
An extended application of a lag screw as a reduction technique in Neer Type V distal clavicle fractures utilizes fundamental trauma principles to offer a simple alternative technique to achieve direct anatomical reduction of the inferior fracture fragment in a stable plate-screw construct without the need for extensive soft-tissue dissection.
Dr. Shaun Kai Kiat Chua, Department of Orthopedic Surgery, Tan Tock Seng Hospital, Singapore. E-mail: shaunkkchua@gmail.com
Abstract
Introduction: Neer Type V distal clavicle fractures are an unstable fracture configuration that is often treated with surgery. Type V fractures are challenging as the integrity of the coracoclavicular ligament needs to be restored by reducing the inferior fragment – a technically challenging endeavor. Multiple heterogeneous surgical techniques have been proposed in the literature to treat unstable distal clavicle fractures without any consensus on best practice. To date, there remains a lack of described effective techniques to aid in reducing the inferior fracture fragment in Neer Type V distal clavicle fractures.
Case Report: We employ a novel method of applying a lag screw technique to aid in the reduction of the inferior fragment to solve this notoriously challenging fracture pattern.
Conclusion: This novel technique builds on fundamental trauma concepts. The extended use of a lag screw as a reduction technique in distal clavicle fractures has not been described in the literature before. This reduction technique reduces the need for extensive soft-tissue dissection for coracoid exposure, as described in other techniques (e.g., suture anchor or button fixations), while enabling direct incorporation of the inferior fragment, bone-to-bone healing, and benefits from the stability of a plate-screw construct.
Keywords: Clavicle fracture, distal, type V, Neer, reduction, lag screw, technique.
Neer Type V distal clavicle fractures are unstable fractures that are notoriously challenging to fix. Type V fractures are described by Neer as an unstable fracture pattern with an inferior clavicle fragment attached to the coracoclavicular ligament [1]. Due to the forces acting on the distal clavicle, high rates of malunion and non-union are associated with Type II and Type V fractures [2]. Non-union rates in non-surgical management of distal clavicle fractures have been reported to be as high as a third of cases [3].
Multiple techniques have been proposed in literature without any consensus on best practice to date [3,4,5]. Often, indirect techniques are employed to incorporate the reduction of the inferior fragment (clavicle fragment to which the coracoclavicular ligament remains attached) in a Type V fracture [3,4,5].
The authors aim to share a novel use of the lag screw technique to aid in the reduction of a Neer Type V distal clavicle fracture.
A 33-year-old right-handed male motorcyclist with a background of impaired fasting glucose on diet control was brought into the emergency department after a road traffic accident. The patient was travelling between 60 and 70 km/h along an expressway when the vehicle ahead braked suddenly. This resulted in the patient crashing into the rear of the vehicle and landing onto his right shoulder. In the emergency room, the patient complained of right shoulder pain with a deformity noted over the lateral aspect of the right shoulder without any overlying skin defect. A Neer Type V distal clavicle fracture was noted after dedicated clavicle radiographs were performed (Fig. 1). The patient was counseled and consented to the surgical fixation of his right distal clavicle.
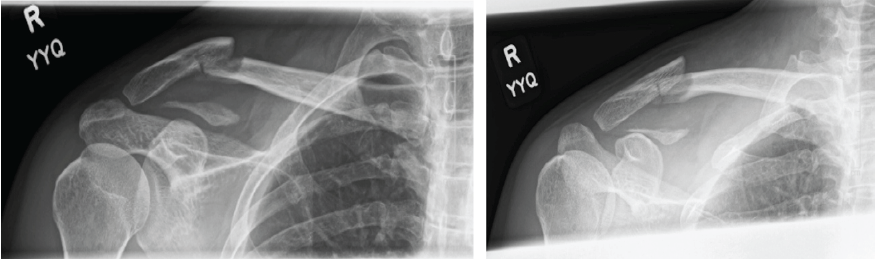
Figure 1: Pre-operative radiographic imaging of right Neer Type V distal clavicle fracture.
Surgical technique
The described technique was performed on a patient who sustained a right Neer Type V distal clavicle fracture confirmed on dedicated clavicle radiographs (Fig. 1). Under general anesthesia, the patient was positioned in a beach chair at 90°. A superior approach was utilized with an incision centered over the fracture. The fracture was exposed and freshened with care to avoid excessive stripping off the surrounding soft tissues. The distal and proximal fracture fragments were reduced with the aid of bone reduction clamps. A distal clavicle 7-hole 3.5 mm locking-compression plate (Superior Clavicle Plate, DePuy Synthes, Indiana, United States) was applied and held with the aid of Kirshner wires and screws (Fig. 2).
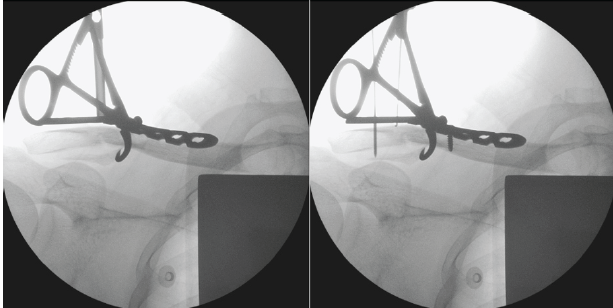
Figure 2: Initial reduction of distal and proximal fracture fragments with bone reduction clamps and locking-compression plate.
Further dissection was employed to retrieve the inferior fragment with the coracoid ligament attached. The reduction lag screw technique was employed to aid in the reduction of the inferior fragment. A 3.5 mm drill was used for the gliding hole created at the cortical screw hole of the plate – overlying the inferior fragment. A pilot hole was drilled through the inferior fragment using a 2.5 mm drill. An initial 3.5 mm cortical screw was applied to engage the inferior fragment (pilot hole). As the lag-screw was advanced, the inferior fragment was reduced toward the main clavicle fragments (Fig. 3). The reduction of the inferior fragment was then reinforced by tying cerclage braided sutures around the main clavicle fragment.
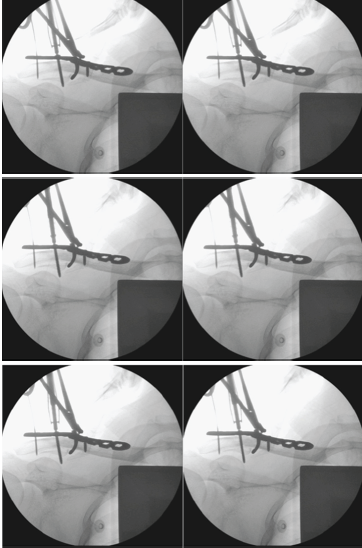
Figure 3: Reduction of the inferior fracture fragment using the lag screw technique.
Once the plate has been securely applied and the remaining screw holes secured, the 3.5 mm cortical screw was then replaced with an appropriately sized cortical screw (holding screw) that engages the inferior fragment (Figs. 4 and 5).
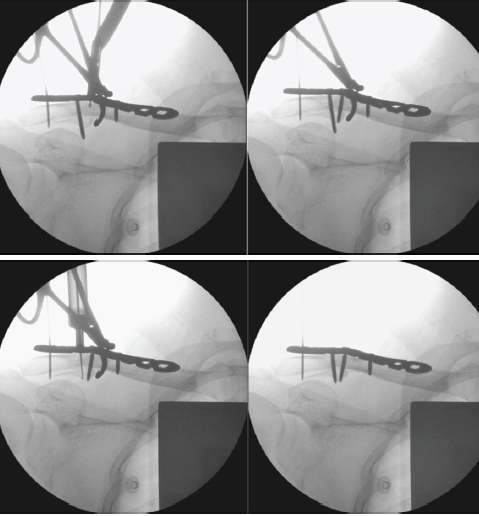
Figure 4: Replacement of a 3.5 mm cortical screw with an appropriately sized holding screw.
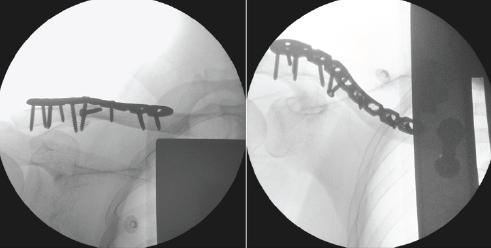
Figure 5: Final plate and screws placement engaging the inferior fragment.
Post-operative care
Postoperatively, the patient’s operated upper limb was kept on an arm sling and non-weight bearing for a total of 4 weeks. Pendular exercises to the operated arm were allowed.
Post-operative outcome
The patient was discharged on the same day and was reviewed in the specialist outpatient setting, with good wound healing noted at 2 weeks postoperatively. The patient returned to work after 4 weeks and was able to achieve abduction and forward flexion of 160° at subsequent follow-up. At 6 months, the patient had no complaints of pain and was subsequently discharged from follow-up. A phone consult was held 2 years postoperatively, with the patient noting the absence of any pain, hardware irritation, or functional limitation of his right upper limb.
The surgical management of Type V fracture is varied, with multiple treatment modalities proposed. The incorporation of the inferior fragment (clavicle fragment that is attached to the coracoclavicular ligament) remains challenging. The authors demonstrated a novel reduction technique employing lag screw principles to aid in the reduction of the clavicle with the inferior clavicle fragment. This reduction directly incorporates the inferior fragment, enables bone-to-bone healing, and benefits from the stability of a plate-screw construct. The patient was able to undergo early mobilization and healed well without complications.
Most techniques to date achieve reduction in an indirect fashion. Suture anchor or button fixations utilize the coracoid as an anchor to aid in reduction. The inferior fragment is often secured to the main distal and lateral fragments using strong cerclage sutures to enable bone-to-bone healing [6,7]. However, extensive soft-tissue dissection is required to enable adequate exposure of the coracoid, with extra caution taken to avoid injury to the medial neurovascular structures. In Christensen et al.’s technique, releases of the coracoacromial ligament as well as structures medially were required to allow adequate visualization of the coracoid [7].
Hook plates similarly reduce unstable Type V fractures indirectly by anchoring itself to the acromion. Further techniques are required to secure the inferior fragment. Complications from hook clavicle plates often require subsequent removal to avoid fracture or osteolysis of the medial acromion [6,8,9].
Boonard et al., through a meta-analysis, recommended plate and screw fixations as a first-line technique for unstable distal clavicle fractures. Although the studies included in the analysis did not involve Type V fractures, plate and screw fixations resulted in higher UCLA scores and significantly lower complications [5]. Plate fixations are often limited by inadequate distal fragment purchase. Modern clavicle plates with lateral extension plates allow multiple locking screw purchases in the limited distal fragment [10]. Modern plate designs further aid in the reduction and fixation of unstable distal clavicle fractures. Osteosynthesis using a scorpion plate in Type V fractures yielded favorable outcomes in a series reported by Furuhata et al. [11]. The presence of a plate and screw fixation allows for a stable scaffold for further reduction techniques to be employed – like the technique described in this report.
There are technical challenges with a lag screw reduction technique. Due to the variable size of the inferior fragment, its incorporation when performing the lag screw fixation may lead to its fragmentation. Similarly, eccentric drilling of the coracoid may result in a cutout during reduction. The use of the 3.5 mm screw requires protection with a Hoffmann retractor placed under the coracoid to avoid injury to structures inferior to the coracoid. In addition, the bone-screw purchase may be lost during the removal of the larger-sized reduction lag-screw in exchange for a holding screw of an appropriate length.
The literature on unstable distal clavicle fractures remains heterogeneous without any consensus on best practice [7]. The authors hope that this novel reduction technique can contribute to the diverse literature available.
Limitations and future directions
This was a single case report and technique description, which could inherently affect the generalizability of results. Further higher-powered clinical studies with longer clinical and radiographical follow-up are needed to validate the outcomes of this novel technique.
This novel technique builds on fundamental trauma concepts. The extended use of a lag screw as a reduction technique has not been described in the literature before. Further studies are required to validate the results of this novel case report.
This novel technique, using a lag screw technique to aid in the reduction of the inferior fragment in Neer Type V distal clavicle fractures, allows direct anatomical reduction of the inferior fracture fragment in a stable plate-screw construct without the need for extensive soft-tissue dissection.
References
- 1. Neer CS 2nd. Fractures of the distal third of the clavicle. Clin Orthop Relat Res 1968;58:43-50. [Google Scholar] [PubMed]
- 2. Stenson J, Baker W. Classifications in brief: The modified neer classification for distal-third clavicle fractures. Clin Orthop Relat Res 2021;479:205-9. [Google Scholar] [PubMed]
- 3. Oh JH, Kim SH, Lee JH, Shin SH, Gong HS. Treatment of distal clavicle fracture: A systematic review of treatment modalities in 425 fractures. Arch Orthop Trauma Surg 2011;131:525-33. [Google Scholar] [PubMed]
- 4. Kim DW, Kim DH, Kim BS, Cho CH. Current concepts for classification and treatment of distal clavicle fractures. Clin Orthop Surg 2020;12:135-44. [Google Scholar] [PubMed]
- 5. Boonard M, Sumanont S, Arirachakaran A, Sikarinkul E, Ratanapongpean P, Kanchanatawan W, et al. Fixation method for treatment of unstable distal clavicle fracture: Systematic review and network meta-analysis. Eur J Orthop Surg Traumatol 2018;28:1065-78. [Google Scholar] [PubMed]
- 6. Chen CY, Yang SW, Lin KY, Lin KC, Tarng YW, Renn JH, et al. Comparison of single coracoclavicular suture fixation and hook plate for the treatment of acute unstable distal clavicle fractures. J Orthop Surg Res 2014;9:42. [Google Scholar] [PubMed]
- 7. Christensen GV, Skalitzky MK, Bozoghlian MF, Lane CM, Nepola JV, Patterson BM, et al. Suture button fixation and nice knot cerclage for neer type V distal clavicle fractures. Arthrosc Tech 2025;14:103452. [Google Scholar] [PubMed]
- 8. Tiren D, Van Bemmel AJ, Swank DJ, Van Der Linden FM. Hook plate fixation of acute displaced lateral clavicle fractures: Mid-term results and a brief literature overview. J Orthop Surg Res 2012;7:2. [Google Scholar] [PubMed]
- 9. Kashii M, Inui H, Yamamoto K. Surgical treatment of distal clavicle fractures using the clavicular hook plate. Clin Orthop Relat Res 2006;447:158-64. [Google Scholar] [PubMed]
- 10. Ochen Y, Frima H, Houwert RM, Heng M, Van Heijl M, Verleisdonk EJ, et al. Surgical treatment of neer type II and type V lateral clavicular fractures: Comparison of hook plate versus superior plate with lateral extension: A retrospective cohort study. Eur J Orthop Surg Traumatol 2019;29:989-97. [Google Scholar] [PubMed]
- 11. Furuhata R, Matsumura N, Kamata Y, Tanji A. Osteosynthesis using Scorpion plate for neer type V distal clavicle fracture. BMC Musculoskelet Disord 2024;25:909. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 “No Traction” Technique: A Novel, Simple, Easy, and Ergonomic Manoeuvre to Reduce Posterior Dislocation of the Hip Joint – A Case Report
May 1, 2026 “No Traction” Technique: A Novel, Simple, Easy, and Ergonomic Manoeuvre to Reduce Posterior Dislocation of the Hip Joint – A Case Report July 1, 2026 Chronic Acromioclavicular Joint Instability: Outcomes after Stabilization without Tendon Graft Augmentation
July 1, 2026 Chronic Acromioclavicular Joint Instability: Outcomes after Stabilization without Tendon Graft Augmentation June 1, 2026 Delayed Pseudoaneurysm of the Subclavian Artery Following Clavicle Fracture Fixation: A Case Report
June 1, 2026 Delayed Pseudoaneurysm of the Subclavian Artery Following Clavicle Fracture Fixation: A Case Report October 1, 2025 Evaluation of Combined Use of Pre-contoured Locking Distal Clavicle Plate and Tunneled Suspensory Device Fixation for Unstable Lateral End Clavicle Fracture
October 1, 2025 Evaluation of Combined Use of Pre-contoured Locking Distal Clavicle Plate and Tunneled Suspensory Device Fixation for Unstable Lateral End Clavicle Fracture