
A missed diagnosis of a bipolar clavicle fracture, especially the medial component, might lead to non-union or malunion, chronic pain, reduced shoulder function, neurovascular complications, post-traumatic arthritis, and cosmetic deformity. Hence, early recognition and optimal management are key to achieving better outcomes.
Dr. B Bidhu, Department of Orthopaedics, Travancore Medical College, Kollam, Kerala, India. E-mail: bidhubalan@gmail.com
Abstract
Introduction: Clavicle fractures are more common, accounts for about 2.6–4% of all fractures in adults. Of these, 69-82% are midshaft clavicle fractures, followed by lateral clavicle fractures, which accounts for 21–28% and medial clavicle fractures, which are the rarest one accounts for about 2–3%. Bipolar clavicle fractures are defined as lateral and medial end clavicle fractures, accounts for only 2–8% of all clavicle fractures.
Case Report: We present the case of a 61-year-old female, came with right shoulder pain and swelling following an alleged history of a fall. Initially managed as a lateral end clavicle fracture, further radiological evaluation revealed a bipolar clavicle fracture . Patient managed operatively with open reduction and internal fixation using locking plates and screws.
Discussion: A bipolar clavicle fracture is the result of direct trauma to the shoulder region, commonly following road traffic accidents. In elderly patients with osteoporotic bone, it has been reported to occur with trivial trauma. Due to the rarity of bipolar clavicle fracture, it’s often missed initially. Proper clinicoradiological evaluation with the aid of computed tomography scan is necessary. With the scarcity of proper treatment guidelines, bipolar clavicle fractures are mostly treated operatively.
Conclusion: Bipolar clavicle fractures are rare but require timely intervention for optimal recovery. Dual plating provides rigid fixation and favorable outcomes.
Keywords: Bipolar clavicle fracture, open reduction, internal fixation.
The clavicle is the first bone to begin ossification during embryologic development. It connects the axial skeleton to the appendicular skeleton. It’s a relatively thin bone, widest at its medial and lateral expansions, where it articulates with the sternum and acromion, respectively. One of the most often fractured bones in the human body is the clavicle. It can be as a result of direct contact or force transmission from falling onto an outstretched hand. Clavicular fracture accounts for around 2.6–4% of all fractures in adults [1]. Of these fractures, 69–82% are mid-shaft fractures, 21–28% are lateral clavicle fractures, and 2–3% are medial clavicle fractures [1,2,3,4]. Segmental clavicular fracture is a rare injury, which generally refers to a concomitant ipsilateral distal and midshaft clavicle fracture [5]. Bipolar clavicle fracture is even rarer, which involves the lateral and medial end clavicle, accounts for only 2–8% of all clavicle fractures [6,7]. Owing to the rarity of bipolar clavicle fractures, well-defined treatment guidelines for their management have not yet been established
A 61-year-old female was admitted with a history of a slip and fall, presented with pain and swelling over her right shoulder [Fig. 1].

Figure 1: Clinical picture of patient at presentation.
Clinical examination revealed gross swelling over the clavicle, tenderness along the right clavicle, and a restricted range of motion with no neurological deficit. Initially, thought of a lateral end clavicle fracture, stabilization was done by strapping, which aggravated the patient’s symptom and increased prominence over the medial end of the clavicle. Radiographic reassessment showed a medial and lateral end clavicle fracture [Fig. 2].

Figure 2: Pre-operative X-rays showing a bipolar clavicle fracture.
To assess any joint involvement, a computed tomography (CT) scan was done, which showed a comminuted, mildly displaced intraarticular fracture in the medial 1/3rd of the right clavicle and displaced oblique fractures in the lateral 1/3rd of the right clavicle with an intact acromioclavicular joint and sternoclavicular joint [Fig. 3].
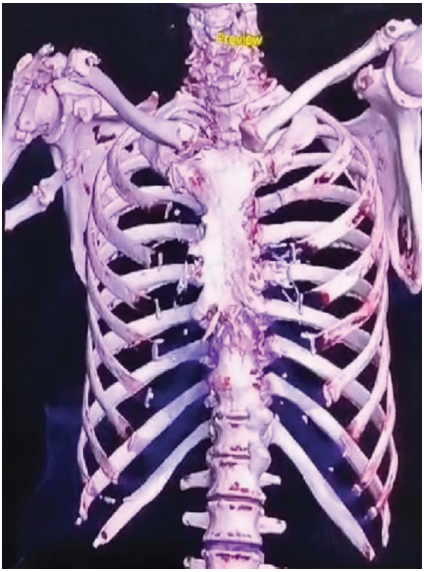
Figure 3: Computed tomography scan, three-dimensional reconstruction of a bipolar clavicle fracture.
The patient underwent open reduction and internal fixation under general anesthesia. The patient was placed in a modified beach chair position during the procedure. No single clavicular plate was available that could fix the bipolar clavicle fracture, so planned fixation with two separate plates. A 5 cm incision was made over the medial third of the clavicle [Fig. 4], the fracture was reduced, and it was fixed with a 3-hole opposite side lateral clavicular locking compression plate (LCP) (3.5 mm–2.7 mm system).
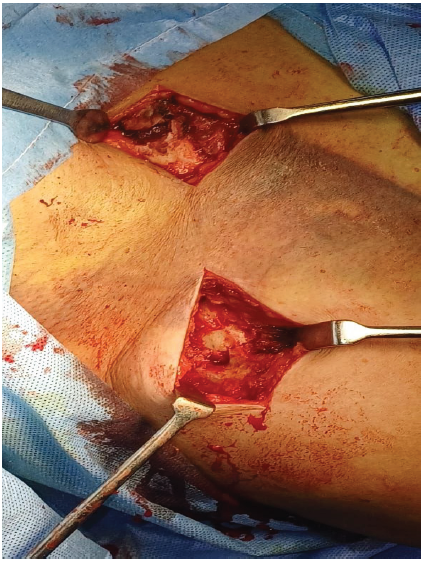
Figure 4: Exposure of fracture site, lateral and medial incision over fracture site.
Subsequently, a 7 cm lateral clavicular incision was made, and the fracture was reduced and fixed with a 4-hole right lateral clavicular LCP [Fig. 5].
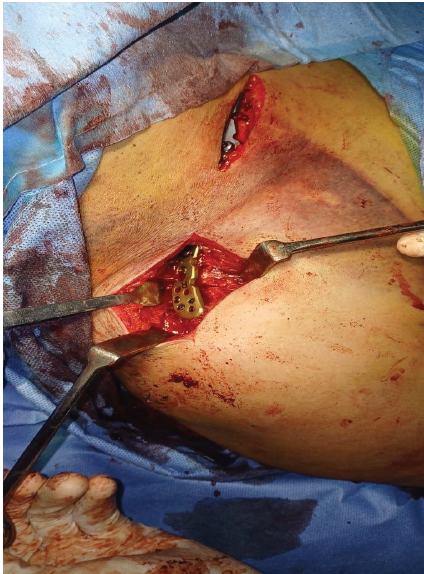
Figure 5: Fracture reduced and fixed with 3 and 4 hole lateral clavicular plate over medial and lateral, respectively.
To avoid stress raisers, plates were fixed at different planes. Early mobilization was initiated post-operatively. Arm abduction was restricted to <90°. For 12 weeks, weight-bearing activities were avoided. Weekly follow-up was advised for the initial 6 weeks, followed by 3 weeks of follow-up till 3 months, subsequently at 6 months interval [fig-6/7]. The 6-week post-operative X-ray showed signs of fracture healing and a maintained anatomical reduction. The 1-year follow -up X-ray showed a united fracture. Outcome was assessed using the Disability of the Arm, Shoulder, and Hand score.
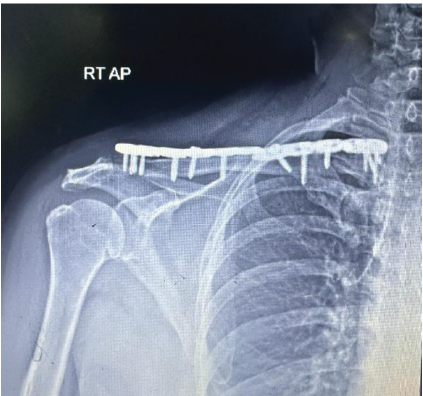
Figure 6: Post-operative X-ray, showing reduced bipolar clavicle fracture.
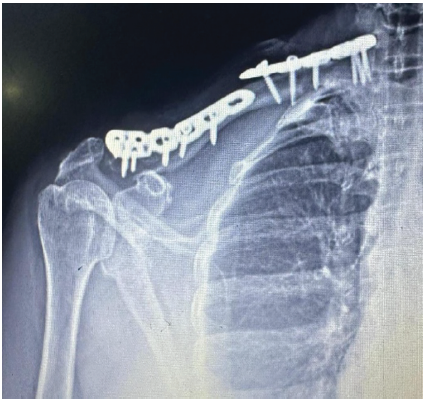
Figure 7: Post-operative X-ray, showing reduced bipolar clavicle fracture.
Bipolar clavicle fractures are a rare but complex form of clavicular injury, characterized by fractures occurring at both the medial and lateral ends of the clavicle. It presents unique challenges due to the instability of both ends. Unlike more common midshaft clavicle fractures, which account for the majority of clavicular injuries, bipolar fractures are often associated with high-energy trauma, such as motor vehicle accidents, falls from height, or contact sports. These fractures can significantly impact shoulder function due to the involvement of both the bone and adjacent neurovascular structures, making them a challenging clinical scenario. The mechanism of injury leading to a bipolar clavicle fracture is poorly understood [9]. Bipolar fractures have been reported to occur with trivial trauma in elderly patients with osteoporotic bone [8,10]. A clavicle fracture may present with various signs and symptoms based on the location of the fracture. May include pain, tenderness around the fracture site, and occasionally ecchymosis and skin tenting due to the displaced segment [5,6]. Bipolar fractures might be missed, as visualization around the medial clavicle on plain radiographs might be difficult because of the overlying structures in the chest. In such cases, CT imaging with three-dimensional reconstructions might be crucial for diagnosis [6]. Fixation of medial clavicular fracture is challenging, modified beach chair position and adequate fluoroscopy avoids major injuries. Being unstable injury, bipolar fractures are at an increased risk of non-union, and operative management is preferred for better outcomes [2]. Probability of non-union is positively correlated with age and degree of displacement of fracture fragments [11]. Non-union of a clavicle fracture may lead to functional deficit, pain, and other complications. Due to the lack of standardized management guidelines for bipolar clavicle fractures, the majority of reported cases have undergone operative treatment.
Bipolar clavicle fractures, though rare, present a significant challenge in orthopedic practice due to their complexity and potential for long-term functional impairment. Early recognition of these fractures is crucial for guiding treatment strategies. While non-operative management may suffice for less severe cases, surgical intervention is often necessary to restore clavicular alignment, stabilize the fracture, and prevent complications, such as malunion or non-union. Advances in surgical techniques, have improved outcomes, but careful patient selection and individualized treatment plans remain vital. Ongoing research into optimal management strategies and rehabilitation protocols will further refine the approach to this challenging injury.
Bipolar clavicle fractures are complex injuries requiring careful evaluation and individualized management. Surgical intervention is often necessary to restore function and prevent complications, such as non-union or malunion. Early recognition and accurate imaging are key to achieving optimal outcomes.
References
- 1. De Ruiter KJ, Gardenbroek TJ, Bos K, van Heijl M, Halm JA. Bipolar clavicular fractures and treatment options. Eur J Trauma Emerg Surg 2021;47:1407-10. [Google Scholar] [PubMed]
- 2. Heywood R, Clasper J. An unusual case of segmental clavicle fracture. J R Army Med Corps 2005;151:93-4. [Google Scholar] [PubMed]
- 3. Khan LAK, Bradnock TJ, Scott C, Robinson CM. Fractures of the clavicle. J Bone Joint Surg 2009;91:447-60. [Google Scholar] [PubMed]
- 4. Salipas A, Kimmel LA, Edwards ER, Rakhra S, Moaveni AK. Natural history of medial clavicle fractures. Injury 2016;47:2235-9. [Google Scholar] [PubMed]
- 5. Daolagupu AK, Gogoi PJ, Mudiganty S. A rare case of segmental clavicle fracture in an adolescent. Case Rep Orthop 2013;2013:248159. [Google Scholar] [PubMed]
- 6. Sethi K, Newman SD, Bhattacharya R. An unusual case of bipolar segmental clavicle fracture. Orthop Rev 2012;4:e26. [Google Scholar] [PubMed]
- 7. Sono T, Sagami A, Takatsuka K. Dual plating for bipolar clavicle fractures: A case report. Trauma Case Rep 2021;34:100494. [Google Scholar] [PubMed]
- 8. Talboys RJ, Mak M, Modi N, Garg S, Deo H. A unique bipolar clavicle fracture sustained with minimal trauma. Int J Shoulder Surg 2016;10:49-51. [Google Scholar] [PubMed]
- 9. Ogawa T, Sasaki T, Masayuki-Kawashima MK, Okawa A, Mahito-Kawashima MK. Internal fixation of only the distal end in a bipolar segmental clavicle fracture: A case report. Malays Orthop J 2017;11:47-9. [Google Scholar] [PubMed]
- 10. Maalouly J, Aouad D, Saade J, Abboud G, El Rassi G. Bipolar clavicular fracture on ipsilateral reverse shoulder prosthesis: Case report. Int J Surg Case Rep 2019;65:176-9. [Google Scholar] [PubMed]
- 11. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br 1998;80:476-84. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Neglected Isolated Lunate Dislocation in a Polytrauma Patient Presenting as Acute Carpal Tunnel Syndrome – A Case Report with Review of Literature
September 1, 2025 Neglected Isolated Lunate Dislocation in a Polytrauma Patient Presenting as Acute Carpal Tunnel Syndrome – A Case Report with Review of Literature June 1, 2026 Bipolar Clavicle Fracture: A Rare Entity of the Commonest Fracture – A Case Report
June 1, 2026 Bipolar Clavicle Fracture: A Rare Entity of the Commonest Fracture – A Case Report May 1, 2026 Temporary Fusionless Occipitocervical Fixation of Bilateral Occipital Condylar Avulsion Fractures in an Adult
May 1, 2026 Temporary Fusionless Occipitocervical Fixation of Bilateral Occipital Condylar Avulsion Fractures in an Adult May 1, 2026 Medial Hoffa’s Fracture Treated with Subvastus Approach – Case Series
May 1, 2026 Medial Hoffa’s Fracture Treated with Subvastus Approach – Case Series