
Orthopaedic Surgeons must have basic knowledge of imaging modalities.
Gokhale Nikhil Abhay,
502/50, Ganesh Sadan, L.T. Road No. 3, Goregaon (W), Mumbai – 400 062, Maharashtra, India.
E-mail: nikhilgokhale125@gmail.com
Abstract
Introduction: Normal menisci of the knee are semilunar structures. Sometimes a meniscus may be found to be thickened and disc like and is called a discoid meniscus. Such a discoid variant is usually found in the lateral meniscus. Its occurrence in the medial meniscus is extremely rare.
Case Report: We report a case of an 18 year old female , who presented to us with knee pain and was found to have a discoid medial meniscus with a tear. We operated upon her arthroscopically and performed meniscectomy and meniscoplasty. Postoperatively, the patient was free of her knee pain.
Conclusion: Discoid medial meniscus is a rare phenomenon which can present as a cause of knee pain. If discoid meniscus is symptomatic, the management includes arthroscopic meniscectomy and meniscoplasty.
Key Words: Meniscoplasty, discoid medial meniscus, arthroscopic meniscectomy.
The menisci are semilunar discs of fibrocartilaginous tissue which play critical roles in knee joint biomechanics [1]. Menisci function to (a) distribute forces equally across the joint surface, (b) stabilize the contact between the femur and tibia, (c) aid in joint proprioception, and (d) aid in lubrication [2,3]. Normal menisci are shaped like crescent moons, in fact the word “meniscus” comes from the Greek word for crescent. A discoid meniscus is a thickened disk-like morphologic variant of a normal meniscus [4]. Discoid meniscus is a relatively rare condition of the knee more frequently found in the lateral meniscus. Discoid medial menisci are even rare. Smillie[5] reported 467 patients had a discoid lateral meniscus and only 7 had a discoid medial meniscus in 10,000 meniscectomies. There have been only few case reports with anomalous discoid medial meniscus. We describe a case of discoid medial meniscus which was symptomatic due to a large intrasubstance horizontal tear.
A 18 year old female patient presented to our out patient department with pain in her left knee of 3 years duration. There was history of fall 3 years ago. She felt pain while walking and while standing up from squatting position. The patient gave no history of locking episodes. On clinical examination there was no obvious swelling over her left knee. There was no tenderness around the knee except for tenderness over the medial joint line. The patient complained of pain during terminal flexion. There was no laxity in the knee. McMurray test was positive for the medial meniscus. Rest of the examination of the knee was unremarkable.
The patient had already been treated with physiotherapy and occasional analgesics. We decided to image the left knee. The radiographs of the knee revealed no abnormality [Fig. 1]. We performed MRI scan of the knee and expected it to show a medial meniscal tear. Initial reporting by the radiologist confirmed a medial meniscal tear without a mention of it being discoid. However because the body of the meniscus was seen in 4 consecutive saggital sections of the MRI scan[Figs. 2 and 3], we suspected a discoid medial meniscus and got the scan reported again. This time the radiologist reported it as a torn discoid medial meniscus. We decided to perform arthroscopic partial meniscectomy and meniscoplasty for the patient.
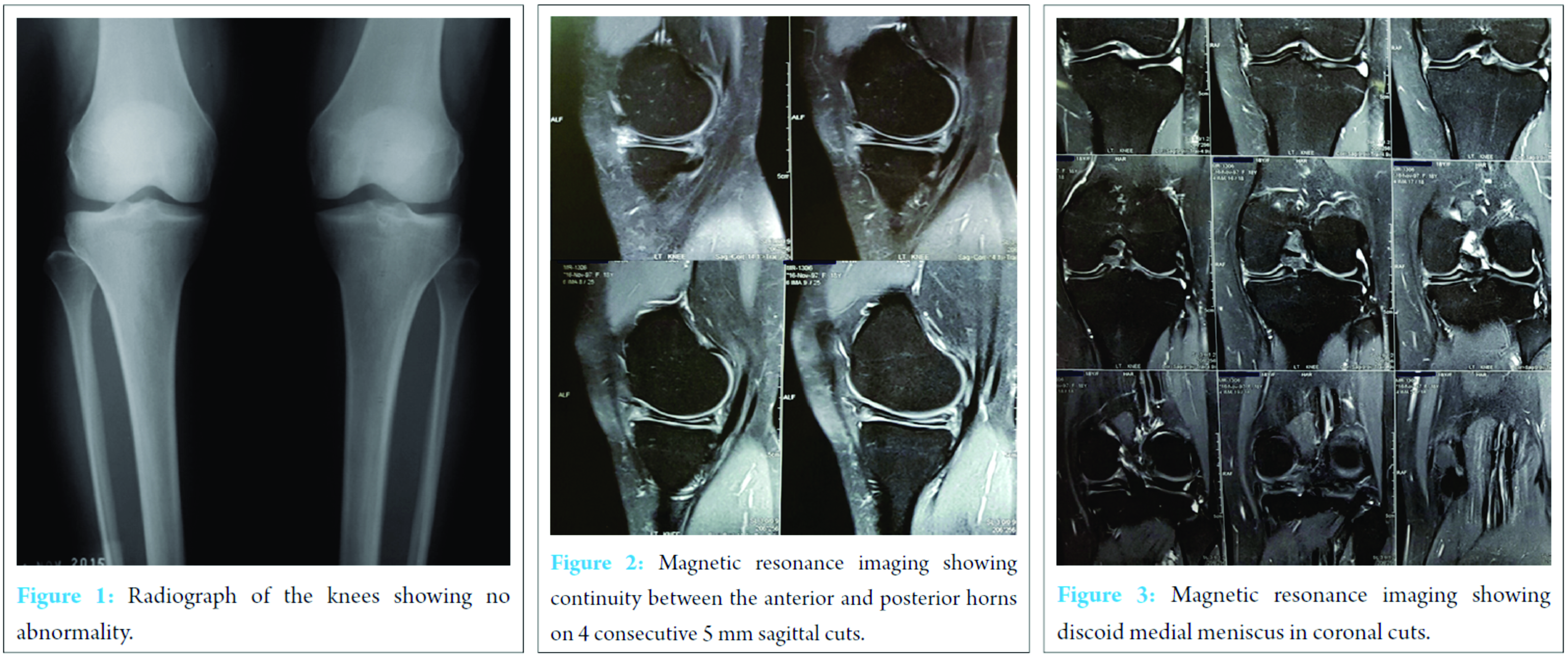
Arthroscopy confirmed a discoid medial meniscus occupying the entire medial tibial plateau [Figure 4]. The anterior part of the discoid meniscus was attached along the anterior cruciate ligament [Fig. 5]. However no obvious tear could be visualised [Figure 6].

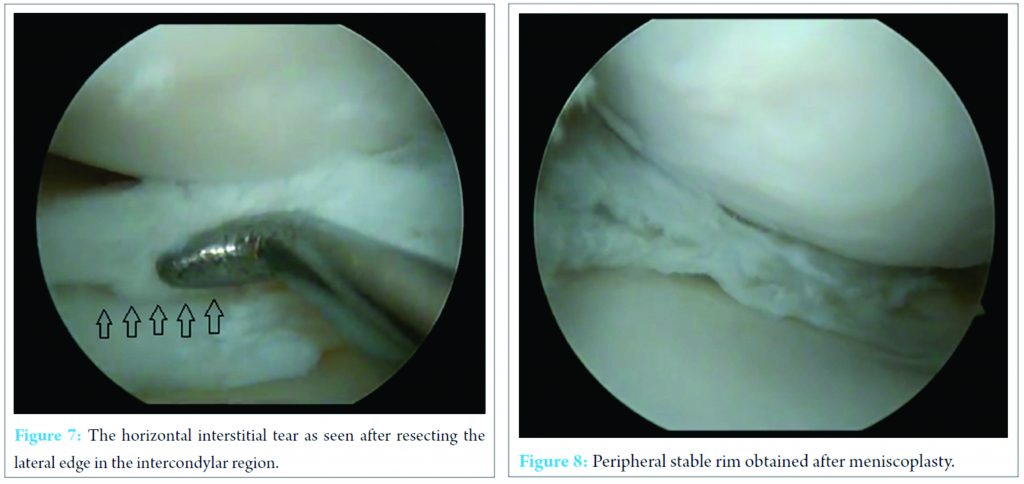
We then trimmed the lateral edge of the meniscus lying towards the intercondylar region which revealed a large cleaveage tear completely restricted to the intersttial part [Fig. 7]. We resected the upper and lower flaps till a stable peripheral semilunar rim of meniscus was obtained[Fig. 8]. Post operatively the patient was started on a physiotherapy protocol to preserve range of motion and muscle strength. Weight bearing was started after pain due to surgery subsided. 2 weeks postoperatively the patient attained full range of motion and was pain free even on terminal flexion.
Discoid medial meniscus was reported for first time by Cave and Staples in 1941 [6]. It is an extremely rare anomaly with an incidence of 0.1-0.3% [7]. Smillie [5] implicated defective disappearance of the meniscal centre during fetal development, with persistence of a fetal stage into adulthood. According to Kaplan [8], discoid lateral meniscus is a pathologic entity developing under certain conditions and influenced by mechanical factors such as posterior segment hypermobility; however, he had no explanation for discoid medial meniscus.
Clinically, the most frequent symptoms in discoid medial meniscus are medial knee pain, iterative effusion and locking in flexion none of which are specific. Knee snapping is rarer than in discoid lateral meniscus. Pain and effusion are more probably due to the meniscal tear than to the discoid shape of the meniscus . Locking may be due to the discoid shape as such, with the thick central region passing forward of the medial condyle[9]. Radiographs, in selected cases, may show a widened medial joint space with squaring of the femoral condyles [10] or depression of the tibial plateau [11]. The MRI is usually diagnostic, showing discoid medial meniscus with associated tears and anomalies of attachment of the meniscal horns. The diagnosis requires continuity between the anterior and posterior horns on three consecutive 5 mm sagittal slices [12] Tachibana and Lee both recommend systematic MRI of the asymptomatic contralateral knee [12,13]; they consider the incidence of bilateral cases to be underestimated. As the abnormality is congenital, they believe it to be usually bilateral. We performed MRI of the opposite asymptomatic knee of our patient but the medial meniscus of the opposite knee was not discoid.
Anomalies associated with the discoid medial meniscus have also been reported. These include depression of the tibial plateau, anomalous attachment of the anterior horn to the ACL, meniscal cyst, pathologic medial patella plica, and discoid lateral meniscus on the same knee.[11,13,14,15-18]. The most frequent anomalies are associated with anomalous insertion of the ACL.[15,17,18]. Kim et al reported anterior transposition of the anterior horn of the medial discoid meniscus below the anterior edge of the tibia plateau.
Asymptomatic discoid medial menisci should be left alone. Patel believes that the discoid meniscus should be preserved if “severe symptoms are not present” [19]. The treatment of symptomatic discoid medial meniscus is essentially surgical. Arthroscopy identifies the type of discoid meniscus and associated tears/unstable flaps. Partial meniscectomy, with excision of the central anomalous discoid meniscus and preservation of stable peripheral rim, is the preferred treatment. Several tears are amenable to arthroscopic repair. The patients must always be counselled that they are always at a higher risk for meniscal injuries in the future due to the abnormal morphology of the meniscus and hence, might require lifestyle and activity modification.[20] Sung-Jae Kim has described a surgical technique of arthroscopic excision of the symptomatic discoid medial meniscus in one piece which leads to less formation of foreign bodies, and is a time-saving technique.[21]
Discoid medial meniscus is a rare phenomenon which can present as a cause of knee pain. If discoid meniscus is symptomatic, the management includes arthroscopic meniscectomy and meniscoplasty. The opposite knee must be screened to look for presence of bilateral discoid medial menisci. The patient must be advised to exercise precautions and activity modification to prevent future symptoms.
Orthopaedic surgeons must have working knowledge about interpretation of imaging modalities like MRI. Rare abnormalities if found on MRI should be dealt with appropriately.
References
- 1. McDermott ID, Masouros SD, Amis AA (2008) Biomechanics of the menisci of the knee. Curr Orthopaed 22:193–201 [Google Scholar] [PubMed]
- 2. B. R. Barber and E. G. McNally, “Meniscal injuries and imaging the postoperative meniscus,” Radiologic Clinics of North America, 2013vol. 51, no. 3, 371–391. [Google Scholar] [PubMed]
- 3. I. D. Hutchinson, C. J. Moran, H. G. Potter, R. F. Warren, and S. A. Rodeo, “Restoration of the meniscus: form and function,”American Journal of Sports Medicine, 2014 vol. 42, no. 4, 987–998. [Google Scholar] [PubMed]
- 4. L.-X. Chen, Y.-F. Ao, J.-K. Yu et al., “Clinical features and prognosis of discoid medial meniscus,” Knee Surgery, Sports Traumatology, Arthroscopy, 2013, vol. 21, no. 2, 398–402. [Google Scholar] [PubMed]
- 5. Smille IS: The congenital discoid meniscus. J Bone Joint Surg Br;1948; 30; 671-682. [Google Scholar] [PubMed]
- 6. Cave EF, Staples OS (1941) Congenital discoid meniscus: A cause of internal impingement of the knee. Am J Surg 54: 371-376. [Google Scholar] [PubMed]
- 7. Ryu KN, Kim IS, Kim EJ, Ahn JW, Bae DK, et al. (1998) MR imaging of tears of discoid lateral menisci. AJR Am J Roentgenol 171(4): 963-967. [Google Scholar] [PubMed]
- 8. Kaplan E.B. Discoid lateral meniscus of the knee joint; nature, mechanism, and operative treatment J Bone Joint Surg Am 1957 ; 39–A : 77-87. [Google Scholar] [PubMed]
- 9. Flouzat-Lachaniette CH, Pujol N, Boisrenoult P, Beaufils P. Discoid medial meniscus: report of four cases and literature review. Orthop Traumatol Surg Res. 2011;97(8):826–32. [Google Scholar] [PubMed]
- 10. Lowenberg DW, Feldman ML. Magnetic resonance imaging diagnosis of discoid medial meniscus. Arthroscopy. 1993;9(6):704-6. [Google Scholar] [PubMed]
- 11. Pinar H, Akseki D, Karaoglan O, Ozkan M, Uluc E. Bilateral discoid medial menisci. Arthroscopy. 2000;16(1):96-101. [Google Scholar] [PubMed]
- 12. Tachibana Y., Yamazaki Y., Ninomiya S. Discoid medial meniscus Arthroscopy 2003 ; 19 : E12-E18 [Google Scholar] [PubMed]
- 13. Lee B.I., Lee Y.S., Kwon S.W., Choi S.W., Cho K.H., Kwon Y.J. Bilateral symptomatic discoid medial meniscus: report of three cases. Knee Surg Sports Traumatol Arthrosc. 2007 ; 15 : 739-743 [Google Scholar] [PubMed]
- 14. Franceschi F, Longo UG, Ruzzini L, Simoni P, Zobel BB, Denaro V. Bilateral complete discoid medial meniscus combined with posterior cyst formation. Knee Surg Sports Traumatol Arthrosc. 2007;15(3):266–8 [Google Scholar] [PubMed]
- 15. Jung YB, Yum JK, Bae YJ, Song KS. Anomalous insertion of the medial menisci. Arthroscopy. 1998; 14(5):505-507. [Google Scholar] [PubMed]
- 16. Kim SJ, Lee YT, Kim DW. Intraarticular anatomic variants associated with discoid meniscus in Koreans. Clin Orthop Relat Res. 1998; (356):202-207. [Google Scholar] [PubMed]
- 17. Min BH, Ha HK, Khang SY. Medial discoid meniscus completely coalesced with the anterior cruciate ligament. Arthroscopy. 2001; 17(7):E27. [Google Scholar] [PubMed]
- 18. Cha JG, Min KD, Han JK, et al. Anomalous insertion of the medial meniscus into the anterior cruciate ligament: the MR appearance published online ahead of print October 30, 2007.. Br J Radiol. 2008; 81(961):20-24. [Google Scholar] [PubMed]
- 19. Patel D, Dimakopoulos P, Denoncourt P: Bucket handle tear of a discoid medial meniscus. Arthroscopic diagnosis-partial excision. A case report. Orthopedics 1986, 9:607-608. [Google Scholar] [PubMed]
- 20. Kini SG, Walker P, Bruce W: Bilateral Symptomatic Discoid Medial Meniscus of the Knee-Case Report and Review of Literature. Archives of Trauma Research; 2015 March; 4(1):e27115. [Google Scholar] [PubMed]
- 21. Kim S-J, Kwun JD, Jung KA, Kim JM. Arthroscopic excision of the symptomatic discoid medial meniscus in one piece: A surgical technique. Arthroscopy 2005;21:1515.e1-1515.e4 [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 September 24, 2017 Subtotal Calcanectomy for the Treatment of Chronic Ulcer Associated with Osteomyelitis: A Case Report
September 24, 2017 Subtotal Calcanectomy for the Treatment of Chronic Ulcer Associated with Osteomyelitis: A Case Report January 1, 2025 Femoral Nerve injury from slip and fall: A novel presentation of debilitating injury
January 1, 2025 Femoral Nerve injury from slip and fall: A novel presentation of debilitating injury May 22, 2018 Chronic Recurrent Multifocal Osteomyelitis – A Rare Clinical Presentation and Review of Literature
May 22, 2018 Chronic Recurrent Multifocal Osteomyelitis – A Rare Clinical Presentation and Review of Literature November 10, 2022 Recurrent Intra-articular Synovial Hemangioma – A Case Report
November 10, 2022 Recurrent Intra-articular Synovial Hemangioma – A Case Report