
Characteristic MRI fat-signal features allow confident diagnosis of intramedullary lipomas, preventing unnecessary biopsy or surgical intervention.
Dr. Yousif Jihad, Department of Trauma and Orthopaedics, United Lincolnshire Teaching Hospitals NHS Trust, Lincoln County Hospital, Lincoln, United Kingdom. E-mail: yousif.ghazwan2000@gmail.com
Abstract
Introduction: Intramedullary lipomas are rare benign bone tumors, most commonly involving the calcaneus, with femoral involvement being uncommon. They are frequently asymptomatic and discovered incidentally during imaging for unrelated complaints, which may raise concern for more aggressive pathology.
Case Report: A 64-year-old female presented following a mechanical fall with bilateral hip pain. Initial pelvic radiographs and computed tomography scans identified an elongated, non-aggressive lucent lesion in the proximal left femoral metaphysis. Subsequent magnetic resonance imaging (MRI) demonstrated homogeneous fat-signal characteristics with complete fat suppression and no aggressive features, consistent with an intramedullary lipoma. The lesion was entirely asymptomatic and unrelated to the presenting complaint. Conservative management with surveillance imaging was adopted.
Conclusion: Characteristic MRI features allow confident diagnosis of intramedullary lipomas, avoiding unnecessary biopsy or surgical intervention. Recognition of these lesions is essential when they are incidentally detected following trauma.
Keywords: Intramedullary lipoma, femur, incidental finding, benign bone tumor, magnetic resonance imaging.
Intramedullary lipomas are among the rarest benign bone tumors, accounting for <0.1% of all primary osseous neoplasms [1]. They are composed of mature adipose tissue within the medullary cavity and most frequently occur in the calcaneus, followed by the proximal femur, tibia, and fibula [1,2]. Many lesions remain clinically silent and are detected incidentally during imaging performed for unrelated pathology. Radiologically, intramedullary lipomas may mimic other lucent bone lesions, including bone infarction, liposclerosing myxofibrous tumor, and low-grade malignancy [2,3]. Magnetic resonance imaging (MRI) is pivotal in confirming the diagnosis by demonstrating fat-signal characteristics and excluding aggressive features [3]. We present a case of an incidentally detected intramedullary lipoma of the proximal femur identified during trauma imaging, highlighting the diagnostic features and management considerations relevant to orthopedic practice.
A 64-year-old female presented following a mechanical fall at work, reporting bilateral hip pain, more pronounced on the left side. The patient had no history of hip pain before the fall. Clinical examination demonstrated a preserved range of motion in both hips, with discomfort on weight bearing but no focal neurological deficit. Initial anteroposterior pelvic radiography demonstrated no acute fracture, but revealed a well-defined lucent lesion in the proximal left femur (Fig. 1). A computed tomography (CT) scan of the pelvis was subsequently performed to exclude an occult fracture. CT confirmed an elongated intramedullary lucent lesion within the proximal left femoral metaphysis, characterized by sclerotic margins without cortical destruction, endosteal scalloping, or an associated soft-tissue mass, suggesting a non-aggressive process (Fig. 2 and 3).
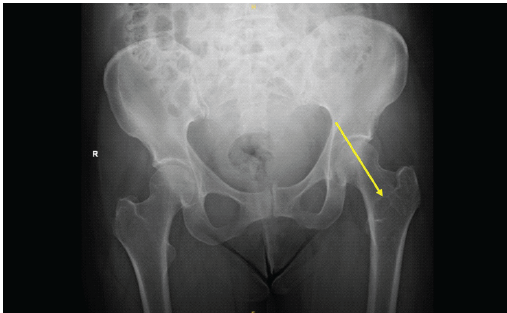
Figure 1: Anteroposterior pelvic radiograph demonstrating a well-defined lucent lesion in the proximal left femoral metaphysis (arrow), with no associated fracture.
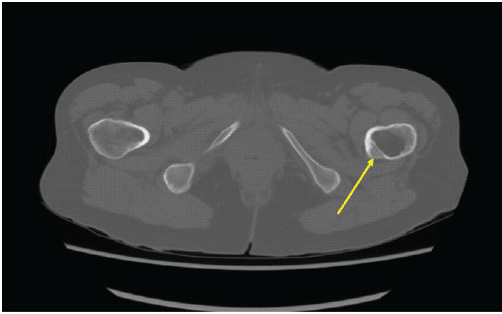
Figure 2: Axial computed tomography image at the level of the proximal femur showing a centrally located intramedullary lucent lesion with preserved cortical integrity and absence of endosteal scalloping or periosteal reaction (arrow).
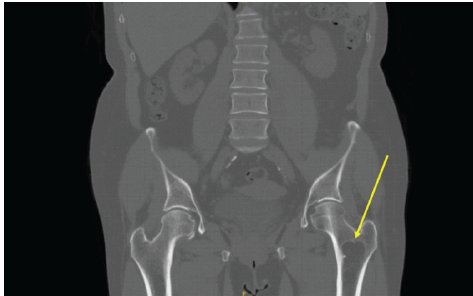
Figure 3: Coronal computed tomography of the pelvis demonstrating an elongated, well-defined intramedullary lucent lesion within the proximal left femoral metaphysis (arrow), with sclerotic margins and no cortical destruction or soft-tissue extension, consistent with a non-aggressive lesion.
Further MRI of the pelvis and hips demonstrated a well-circumscribed intramedullary lesion with homogeneous high signal intensity on T1-weighted sequences and complete signal suppression on fat-suppressed images (Fig. 4a). No surrounding marrow edema, cortical breach, or contrast enhancement was identified (Fig. 4b). These findings were diagnostic of an intramedullary lipoma. No features suggestive of malignant transformation were present.
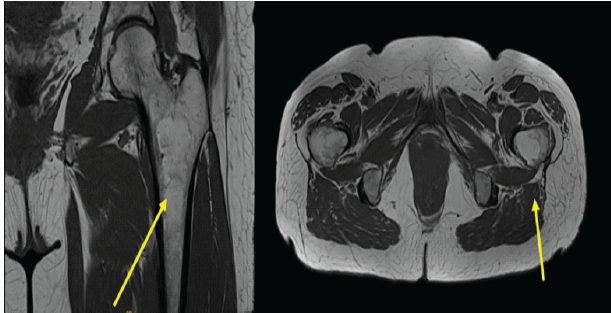
Figure 4: (a) Coronal T1-weighted magnetic resonance imaging (MRI) of the pelvis demonstrating a well-circumscribed intramedullary lesion within the proximal left femur exhibiting homogeneous high signal intensity consistent with fat content (arrow). (b) Axial T1-weighted MRI confirming central intramedullary location with preserved cortical margins and no surrounding marrow edema or soft-tissue extension (arrow).
The lesion was considered incidental and unrelated to the patient’s presenting symptoms. The patient was reviewed in the orthopedic clinic, reassured regarding the benign nature of the finding, and managed conservatively with interval MRI surveillance due to the lesion’s proximity to the femoral calcar.
Intramedullary lipomas are benign lesions composed of mature adipocytes within the medullary cavity. According to Milgram’s [1] classification, these tumors are classified into three stages: Stage I lesions consist of viable adipose tissue and appear as homogeneous fat-containing lesions; Stage II lesions demonstrate partial fat necrosis with focal calcification; and Stage III lesions show extensive fat necrosis, cystic change, and sclerosis (Fig. 5). The imaging characteristics in this case are consistent with a Stage I intramedullary lipoma.
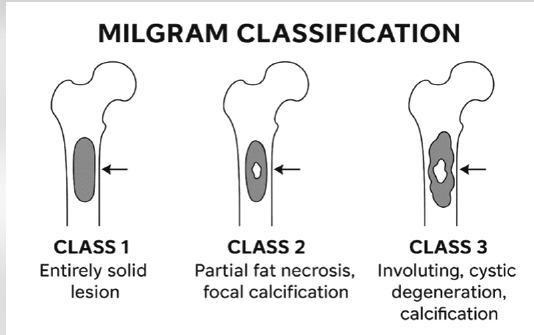
Figure 5: Schematic illustration of the Milgram classification of intramedullary lipomas.
Differentiating lipoma from bone infarction is particularly important, as both entities may demonstrate an intramedullary fat-signal on MRI [2,3]. Bone infarcts typically exhibit serpiginous peripheral margins, central necrosis, and reactive sclerosis, whereas intramedullary lipomas appear as well-circumscribed lesions with uniform fat-signal intensity and minimal reactive change [2,3]. Liposclerosing myxofibrous tumors represent another differential diagnosis, particularly in the proximal femur, but usually demonstrate mixed signal characteristics, ground-glass appearance, or fibrous components not seen in intramedullary lipomas [4,5]. The radiological diagnosis of an intramedullary lipoma relies heavily on cross-sectional imaging. CT typically demonstrates a well-defined intramedullary lesion with fat attenuation values and sclerotic margins, reflecting a non-aggressive process [6,7]. MRI is the modality of choice, characteristically showing homogeneous high signal intensity on T1-weighted images with complete signal suppression on fat-suppressed sequences and the absence of surrounding marrow edema or soft-tissue mass [7,8]. These features allow confident differentiation from malignant lipomatous tumors and other aggressive intramedullary lesions. Although intramedullary lipomas can occur throughout the skeleton, the proximal femur remains an uncommon site, accounting for a minority of reported cases [6,9]. Lesions in this location may raise concern for pathological fracture or malignancy, particularly when identified incidentally following trauma. However, multiple series have demonstrated that asymptomatic intramedullary lipomas without aggressive imaging features can be safely managed conservatively [1,2,6,8]. Surgical intervention or biopsy is generally reserved for symptomatic lesions, diagnostic uncertainty, features suggestive of malignancy, or structural compromise that poses a fracture risk [1,3,6,10]. In the present case, the lesion demonstrated classic Stage I features according to Milgram’s [1] classification, with homogeneous fat content and absence of necrosis or calcification. The lack of lesion-related symptoms, combined with characteristic MRI findings, supported a non-operative approach. Interval imaging surveillance was selected due to the lesion’s proximity to the femoral calcar, in keeping with previously published management strategies [6,8].
Intramedullary lipomas of the femur are rare and often discovered incidentally. Familiarity with their characteristic imaging appearance allows for confident diagnosis, patient reassurance, and the avoidance of unnecessary invasive procedures. Conservative management with surveillance is appropriate for asymptomatic lesions without aggressive features.
Intramedullary lipomas of the femur are rare and frequently incidental. Recognition of characteristic MRI fat-signal features enables accurate diagnosis and prevents unnecessary biopsy or surgical intervention.
References
- 1. Milgram JW. Intraosseous lipomas. A clinicopathologic study of 66 cases. Clin Orthop Relat Res 1988;231:277-302. [Google Scholar] [PubMed]
- 2. Campbell RS, Grainger AJ, Mangham DC, Beggs I, Teh J, Davies AM. Intraosseous lipoma: Report of 35 cases and review of the literature. Clin Radiol 2003;58:950-7. [Google Scholar] [PubMed]
- 3. Murphey MD, Carroll JF, Flemming DJ, Pope TL, Gannon FH, Kransdorf MJ. From the archives of the AFIP: Benign musculoskeletal lipomatous lesions. Radiographics 2004;24:1433-66. [Google Scholar] [PubMed]
- 4. Campbell RS, Grainger AJ. Imaging of benign intramedullary bone lesions. Semin Musculoskelet Radiol 2013;17:101-12. [Google Scholar] [PubMed]
- 5. Kransdorf MJ, Murphey MD. Imaging of benign skeletal lipomatous lesions. Radiol Clin North Am 2011;49:1295-313. [Google Scholar] [PubMed]
- 6. Radl R, Leithner A, Machacek F, Cetin E, Koehler W, Koppany B, et al. Intraosseous lipoma: Retrospective analysis of 29 patients. Int Orthop 2004;28:374-8. [Google Scholar] [PubMed]
- 7. Propeck T, Bullard MA, Lin J, Doi K, Martel W. Radiologic-pathologic correlation of intraosseous lipoma. AJR Am J Roentgenol 2000;175:673-8. [Google Scholar] [PubMed]
- 8. Herneth AM, Pretterklieber ML. Intraosseous lipoma: MRI findings and clinical relevance. Skeletal Radiol 2002;31:520-5. [Google Scholar] [PubMed]
- 9. Chow LT, Lee KC. Intraosseous lipoma. A clinicopathologic study of nine cases. Pathology 1992;24:219-22. [Google Scholar] [PubMed]
- 10. Greenspan A. Benign bone-forming lesions: Osteoma, osteoid osteoma, and osteoblastoma. Clin Imaging 1993;17:81-90. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Bizarre Parosteal Osteochondromatous Proliferation: A Case Series and Literature Review
July 1, 2026 Bizarre Parosteal Osteochondromatous Proliferation: A Case Series and Literature Review July 1, 2026 Correlation between Magnetic Resonance Imaging Modic Endplate Changes and Histopathological Inflammatory Activity in Lumbar Degenerative Disc Disease
July 1, 2026 Correlation between Magnetic Resonance Imaging Modic Endplate Changes and Histopathological Inflammatory Activity in Lumbar Degenerative Disc Disease June 1, 2026 Atypical Bilateral Cystic Foot Swellings with Osteomyelitis-Like Features: A Diagnostic Dilemma
June 1, 2026 Atypical Bilateral Cystic Foot Swellings with Osteomyelitis-Like Features: A Diagnostic Dilemma June 1, 2026 Hydatid Disease Masquerading as Infected Non-Union of Subtrochanteric Femur: A Rare Case Report
June 1, 2026 Hydatid Disease Masquerading as Infected Non-Union of Subtrochanteric Femur: A Rare Case Report