
Stacked Flexible Nailing done for midshaft radius ulna fractures in adults seems a good minimally invasive surgical option with no postoperative immobilisation, early rehabilitation and excellent functional outcome.
Dr Qaedjohar Dhariwala
Inamdar Hospital, Fatima Nagar, Pune , India.
E-mail: qaedjohar@gmail.com
Abstract
Introduction: Simultaneous radius and ulna fractures are common in adults and generally osteosynthesis with plating is the treatment of choice. Nailing of such fractures is infrequently advocated. We present our unique technique of radius ulna nailing in adults to achieve closed reduction and early predictable union with minimal or no complications.
Case Report: Case 1: 22 year old male with midshaft both bones forearm fracture was treated with stacked nailing. Two 2.5 mm steel elastic nails were used in each radius and ulna. No post-operative splintage was needed and patient was mobilized immediately. Patient was able to go back to work in 2 weeks and at one year follow up he showed excellent functional outcome. Case 2: Fifteen year old boy presented with midshaft both bone fractures secondary to fall from height. He was also treated with stacked flexible nailing. Good stability was achieved and patient was mobilized immediately without any splints. He was able to write his exams which started on 11th day post-surgery and could complete his theory papers. At final follow up both bones united with good callus and no functional limitations.
Conclusion: Stacked nailing technique is a good option in midshaft transverse or short oblique fractures of radius and ulna. It allows for early mobilization without brace or splint. With proper patient selection, good results can be obtained by this simple and minimally invasive technique.
Keywords: Radius Ulna Fracture, stacked nailing, closed reduction.
The both bone forearm (radius and ulna) fractures in paediatric population can be satisfactorily treated commonly by simple immobilsation or closed nailing [1-4] but in adolescent and adult population open plating is preferred than nailing [1-7]. The goal of treatment of both bone forearm fracture is to achieve both axial and rotational stability irrespective of age, modality or implant [8]. In adults, the standard treatment for such fractures is open reduction and internal fixation with plating because of risk of malunion [9]. There are numerous studies supporting osteosynthesis for such fractures [9] [10] though these describe the well known complications like soft tissue damage, malunion and non-union as well [9]. Early reports of intramedullary nailing in forearm fractures reported unsatisfactory results due to lack of rotational stability [11,12]. Interlocking intramedullary nailing were introduced and they too offer good results comparable to plating [13]. We treated two cases of both bone forearm fractures using technique of stacked intramedullary nailing using multiple flexible nails and report the clinical and functional outcome.
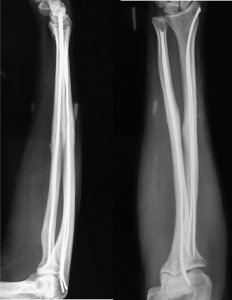
Case 1: Twenty two years old male who sustained closed fracture of midshaft of both bones of forearm due to a fall from motorcycle (Fig. 1).

Patient was taken up for surgery the next day under regional block after proper preanaesthetic check up. In our technique, a transverse incision was made over radial styloid along Langer’s lines. Care was taken to protect the sensory branch of radial nerve and thumb tendons. Entry point was created with awl or 3.2 mm drill bit making it big enough to allow passage of two nails. Tip of flexible nail was pre-bent into a gentle curve. Nail was inserted into radial canal manually with a T handle. Insertion typically encounters resistance every few centimeters. Resistance can be overcome by minimally rotating the nail. Nail was passed up to fracture site. Closed reduction was achieved using C arm. Nail was passed across fracture site but not completely so as to allow manipulation for reduction of ulna fracture. For ulna, entry point was made on the radial aspect of ulnar shaft near olecranon (eccentric). A prebent nail was inserted in to the ulnar canal up to fracture site. Closed reduction was achieved and the nail was passed across up to ulnar head. Similarly radial nail was passed up to radial head. One more additional nail was passed in both radius and ulna (2 in radius and 2 nails in ulna). The nails were cut flush with bone. Reduction was found to be stable on table during prono-supination movements (Fig. 2). No immobilization was given post-surgery and physiotherapy was started the next day and patient was comfortably performing prono-supination from third day post-surgery (Fig. 3).

Patient was followed up at 2 weeks, 6 weeks, 3 months, 6 months and 1 year. Patient had minimal pain post operatively and achieved full prono-supination and wrist and elbow range of movements by 2 weeks. He was able to return to his computer work in 2 weeks. Callus was seen by 3 months and fractures were completely united by 6 months (Fig. 4). At one year follow up the bone showed good union and functionally patient was able to do all activities (Fig. 5).
Case 2: Fifteen year old boy presented to with midshaft left radius ulna fracture secondary to fall from height. He had his board exams in 10 days and parents were very apprehensive about him writing his exams. Multiple stack nailing was done using 2.5 mm steel elastic nails (Fig. 6). Post operatively patient was allowed mobilization from second day and at 10 days follow up he was able to hold his pen and write (Video 1). He was able to write his exams which started 11th day after surgery and could complete all his papers. Follow up at 6 weeks showed good callus and patient was fully functional (Fig. 6b).

The primary goal of treatment is stable fixation and early mobilization. Two most common interventions used for displaced both bone forearm fractures are osteosynthesis with plating and closed/open reduction with nail fixation [1,4]. Historically, Schone in 1913 described closed intramedullary nailing technique [7]. Though open reduction and internal fixation with plating is treatment of choice for both bone forearm fractures since Second World War [7]. Plating is more logical to most of the orthopaedic surgeons as it restores radial bow [1]. Flexible nailing in adults was criticized to have unsatisfactory result due to lack of rotational stability and also need for a cast or brace after surgery [11,12]. In the technique of stacked nailing, both these issues are resolved. Due to stacking of multiple nails the construct fills in the medullary cavity and provides excellent rotational stability and this also eliminates need for a cast or brace. The flexible nature of the nails allows for restoration of the radial bow and interosseous space. This was evident by good prono-supination achieved by the patient at 2 weeks post-surgery. It was amazing to see the second patient write comfortably at 10 days post-surgery and able to complete his examinations. Being flexible, the nails do allow some motion at the fracture site, thus promoting secondary callus formation and healing. Interlocking intramedullary radius ulna nailing also achieve the same effect by using the interlocking bolts. These interlocking nails have shown to achieve good results, with better cosmesis and early motion [8-11,14]. However these nails are expensive as compared to simple flexible steel nails and probably technically more demanding. Use of multiple stacked nailing was first described in German literature by Hackethal in 1961 [15]. He used 3mm rigid nails to stack the medullary cavity of various bones including humerus, tibia and also both bone forearm fractures. The procedure was technically difficult due to use of rigid nails of same size, but later authors reported use of flexible nails of varying diameter to simplify the procedure [16]. Most reports are in German literature and English language literature has reported the use of stacked nailing for humerus fractures only [16,17,18,19]. From experience of stacked nailing in humerus fractures it is reported to be best indicated for transverse or short oblique fractures of middle third of humerus and extending the indications may lead to high incidence of non-unions [18,20]. Same can be extrapolated to radius ulna fractures and in our opinion, technique is good for mid shaft radius ulna fractures which are transverse of short oblique. Galleazi and Monteggia fracture dislocations are contraindications as they require perfect anatomical reduction and rigid fixation. Distal 4th radius fractures or proximal 4th ulna fractures are also relative contraindications as the fractures are too close to the entry point of the nail and reduction would be difficult. The advantage of the technique is that the fixation is rotationally stable allowing immediate postoperative mobilization and as the nails are elastic, the normal bowing of the bones is restored. Due to minimal soft tissue trauma, post-operative pain is less and rehabilitation is easy. The core principle is to stack multiple flexible nails. The multiple nails fill up the canal and provide the necessary rotational stability. Also these provide for some movement along the fracture site, thus stimulating osteogenesis and callus formation. In our technique, the anticipated problems are bending of the nails at the fracture site if the patient has a fall before fracture union and for this we recommend patients to use an elbow pouch when they are up and about. The second problem is implant removal is difficult as the nails are cut flush at entry point. We don’t consider this as a major disadvantage as most authorities do not recommend removal of forearm plates either. Also in case there is refracture, we believe the nails can be removed through the fracture site. Some authors have reported hypertrophic ossification at nail entry points when stacked nailing was used for humerus fractures [17]. We did not face this complication in our two cases and we think making a large enough entry point will help preventing this complication
Stacked Flexible nailing technique for radius ulna fracture in adults can be a viable and easier alternative to plating. We can confidently avoid plaster immobilisation after nailing. In our opinion it has definite advantages. Already study is underway in a larger group of patients. Results so far are very encouraging.
The authors would like to acknowledge Dr Hemant Patankar who introduced us to this technique
References
- 1. Vopat ML, Kane PM, Christino MA, Truntzer J, McClure P, Katarincic J, Vopat BG. Treatment of diaphyseal forearm fractures in children. Orthop Rev (Pavia). 2014 Jun 24;6(2):5325. [Google Scholar] [PubMed]
- 2. Sinikumpu JJ, Keränen J, Haltia AM, Serlo W, Merikanto J. A new mini-invasive technique in treating pediatric diaphyseal forearm fractures by bioabsorbable elastic stable intramedullary nailing: a preliminary technical report. Scand J Surg. 2013;102(4):258-64.. [Google Scholar] [PubMed]
- 3. Parajuli NP, Shrestha D, Dhoju D, Dhakal GR, Shrestha R, Sharma V. Intramedullary nailing for paediatric diaphyseal forearm bone fracture. Kathmandu Univ Med J (KUMJ). 2011 Jul-Sep;9(35):198-202.. [Google Scholar] [PubMed]
- 4. Truntzer J, Vopat ML, Kane PM, Christino MA, Katarincic J, Vopat BG. Forearm diaphyseal fractures in the adolescent population: treatment and management. Eur J Orthop Surg Traumatol. 2015 Feb;25(2):201-9. [Google Scholar] [PubMed]
- 5. Patel A, Li L, Anand A. Systematic review: functional outcomes and complications of intramedullary nailing versus plate fixation for both-bone diaphyseal forearm fractures in children. Injury. 2014 Aug;45(8):1135-43. [Google Scholar] [PubMed]
- 6. Durst A, Johal S, Chirodian N. An inexpensive alternative method in the [Google Scholar] [PubMed]
- 7. management of paediatric forearm fractures. Ann R Coll Surg Engl. 2014 May;96(4):319. [Google Scholar] [PubMed]
- 8. Bartoníček J, Kozánek M, Jupiter JB. History of operative treatment of forearm diaphyseal fractures. J Hand Surg Am. 2014 Feb;39(2):335-42. [Google Scholar] [PubMed]
- 9. Saka G, Saglam N, Kurtulmuş T, Avcı CC, Akpinar F, Kovaci H, Celik A. New interlocking intramedullary radius and ulna nails for treating forearm diaphyseal fractures in adults: a retrospective study. Injury. 2014 Jan;45 Suppl 1:S16-23. [Google Scholar] [PubMed]
- 10. Schulte LM, Meals CG, Neviaser RJ. Management of adult diaphyseal both-bone forearm fractures. J Am Acad Orthop Surg. 2014 Jul;22(7):437-46. [Google Scholar] [PubMed]
- 11. Köse A, Aydın A, Ezirmik N, Can CE, Topal M, Tipi T. Alternative treatment of forearm double fractures: new design intramedullary nail. Arch Orthop Trauma Surg. 2014 Oct;134(10):1387-96. [Google Scholar] [PubMed]
- 12. Knight RA, Purvis GD. Fractures of both bones of the forearm in adults. J Bone Joint Surg 1949;31A–4:755–764. [Google Scholar] [PubMed]
- 13. Sage FP. Medullary fixation of fractures of the forearm. A study of the medullary canal of the radius and a report of fifty fractures of the radius treated with a prebent triangular nail. J Bone Joint Surg 1959;41A:1489–1516. [Google Scholar] [PubMed]
- 14. Jones DB Jr, Kakar S. Adult diaphyseal forearm fractures: intramedullary nail versus plate fixation. J Hand Surg Am. 2011 Jul;36(7):1216-9. [Google Scholar] [PubMed]
- 15. Shah AS, Lesniak BP, Wolter TD, Caird MS, Farley FA, Vander Have KL. Stabilization of adolescent both-bone forearm fractures: a comparison of intramedullary nailing versus open reduction and internal fixation. J Orthop Trauma. 2010 Jul;24(7):440-7. [Google Scholar] [PubMed]
- 16. Hackethal KH (Ed). The bundle nailing. Experimental and Clinical Study on a Novel Method of Marksmanship (German Edition). Berlin, Springer Verlag. Page 149 [Google Scholar] [PubMed]
- 17. Durbin RA, Gottesman MJ, Saunders KC. Hackethal stacked nailing of humeral shaft fractures. Experience with 30 patients. Clin Orthop Relat Res. 1983 Oct;(179):168-74. [Google Scholar] [PubMed]
- 18. Henley MB, Chapman JR, Claudi BF. Closed retrograde Hackethal nail stabilization of humeral shaft fractures. J Orthop Trauma. 1992;6(1):18-24. [Google Scholar] [PubMed]
- 19. Obruba P, Kopp L, Edelmann K. [Treatment of humeral shaft fractures using Hackethal’s technique of intramedullary bundle nailing]. Acta Chir Orthop Traumatol Cech. 2012;79(4):341-6. [Google Scholar] [PubMed]
- 20. Margad O, Boukhris J, Sallahi H, Daoudi M, Azriouil O, Koulali K. [Role of Hackethal bundle nailing in the treatment of humerus fractures: about 80 cases]. Pan Afr Med J. 2016 Jul 19;24:253. [Google Scholar] [PubMed]
- 21. Obruba P, Rammelt S, Kopp L, Edelmann K, Avenarius J. Non-Unions After Fixation Of Humeral Fractures Using Hackethal’s Bundle Nailing Technique. Acta Ortop Bras. 2016 Sep-Oct;24(5):270-274.. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2024 Robotic-Assisted Total Knee Arthroplasty: Innovations, Precision, and the Future of Joint Reconstruction
December 1, 2024 Robotic-Assisted Total Knee Arthroplasty: Innovations, Precision, and the Future of Joint Reconstruction March 10, 2018 Arthroscopic Treatment of Concurrent Avulsion Fracture of Anterior and Posterior Cruciate Ligament with Suspension Device
March 10, 2018 Arthroscopic Treatment of Concurrent Avulsion Fracture of Anterior and Posterior Cruciate Ligament with Suspension Device May 1, 2025 Temporal Patterns of Trauma Mortality and Causes of Death in a Level 1 Trauma Center: Implications for Improved Trauma Care
May 1, 2025 Temporal Patterns of Trauma Mortality and Causes of Death in a Level 1 Trauma Center: Implications for Improved Trauma Care February 1, 2026 Pseudomeningocele Presenting with Neurological Symptoms 1 Year after Spinal Surgery: A Case Report
February 1, 2026 Pseudomeningocele Presenting with Neurological Symptoms 1 Year after Spinal Surgery: A Case Report