
Patients who undergo shoulder arthroplasty procedures requiring post-operative warfarin initiation, especially those with possible warfarin sensitivity, are at high risk for delayed spontaneous hemorrhage even when anticoagulation is resumed in accordance with national guidelines.
Dr. J Michael Wiater, Department of Orthopaedic Surgery, Oakland University William Beaumont School of Medicine, Michigan, United States. E-mail: j.michael.wiater@corewellhealth.org
Abstract
Introduction: Warfarin is a widely used anticoagulant with a narrow therapeutic index and significant bleeding risk. Accounts of warfarin-associated spontaneous hemorrhage have been documented, but few reports in the orthopedic literature describe this event and its complications following reinitiation of warfarin in the post-operative period.
Case Presentation: A 70-year-old Caucasian woman with antiphospholipid syndrome developed spontaneous hemorrhage from the lateral pectoral artery following reinitiation of warfarin after ipsilateral reverse total shoulder arthroplasty (RTSA), successfully managed with anticoagulation reversal, embolization, and chest wall hematoma evacuation. To our knowledge, this is the first case report of perioperative warfarin-associated spontaneous hemorrhage from the lateral pectoral artery after RTSA.
Conclusion: As surgical candidates become more medically complex, it is essential that surgeons develop the ability to identify preoperatively patients at high risk for bleeding, take steps to minimize risk factors for bleeding, and learn how to manage spontaneous hemorrhage using a multidisciplinary approach.
Keywords: Warfarin, reverse total shoulder arthroplasty, shoulder arthroplasty, spontaneous hemorrhage, warfarin sensitivity, lateral pectoral artery.
Reverse total shoulder arthroplasty (RTSA) has become increasingly popular over the past decade for the treatment of multiple shoulder conditions, most commonly rotator cuff arthropathy [1,2,3]. While scapular notching, glenoid component loosening, and prosthetic dislocation are common complications, acromial fracture, infection, hematoma, and, rarely, neurologic and vascular injury can also occur [4,5]. As patient populations become more medically complex [6,7], it is important for surgeons to carefully examine and control modifiable patient factors that could lead to surgical complications. This is particularly crucial for patients with hypercoagulable diseases on long-term anticoagulants, such as warfarin, given the drug’s narrow therapeutic range and need for meticulous monitoring. Further, allelic variants of CYP2C9, the hepatic enzyme that metabolizes warfarin, can result in patients with heightened warfarin sensitivity and difficulty maintaining therapeutic international normalized ratio (INR) ranges [8,9]. Warfarin sensitivity may not be initially recognized by medical care teams, leading to increased bleeding risk when these patients are treated with standard warfarin doses [8]. Spontaneous hemorrhage secondary to warfarin use resulting in retroperitoneal, intramuscular, intracerebral, and subinguinal hematomas is well documented [10,11,12,13,14]. However, reports of spontaneous hemorrhage after reinitiation of warfarin in the post-operative period are limited, and none, to our knowledge, have been described involving the lateral pectoral artery after RTSA. In this report, we present a rare case of delayed spontaneous hemorrhage from the lateral pectoral artery following warfarin reinitiation in a patient with antiphospholipid syndrome (APS) after ipsilateral RTSA, managed with anticoagulation reversal, embolization, and chest wall hematoma evacuation.
A 70-year-old woman with chronic left shoulder pain and weakness presented to our clinic and was diagnosed with rotator cuff arthropathy (Fig. 1).
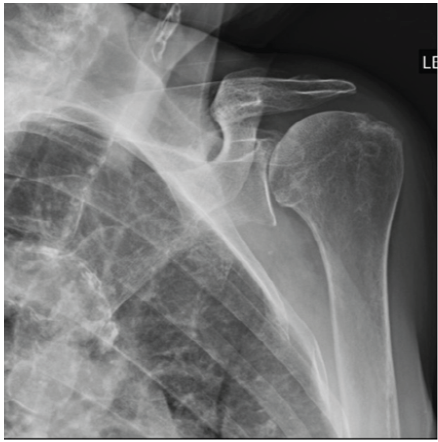
Figure 1: A pre-operative Grashey view radiograph of the left shoulder.
Due to her limited shoulder function and pain, she wished to proceed with RTSA. Her medical history was significant for antiphospholipid syndrome (APS) managed with warfarin, chronic anemia, deep vein thrombosis (DVT) while previously on Eliquis, chronic obstructive pulmonary disease, systemic lupus erythematosus (SLE), non-ST-segment elevation myocardial infarction, empyema, and Raynaud’s disease. Her pertinent surgical history included arthroscopic repair of a massive rotator cuff tear in the left shoulder in 2018. Past episodes of supratherapeutic INR values of 3.8–7.3 were documented in the medical record, necessitating decreased warfarin doses and suggesting warfarin sensitivity. The patient had not undergone warfarin sensitivity genotyping.
The patient discontinued warfarin 5 days before her scheduled arthroplasty procedure and began taking 60 mg enoxaparin twice daily. Enoxaparin was then held for 48 h before surgery. Given the patient’s history of APS and prior embolic episodes, timely reinitiation of anticoagulation with enoxaparin 24–48 h after the date of surgery was recommended by her Internal Medicine physician. As per the American Society of Hematology’s guidelines, if a patient’s INR is >1.5 on the date of surgery, it is recommended that procedures with a high bleeding risk do not proceed [15]. Our patient’s INR was 1.1 on the date of surgery. After general anesthesia was induced, the patient was placed in the beach chair position and a standard deltopectoral approach was performed. Access to the joint was obtained through a subscapularis tenotomy. A standard humeral neck osteotomy and soft tissue releases were performed. Implantation of the INHANCE™ reverse prosthesis (Johnson and Johnson MedTech, Raynham, MA, USA) was uneventful. The subscapularis tenotomy was repaired and the surgical wound was closed with absorbable suture. No significant bleeding was encountered. Drain placement was not needed. The patient was placed in a shoulder immobilizer with an abduction pillow and transported to the post-operative recovery room (Fig. 2). Total blood loss during the procedure was 150 mL and post-operative hemoglobin was 8.8 g/dL. Tranexamic acid 1 g infusion was administered at the beginning and end of the case for a total of 2 g.
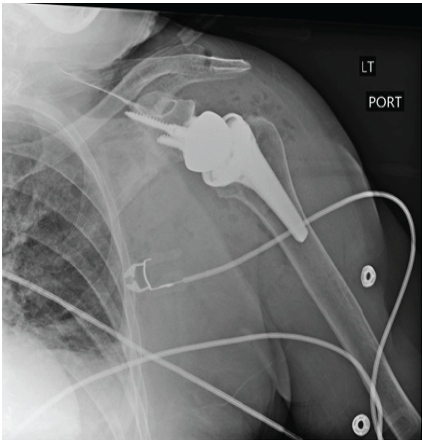
Figure 2: Anterior-posterior radiograph of the left shoulder on the 1st post-operative day after reverse total shoulder arthroplasty, demonstrating a reduced shoulder with good alignment of the components.
In consultation with Internal Medicine, Hematology, and inpatient pharmacy, 3 mg of warfarin and 60 mg of enoxaparin twice daily bridge therapy were resumed post-operative day (POD) 2. By POD 5, INR had risen rapidly from 1.6 to 2.8, falling within the target therapeutic range of 2–3. Despite holding warfarin beginning POD 5, the patient became supratherapeutic on POD 6 with INR of 3.6 and remained supratherapeutic from that point on. On POD 8, the patient developed acute hypotension, tachycardia, and was noted to have large, firm swelling of the left chest wall (Fig. 3).

Figure 3: Clinical photograph demonstrating left chest wall hematoma with overlying ecchymosis on post-operative day 8.
Hemoglobin also dropped acutely from 7.5 g/dL to 4.8 g/dL. Warfarin reversal was initiated immediately with two units of fresh frozen plasma and intravenous vitamin K, followed by 2,000 units of prothrombin complex concentrate to more expeditiously reverse anticoagulation without causing hypervolemia. Two units of packed red blood cells were administered, increasing her hemoglobin to 8.4 g/dL and resolving the hemodynamic instability. Computed tomography (CT) of angiography of the left upper extremity was obtained and revealed a large pectoral hematoma measuring 16.0 × 9.6 × 17.5 cm with active contrast extravasation from the lateral pectoral artery, a branch of the second segment of the axillary artery (Fig. 4). INR decreased from 3.8 to 1 by the next day.
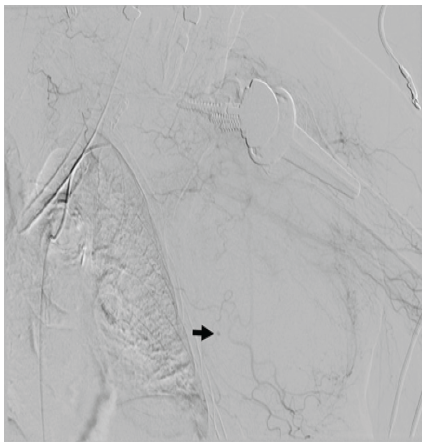
Figure 4: Angiogram demonstrating contrast extravasation from a branch of the lateral pectoral artery in the soft tissues of the left chest wall (arrow).
Interventional radiology was consulted for embolization of the left lateral pectoral artery. This initial attempt through the left superficial femoral artery was unsuccessful due to the acute angle of the artery takeoff and the narrow lumen from atherosclerosis. A second attempt through the left brachial artery was again unsuccessful. Instead, a 6 mm × 5 cm Gore VIABAHN™ (W.L. Gore and Associates, Inc., Flagstaff, AZ, USA) stent was placed over the origin of the lateral pectoral artery to occlude the vessel and prevent any further hemorrhage. The hematoma stabilized with no further expansion on examination. After the procedure, the patient was hemodynamically stable with hemoglobin of 9.4 g/dL. Due to pain and concern for skin necrosis of the left chest wall, hematoma evacuation was performed in the operating room on POD 10. Warfarin with enoxaparin bridge was resumed 5 days after this procedure without hematoma recurrence, and the patient was discharged uneventfully 8 days later.
Post-operative anticoagulation management in patients at risk for venous thromboembolism (VTE) requires careful consideration of each individual’s prothrombotic and bleeding risk factors as well as timeline to reinitiation of anticoagulation, particularly in those with known thrombophilia. APS is a thrombogenic disease caused by the production of antibodies that target phospholipids, leading to arterial and venous thrombosis (VT) which, in turn, results in complications such as ischemic stroke, myocardial infarction, and pulmonary embolism [16,17]. Anticoagulation with warfarin is the standard of care for the management of APS to prevent thrombosis [18,19]. Without anticoagulation, patients with APS have a monthly risk of VTE exceeding 10% [15]. In addition, patients with APS and a prior episode of thrombosis who subsequently discontinue anticoagulation have a 50% risk of recurrent VTE at 2 years and 78% risk at 8 years from the initial thrombotic event, illustrating the importance of consistent anticoagulation in this population [6]. APS can also be secondary to other primary autoimmune diseases with prothrombotic tendencies, such as SLE [20,21]. Patients with SLE and coexistent antiphospholipid antibodies have a 50–70% risk of VT, further increasing the risk of thrombosis compared to the general population [21,22]. Our patient had a history of both APS and SLE, a prior episode of DVT while on Eliquis, and was taking warfarin for the management of her APS. Timely resumption of post-operative anticoagulation was essential to minimize her risk of thrombosis not only due to APS but also the markedly increased risk of VTE after undergoing a major surgical procedure like RTSA [15]. The American Heart Association recommends initiating low-molecular-weight heparin bridge therapy 48–72 h after major surgical procedures where bleeding risk is high [23]. In accordance with these guidelines, our patient’s warfarin and enoxaparin bridge was initiated POD 2. However, the guidelines may not adequately address patients with warfarin sensitivity, such as our patient, whose baseline bleeding risk is greater than that of the general public. Although a delay of 72 h before reinitiation of warfarin and bridge therapy with enoxaparin may have further reduced our patient’s bleeding risk, the onset of acute anemia and hemodynamic instability occurred 6 days after reinitiation of warfarin, suggesting her bleeding event was more likely related to spontaneous hemorrhage rather than early initiation of post-operative anticoagulation. There are multiple reports of spontaneous hemorrhage associated with warfarin use in the medical literature, even at therapeutic INR levels [10,11,12,13,14,24,25]. In a post-operative setting, bleeding due to warfarin can have devastating consequences for patients. A case series by Meshram et al. [26] described patients with atrial fibrillation on warfarin – one who underwent shoulder manipulation under anesthesia and another RTSA – who both developed upper extremity acute compartment syndrome in the post-operative period requiring fasciotomies. Specifically, the patient who underwent RTSA developed a pulmonary embolism on POD 1 and was treated with warfarin. This led to hematoma formation 4 days later in the operative shoulder and subsequent compartment syndrome of the arm. Our patient demonstrated an episode of acute hemorrhage with hemodynamic instability and a 2.7 point decrease in hemoglobin 6 days after resuming warfarin with enoxaparin bridge therapy and 8 days from the initial date of surgery. The patient’s clinical presentation and timeline to bleeding were similar to a case wherein a patient underwent total knee arthroplasty and developed spontaneous hemorrhage from the superior geniculate artery 9 days after post-operative warfarin reinitiation [25]. In comparison, direct arterial injury during RTSA would demonstrate acute anemia, hemodynamic instability, and visible hematoma formation at the surgical site on examination within a few hours of the procedure, not days later [27].
Our case highlights the importance of careful patient selection and identification of patient-specific risk factors before surgery, such as medications and anticoagulation sensitivity, that could lead to severe perioperative complications. Surgeons who perform shoulder arthroplasty should be aware of the possibility of spontaneous hemorrhage in the post-operative period for patients treated with warfarin, particularly those with documented warfarin sensitivity, and, before surgery, be prepared to intervene should this complication arise. Understanding how to manage anticoagulants and quickly reverse their effects if needed, as well as prompt collaboration with subspecialists, is crucial to ensure timely control of bleeding.
Patients with hypercoagulable disorders and warfarin sensitivity are at increased risk for delayed, spontaneous hemorrhage after undergoing uncomplicated shoulder arthroplasty, even when INR levels are therapeutic. Surgeons should take the time to carefully evaluate each surgical candidate’s risk factors for bleeding and attempt to reduce any modifiable factors preoperatively. Hemodynamic instability and acute anemia that present several days after surgery should lead to urgent evaluation of possible arterial bleeding through CT angiography and prompt anticoagulation reversal by the surgical team. Multidisciplinary care is essential for patients with heightened anticoagulation sensitivity and should be established in the immediate post-operative period to ensure appropriate timing and doses of anticoagulants in these medically complex patients.
References
- 1. Kozak T, Bauer S, Walch G, Al-Karawi S, Blakeney W. An update on reverse total shoulder arthroplasty: Current indications, new designs, same old problems. EFORT Open Rev 2021;6:189-201. [Google Scholar] [PubMed]
- 2. Mayfield CK, Korber SS, Hwang NM, Bolia IK, Gamradt SC, Weber AE, et al. Volume, indications, and number of surgeons performing reverse total shoulder arthroplasty continue to expand: A nationwide cohort analysis from 2016-2020. JSES Int 2023;7:827-34. [Google Scholar] [PubMed]
- 3. Rugg CM, Coughlan MJ, Lansdown DA. Reverse total shoulder arthroplasty: Biomechanics and Indications. Curr Rev Musculoskelet Med 2019;12:542-53. [Google Scholar] [PubMed]
- 4. Farshad M, Gerber C. Reverse total shoulder arthroplasty-from the most to the least common complication. Int Orthop 2010;34:1075-82. [Google Scholar] [PubMed]
- 5. Kriechling P, Zaleski M, Loucas R, Loucas M, Fleischmann M, Wieser K. Complications and further surgery after reverse total shoulder arthroplasty: Report of 854 primary cases. Bone Joint J 2022;104-B:401-7. [Google Scholar] [PubMed]
- 6. Holman HR. The relation of the chronic disease epidemic to the health care crisis. ACR Open Rheumatol 2020;2:167-73. [Google Scholar] [PubMed]
- 7. Naik H, Murray TM, Khan M, Daly-Grafstein D, Liu G, Kassen BO, et al. Population-based trends in complexity of hospital inpatients. JAMA Intern Med 2024;184:183-92. [Google Scholar] [PubMed]
- 8. Ma Z, Wang P, Mahesh M, Elmi CP, Atashpanjeh S, Khalighi B, et al. Warfarin sensitivity is associated with increased hospital mortality in critically Ill patients. PLoS One 2022;17:e0267966. [Google Scholar] [PubMed]
- 9. Moyer TP, O’Kane DJ, Baudhuin LM, Wiley CL, Fortini A, Fisher PK, et al. Warfarin sensitivity genotyping: A review of the literature and summary of patient experience. Mayo Clin Proc 2009;84:1079-94. [Google Scholar] [PubMed]
- 10. Akuzawa N, Kurabayashi M. Multiple spontaneous hemorrhages after commencing warfarin therapy. SAGE Open Med Case Rep 2018;6:2050313X18778380 . [Google Scholar] [PubMed]
- 11. Benbouchta K, Mrabet A, Kallel O, El Ouafi N, Bazid Z. Spontaneous massive pectoral hematoma induced by vitamin K antagonist therapy: A case report. Pan Afr Med J 2021;38:324. [Google Scholar] [PubMed]
- 12. Koklu H, Oge Koklu N, Aksoy Khurami F, Duman E, Meral A. Therapy-related spontaneous pectoral muscle hematoma: A case report and review of the literature. J Am Geriatr Soc 2016;64:1135-7. [Google Scholar] [PubMed]
- 13. Lawrentschuk N, Kariappa S, Kaye AH. Spontaneous intracerebral haemorrhages-warfarin as a risk factor. J Clin Neurosci 2003;10:550-2. [Google Scholar] [PubMed]
- 14. Nasr MA, Khallafalla H, Kumar VR, Pathan SA. Warfarin-induced spontaneous retroperitoneal hemorrhage from the renal vein: A rare case with an uncommon etiology. Qatar Med J 2019;2019:6. [Google Scholar] [PubMed]
- 15. Spyropoulos AC, Douketis JD. How I treat anticoagulated patients undergoing an elective procedure or surgery. Blood 2012;120:2954-62. [Google Scholar] [PubMed]
- 16. Derksen RH, De Groot PG, Kater L, Nieuwenhuis HK. Patients with antiphospholipid antibodies and venous thrombosis should receive long term anticoagulant treatment. Ann Rheum Dis 1993;52:689-92. [Google Scholar] [PubMed]
- 17. Knight JS, Branch DW, Ortel TL. Antiphospholipid syndrome: Advances in diagnosis, pathogenesis, and management. BMJ 2023;380:e069717. [Google Scholar] [PubMed]
- 18. Farmer-Boatwright MK, Roubey RA. Venous thrombosis in the antiphospholipid syndrome. Arterioscler Thromb Vasc Biol 2009;29:321-5. [Google Scholar] [PubMed]
- 19. Pengo V, Ruffatti A, Legnani C, Gresele P, Barcellona D, Erba N, et al. Clinical course of high-risk patients diagnosed with antiphospholipid syndrome. J Thromb Haemost 2010;8:237-42. [Google Scholar] [PubMed]
- 20. Bazzan M, Vaccarino A, Marletto F. Systemic lupus erythematosus and thrombosis. Thromb J 2015;13:16. [Google Scholar] [PubMed]
- 21. Franco JS, Molano-González N, Rodríguez-Jiménez M, Acosta-Ampudia Y, Mantilla RD, Amaya-Amaya J, et al. The coexistence of antiphospholipid syndrome and systemic lupus erythematosus in Colombians. PLoS One 2014;9:e110242. [Google Scholar] [PubMed]
- 22. Hisada R, Atsumi T. An antiphospholipid antibody profile as a biomarker for thrombophilia in systemic lupus erythematosus. Biomolecules 2023;13:617. [Google Scholar] [PubMed]
- 23. Hirsh J, Fuster V, Ansell J, Halperin JL. American heart association/American college of cardiology foundation guide to warfarin therapy. Circulation 2003;107:1692-711. [Google Scholar] [PubMed]
- 24. Yang JC, Makaryus AN. Warfarin anticoagulation and spontaneous pectoral haematomas. Heart Lung Circ 2016;25:e81-4. [Google Scholar] [PubMed]
- 25. Yang JH, Kim JH, Lee SW, You J, Park SM, Kim SG. Acute compartment syndrome after restarting warfarin therapy following polyethylene exchange in unicompartmental knee arthroplasty: Case report. Heliyon 2022;8:e11838. [Google Scholar] [PubMed]
- 26. Meshram P, Joseph J, Zhou Y, McFarland EG. Acute compartment syndrome caused by hematoma after shoulder surgery: A case series. J Shoulder Elbow Surg 2021;30:1362-8. [Google Scholar] [PubMed]
- 27. Noh YM, Do HS, Heo SY. Occult thoracoacromial artery injury during reverse total shoulder arthroplasty resulting in a cascade of postoperative complications: A case report. Radiol Case Rep 2020;15:1657-62. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Strength Recovery with Lateralized Reverse Total Shoulder Arthroplasty Combined with Pectoralis Major Transfer for Rotator Cuff Arthropathy with Internal Rotational Deficiency: A Case Report
February 1, 2026 Strength Recovery with Lateralized Reverse Total Shoulder Arthroplasty Combined with Pectoralis Major Transfer for Rotator Cuff Arthropathy with Internal Rotational Deficiency: A Case Report December 1, 2025 Revision of Cemented Reverse Total Shoulder Arthroplasty with Bone Graft in Osteogenesis Imperfecta: A Case Report
December 1, 2025 Revision of Cemented Reverse Total Shoulder Arthroplasty with Bone Graft in Osteogenesis Imperfecta: A Case Report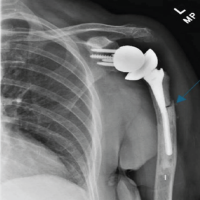 September 1, 2025 Transverse Periprosthetic Fracture With a Bent Stem Following Reverse Total Shoulder Arthroplasty – A Case Report
September 1, 2025 Transverse Periprosthetic Fracture With a Bent Stem Following Reverse Total Shoulder Arthroplasty – A Case Report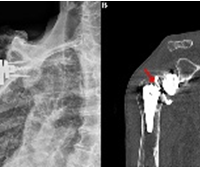 February 1, 2025 Revision Reverse Total Shoulder Arthroplasty Combined With Secondary Pectoralis Major Transfer for Tray-Taper Breakage and Internal Rotational Dysfunction: A Case Report
February 1, 2025 Revision Reverse Total Shoulder Arthroplasty Combined With Secondary Pectoralis Major Transfer for Tray-Taper Breakage and Internal Rotational Dysfunction: A Case Report