postoperatively, patients were immobilized with an ABD brace for 6 weeks. During this phase, only scapular stabilization exercises and passive range of motion (ROM) were permitted. From week 7 onward, active ROM exercises in all planes were initiated. At 3 months post-surgery, patients advanced to full ROM and commenced gentle strengthening exercises. At the 2 years postoperatively, all patients showed improvement in clinical outcomes including visual analog scale (VAS) score for shoulder pain, patients reported outcome measurement (PROM), active ROM (aROM), and aROM strength. The post-operative VAS score (1.6 ± 0.6) was significantly improved compared to preoperative VAS score (6.3 ± 0.6) (P < 0.001). The single assessment numeric evaluation score (44.0 ± 5.6 to 70.7 ± 2.5, P < 0.001), American shoulder and elbow surgeons score (44.3 ± 1.5 to 70.7 ± 2.5, P < 0.001), and University of California, Los Angeles score (16.3 ± 0.6 to 25.3 ± 1.5, P < 0.001) showed significant improvement after operation. Among the aROM, forward elevation ([FE] 90.0 ± 10.0 to 156.7 ± 5.8, P < 0.001), ABD 96.7 ± 5.8 to 133.3 ± 5.8, P < 0.001), and (IR 2.7 ± 1.2 to 8.0 ± 0.0, P < 0.001) also showed significant improvement after operation (Fig. 4).
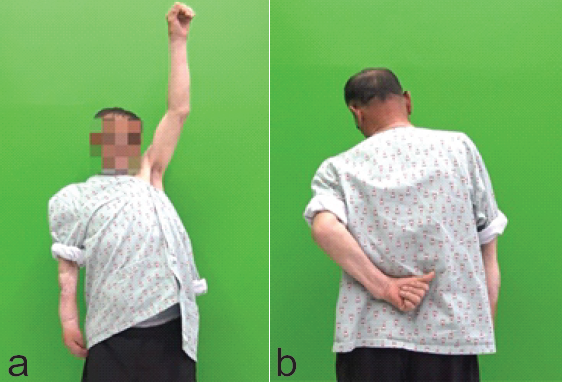
Figure 4: (a and b) Post-operative clinical photo of one-arm patient after combined anterior latissimus dorsi and teres major tendon transfer. The patient shows recovery of forward elevation and internal rotation.
The aROM strength was measured using a standard barometer by applying resistance to the movement and recording the force exerted at a specific joint angle (90° FE, 90° ABD, neutral IR, and neutral ER). The FE strength (16.1 ± 2.2 to 25.7 ± 1.1, P < 0.001), ABD strength (13.5 ± 1.1 to 25.9 ± 1.6, P < 0.001), and IR strength (16.1 ± 3.1 to 27.5 ± 3.4, P < 0.001) showed significant improvement after operation. As a radiologic outcome, the acromiohumeral distance and Hamada grade showed no changes before and after operation (Table 2).
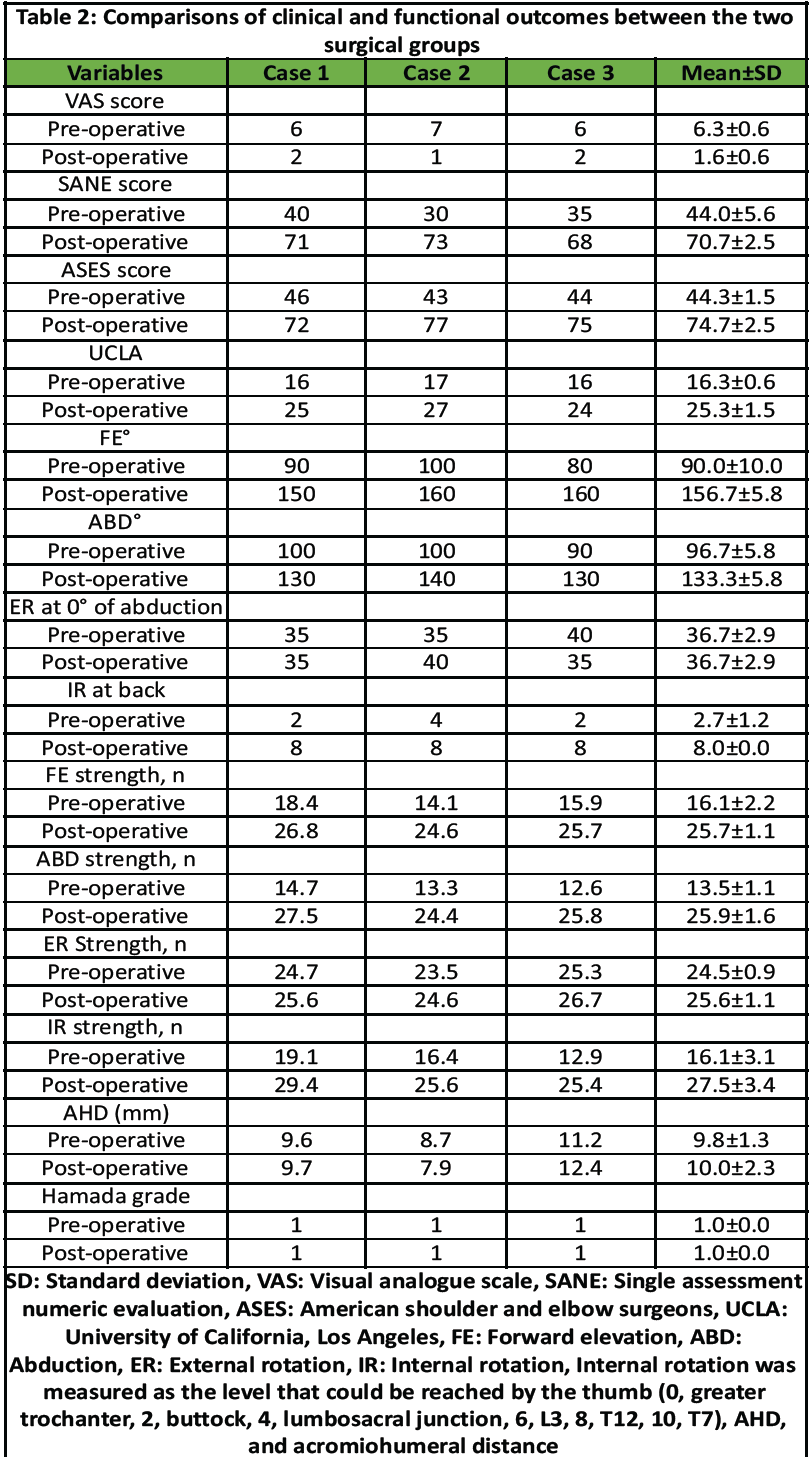
Table 2: Comparisons of clinical and functional outcomes between the two surgical groups
In all three patients, 2-year post-operative MRIs confirmed that the grafts remained intact without any retear (Fig. 5). There was no post-operative complication. All clinical outcomes were objectively assessed by a research coordinator who blinded the patient’s information and the details of this study.
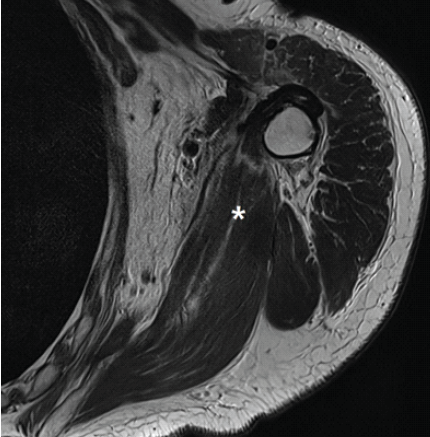
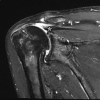
Figure 5: Post-operative magnetic resonance imaging (MRI) of combined anterior latissimus dorsi and teres major tendon transfer of the left shoulder A post-operative T2-weighted oblique coronal image of the MRI shows the transferred tendons (asterisk).
To the best of our knowledge, this case report is the first study to evaluate the efficacy and safety of aLDTM tendon transfer in one-arm patients with ASIRCTs without arthritic change. In this case repost, all three patients showed improvement in clinical outcomes including VAS score, PROMs, aROM, and aROM strength without progression of arthritis or any complications. Based on these results, it has been confirmed that aLDTM tendon transfer is an effective and safe treatment option for ASIRCTs without arthritic change in one-arm patients. One-arm patients with contralateral upper arm extremity amputation or complete palsy rely entirely on their remaining functional arm for performing basic activities of daily living [1]. The shoulder problems can significantly impact daily functioning and compromise their ability to remain independent [8]. This level of dependence on one functional upper extremity can lead to overuse injuries, such as rotator cuff tears, and eventually result in degenerative joint disease over time [9]. This may lead to the need for shoulder surgery in one-arm patients [1]. However, performing shoulder surgery in these patients poses unique challenges, including potential limitations in daily functioning and increased reliance on others during the post-operative rehabilitation phase [1]. In addition, the surgically treated shoulder may be exposed to a higher risk of complications due to post-operative overload and repetitive use [1]. Ultimately, these concerns – along with the limited data on surgical outcomes in this population – make the decision to proceed with surgery particularly complex for one-arm patients. Limited evidence exists on the outcomes of shoulder surgery in one-arm patients. Only one small case series reported the clinical outcomes and complications of RSA in one-arm patients [1]. In this study, five one-arm patients with cuff tear arthropathy (CTA) underwent RSA and showed significant improvement in pain, PROM, and aROM with no post-operative complications. They demonstrate that the RSA may be a safe and effective treatment for one-arm patients with CTA [1]. However, no studies have investigated joint-preserving treatments in one-arm patients with massive irreparable rotator cuff tears. Therefore, this study is the first to report the clinical outcomes and safety of aLDTM tendon transfer in one-arm patients with ASIRCTs. aLDTM tendon transfer has emerged as an effective joint-preserving surgical option for treating ASIRCTs, particularly in cases where conventional rotator cuff repair is not possible, such as in patients with functional limitation of the contralateral limb [6]. This procedure has demonstrated notable clinical efficacy, including substantial pain reduction and functional improvement, especially in IR [6]. The favorable clinical outcomes are thought to be attributed to the biomechanical advantages of the combined tendon transfer [7,10]. The transferred LD and TM muscles act synergistically to restore shoulder stability by reinforcing superior support and providing a compensatory mechanism for deficient posterior cuff function [7]. This restoration of balanced muscle forces across both the coronal and transverse planes likely contributes to improved joint centering and dynamic stabilization [7]. Given these biomechanical and clinical benefits, aLDTM tendon transfer offers a promising joint-preserving alternative for managing ASIRCTs, particularly in one-arm patients. This report has several inherent limitations due to its case-report design. First, the study included only three one-arm patients, precluding statistical analysis and generalization of findings. However, this limitation is unavoidable given the extreme rarity of the condition. Second, the follow-up duration (mean, 32 months) was insufficient to assess long-term graft durability and late degenerative changes. Third, post-operative imaging was limited to MRI integrity without dynamic evaluation of tendon healing or muscle activation. Finally, individualized rehabilitation strategies, observer bias, and socioeconomic burden were not assessed. Despite these limitations, this case report provides valuable preliminary evidence supporting the feasibility and safety of combined aLDTM tendon transfer as a joint-preserving surgical option for ASIRCTs in one-arm patients – a population in which such cases are exceedingly rare.
This case report is the first study to evaluate the efficacy and safety of aLDTM tendon transfer in one-arm patients with ASIRCTs. In this case report, all three patients showed improvement in clinical outcomes without progression of arthritis or any complications. Based on these results, it has been confirmed that aLDTM tendon transfer is an effective and safe treatment option for ASIRCTs in one-arm patients.
Combined anterior latissimus dorsi and teres major (aLDTM) tendon transfer is an effective and safe joint preserving treatment option for anterosuperior irreparable rotator cuff tears (ASIRCTs) in one-arm patients.
References
- 1. Alentorn-Geli E, Wanderman NR, Assenmacher AT, Elhassan BT, Sánchez-Sotelo J, Cofield RH, et al. Reverse shoulder arthroplasty in patients with amputation or paralysis of the contralateral upper extremity (one-arm patients). PM R 2017;9:1006-12. [Google Scholar] [PubMed]
- 2. Werthel JD, Walch G, Vegehan E, Deransart P, Sanchez-Sotelo J, Valenti P. Lateralization in reverse shoulder arthroplasty: A descriptive analysis of different implants in current practice. Int Orthop 2019;43:2349-60. [Google Scholar] [PubMed]
- 3. Berth A, Neumann W, Awiszus F, Pap G. Massive rotator cuff tears: Functional outcome after debridement or arthroscopic partial repair. J Orthop Traumato 2010;11:13-20. [Google Scholar] [PubMed]
- 4. Kany J, Guinand R, Croutzet P, Valenti P, Werthel JD, Grimberg J. Arthroscopic-assisted latissimus dorsi transfer for subscapularis deficiency. Eur J Ortho Surg Traumatol 2016;26:329-34. [Google Scholar] [PubMed]
- 5. Koh KH, Han KY, Yoon YC, Lee SW, Yoo JC. True anteroposterior (Grashey) view as a screening radiograph for further imaging study in rotator cuff tear. J Shoulder Elbow Surg 2013;22:901-7. [Google Scholar] [PubMed]
- 6. Baek CH, Kim JG, Baek GR. Outcomes of combined anterior latissimus dorsi and teres major tendon transfer for irreparable anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2022;31:2298-307. [Google Scholar] [PubMed]
- 7. Baek GR, Kim JG, Kwak D, Nakla AP, Chung MS, McGarry MH, et al. Biomechanical comparison of combined latissimus dorsi and teres major tendon transfer vs. Latissimus dorsi tendon transfer in shoulders with irreparable anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2023;32:703-12. [Google Scholar] [PubMed]
- 8. Garreau De Loubresse C, Norton MR, Piriou P, Walch G. Replacement arthroplasty in the weight-bearing shoulder of paraplegic patients. J Shoulder Elbow Surg 2004;13:369-72. [Google Scholar] [PubMed]
- 9. Kim SC, Kim HG, Rhee YG, Rhee SM, Cho CH, Kim DH, et al. Surgical outcomes of weight-bearing shoulders: Arthroscopic rotator cuff repair and reverse shoulder arthroplasty. Clin Orthop Surg 2025;17:438-52. [Google Scholar] [PubMed]
- 10. Baek CH, Lim CM, Kim JG, Kim BT, Kim SJ. Efficacy of combined anterior latissimus dorsi and teres major tendon transfer vs. Reverse total shoulder arthroplasty in anterosuperior irreparable rotator cuff tears with loss of active internal rotation. J Shoulder Elbow Surg 2025;34:e866-78. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Dual Reconstruction, Combined Anterior Latissimus Dorsi with Teres Major and Middle Trapezius Tendon Transfer, Reduces Anterior Superior Humeral Subluxation: Case Report
January 1, 2026 Dual Reconstruction, Combined Anterior Latissimus Dorsi with Teres Major and Middle Trapezius Tendon Transfer, Reduces Anterior Superior Humeral Subluxation: Case Report April 7, 2014 Subdeltoid Bursa Tuberculosis with Rice Bodies Formation: Case Report and Review of Literature
April 7, 2014 Subdeltoid Bursa Tuberculosis with Rice Bodies Formation: Case Report and Review of Literature May 10, 2022 Severe Normal Pressure Hydrocephalus Symptom Caused by Rheumatoid Arthritis-induced Atlantoaxial Subluxation: A Case Report
May 10, 2022 Severe Normal Pressure Hydrocephalus Symptom Caused by Rheumatoid Arthritis-induced Atlantoaxial Subluxation: A Case Report September 9, 2018 Painful Nonunion after Missed Juvenile Tillaux Fracture in an Athlete – Case Report and Description of a New Fixation Technique
September 9, 2018 Painful Nonunion after Missed Juvenile Tillaux Fracture in an Athlete – Case Report and Description of a New Fixation Technique