
Ceramic femoral heads fracture can occur, and recur, even in dual mobility hips when mechanical stresses are high.
Dr. Mohamad Khaled Ghannam, Department of Orthopaedic Surgery, Ramsay Sante, Hôpital Privé Jean Mermoz, Centre Orthopédique Santy, Lyon, France. E-mail: khaled.ghannam@hotmail.com
Abstract
Introduction: Ceramic femoral heads reduce wear in total hip arthroplasty (THA), yet fracture remains a rare but serious complication. Reports almost exclusively concern ceramic-on-ceramic bearings; cases in dual mobility constructs are exceptional. We describe, to our knowledge, the first report of two successive ceramic femoral head fractures occurring in the same dual mobility hip in a single patient, and we outline plausible mechanical contributors.
Case Report: Sixty-six-year-old White European man with no major comorbidities underwent primary THA with a dual mobility construct at another institution. Ten days later, he developed mechanical pain and audible noises without trauma; imaging demonstrated a ceramic femoral head fracture. Urgent revision replaced the acetabular component and femoral stem, and a new ceramic head was implanted; recovery was initially satisfactory. Twenty-two months later, during a torsional movement without high-energy trauma, he experienced sudden pain and functional impairment of the same hip. Imaging again confirmed a ceramic femoral head fracture. At re-revision, fragmented ceramic debris was found; the acetabular shell and the trunnion were intact and well fixed. The ceramic head was exchanged for a cobalt-chromium head with a compatible polyethylene insert, with extensive irrigation. Eight months later, he was pain-free with a full range of motion and returned to normal activities. The patient’s ethnic background was not recorded.
Conclusion: This case shows that dual mobility constructs are not immune to ceramic femoral head fracture and that recurrence is possible even with correct component positioning. The combination of increased femoral offset and an extended ceramic head, particularly in a patient with elevated body mass index, may raise stresses at the head–trunnion junction and precipitate failure. Clinicians should weigh patient and implant-related mechanical demands when selecting ceramic heads for dual mobility constructs and consider alternatives when risk appears high.
Keywords: Ceramic femoral head fracture, dual mobility hip arthroplasty, femoral offset, head–trunnion junction.
The introduction of ceramic materials in total hip arthroplasty (THA) has marked a significant advancement, notably by reducing wear and associated osteolysis due to the favorable mechanical and biological properties of this bioinert material [1,2]. Nevertheless, ceramic femoral heads are not without complications. The most frequently reported issues are noise phenomena known as squeaking and, more seriously, ceramic head fracture [1,3,4]. This risk is particularly well documented in ceramic-on-ceramic bearings and, to a lesser extent, in ceramic-on-polyethylene configurations, with only a few case reports documenting fractures [5,6,7,8]. To date, only one case of ceramic head fracture has been reported in the setting of a modular dual mobility THA (DM-THA) [9]. We report an unusual case involving two successive ceramic head fractures in a dual mobility hip implant in the same patient.
We present the case of a 66-year-old active male with no significant medical history and a body mass index (BMI) of 30.6 (176 cm height and 95 kg weight). He underwent right THA in 2018 for primary osteoarthritis at an outside institution, with an uncomplicated post-operative course. In July 2023, he underwent contralateral THA for the same indication, also performed in another institution. The implants used consisted of a 55 mm NOVAE® Sunfit TH acetabular shell combined with a size 11 CORAIL® High Offset 135° (DEPUY SYNTHES) collared femoral stem. The bearing surface included a 28 mm BIOLOX Delta® ceramic head (+8.5 mm head length) articulating with a polyethylene insert (outer diameter 55 mm, inner diameter 28 mm). The head was impacted into the polyethylene insert using a head–liner press provided by the manufacturer, which applies standardized force and has been used in multiple prosthetic implantations. The assembly was then impacted onto the taper in a standard manner. The taper was in a pristine condition. Post-operative radiographs were satisfactory (Fig. 1) and the early recovery was uneventful. On post-operative day 10, the patient presented to the emergency department of the same institution where the surgery was performed, reporting mechanical pain and audible noises from the operated hip, without any reported trauma or excessive rehabilitation. Radiographs revealed dissociation of the femoral head from the trunnion (Fig. 2).
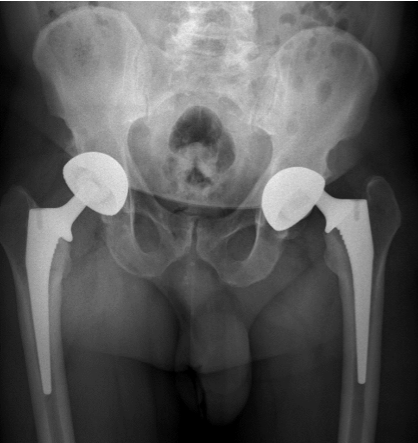
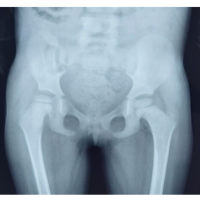
Figure 2: Radiographic evidence of femoral head dissociation from the trunnion at post-operative day 10. Anteroposterior pelvis radiograph at post-operative day 10 showing dissociation of the 28-mm ceramic head from the femoral trunnion, without traumatic history. The acetabular component remains in place.
An urgent revision surgery was performed. Intraoperatively, a ceramic head fracture was confirmed, along with taper damage and acetabular liner scratches from trunnion impingement. The acetabular component was revised to a 57 mm NOVAE® Sunfit TH, and the femoral stem to a size 12 CORAIL® KHO (DEPUY SYNTHES). A new 28 mm BIOLOX® Delta ceramic head (+8.5 mm) was implanted (Fig. 3). Head impaction was performed according to standard practice. The post-operative course was uneventful, and the patient showed satisfactory recovery at the 4-month follow-up. A 1-year follow-up was scheduled.

Figure 3: Post-operative radiograph following first revision surgery with complete implant exchange and reimplantation of a new ceramic head. Anteroposterior pelvis radiograph following urgent revision with exchange of the acetabular shell and femoral stem and implantation of a new 28-mm (+8.5 mm) ceramic head. Alignment and fixation are satisfactory, with no immediate complication detected.
However, 22 months post-operatively, the patient was referred to our institution for sudden hip pain and functional impairment of the left hip, occurring during a torsional trunk movement while the foot remained fixed. Radiographs revealed a second ceramic head fracture (Fig. 4). Revision surgery was planned to replace the head and insert, with intraoperative assessment of the acetabular shell and femoral stem.
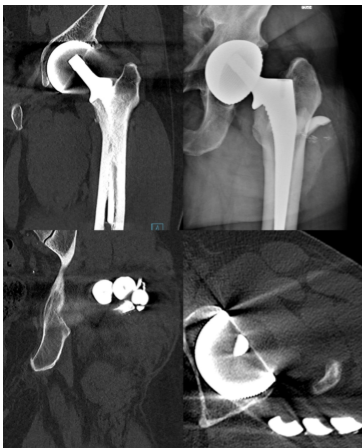
Figure 4: Radiograph and computed tomography-scan demonstrating the recurrent ceramic femoral head fracture 22 months after the initial revision surgery. Anteroposterior pelvis radiograph and computed tomography performed 22 months after the first revision, confirming a recurrent ceramic femoral head fracture after a low-energy torsional movement. No loosening of the acetabular shell or of the femoral stem is identified.
Revision surgery was performed, during which fragmented ceramic material was found (Fig. 5). There were no signs of damage to the acetabular shell or the trunnion, and both components remained well-fixed. The fractured ceramic head was replaced with a 28 mm cobalt-chromium head along with a compatible polyethylene insert (Fig. 6). A decision was made to change the type of prosthetic head bearing. 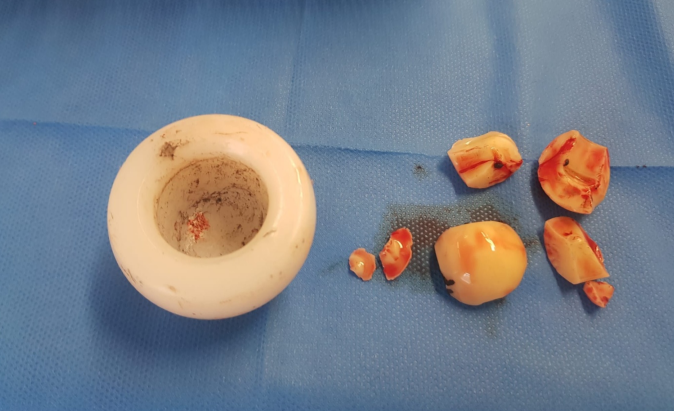
Figure 5: Intraoperative retrieval of fractured ceramic head fragments. Intraoperative image showing multiple fragments of the fractured ceramic femoral head retrieved during the second revision surgery.

Figure 6: Post-re-revision radiograph after exchange to cobalt chromium head and polyethylene insert. Post-operative radiograph after second revision surgery with replacement of fractured ceramic head by a 28 mm Cobalt-Chromium head and a compatible polyethylene insert.
Extensive irrigation of the joint space was performed to remove residual ceramic debris. Eight months after surgery, the patient demonstrated excellent functional recovery, with a clean and well-healed surgical incision, pain-free ambulation, return to normal activities, and full restoration of the revised hip range of motion.
Fracture of ceramic femoral heads remains one of the most feared complications in hip ceramic-on-ceramic arthroplasty. Although alumina offers excellent compressive strength, its tensile and flexural strength are relatively limited. Fracture rates with third-generation ceramics (BIOLOX® Forte) have been reported at approximately 0.021% [10]. To overcome the mechanical limitations of pure alumina, fourth-generation composite ceramic (BIOLOX® Delta) has been developed. These ceramics incorporate 17% zirconia, 0.6% strontium, and 0.3% chromium oxide, and have significantly reduced the incidence of fractures down to 0.003% according to the French National Agency for Safety of Drugs and Medical Products [9,10]. Beyond material composition, several risk factors for ceramic head fracture have been identified in the literature. Patient-related factors include elevated BMI, high activity levels, and trauma. Mechanical risk factors include the use of small (28 mm) heads, short neck lengths, manufacturing defects, or suboptimal implant positioning [7,11,12,13]. The type of bearing couple is also implicated; ceramic-on-polyethylene configurations appear to carry a lower risk than ceramic-on-ceramic [14]. One case of intraoperative ceramic head fracture has been reported during revision surgery, attributed to trunnion damage and component mismatch [15]. Fractures generally occur within the first 2 years following surgery [10]. However, delayed fractures without any history of trauma have been increasingly reported, raising the possibility of low-temperature degradation of zirconia in hybrid ceramic bearings [16,17]. However, this mechanism was not identified, and no fractures were reported in mid- to long-term follow-up in several series evaluating hybrid ceramic bearings [18,19]. The present case is notable in that the fracture occurred in a DM THA, a configuration not commonly associated with this complication, as in a conventional prosthesis. To our knowledge, no case series of ceramic head fractures in dual mobility implants has been published. Only one isolated case, described by Mickaël Patetta, involved a traumatic fracture occurring 4.5 years post-operatively [9]. It is noteworthy that, in this case, a modular dual mobility acetabular component was implanted. Modular dual mobility acetabular components are recognized for offering intraoperative flexibility and a theoretical reduction in the risk of post-operative instability [20,21]. Nevertheless, these advantages come with potential disadvantages, including mechanical issues, such as accelerated wear and fretting corrosion, as well as biological risks related to increased metal ion release and adverse local tissue reactions [21,22]. In contrast, the implant used in our case was a monoblock dual mobility cup. What makes our case particularly noteworthy is not only the use of a dual mobility constructs, but also the occurrence of two successive ceramic head fractures in the same hip. The first fracture occurred in the absence of any traumatic event, while the second followed a minor, low-energy incident. This unusual recurrence raises concerns about underlying mechanical or biomaterial-related factors that remain poorly understood in DM THA. Upon analyzing the potential contributing factors in our case, several classic causes can be excluded. The use of a short head length was not an issue, as both heads were +8.5 mm. A manufacturing defect seems unlikely to have affected two consecutive implants in the same patient. Component positioning was confirmed as satisfactory on CT scans. Moreover, no trunnion wear was observed intraoperatively, and compatibility between head and trunnion was confirmed. We hypothesize that the fracture of the ceramic head was caused by excessive mechanical stress at the head-trunnion interface, resulting from a significant increase in medio-lateral offset. This increase was due to the combined utilization of an extended femoral head (+8.5 mm) and a high-offset femoral stem in a patient presenting an elevated BMI. The impact of increased offset on the head–trunnion junction has previously been explored in the literature, with most studies indicating that greater medio-lateral offsets and extended neck moment arms correlate with elevated stress and increased taper damage at modular interfaces [23,24]. Del Balso et al., in their analysis of 56 retrieved femoral heads, documented greater trunnion corrosion and fretting damage predominantly affecting the central bore in cases involving elongated heads paired with high-offset stems [25]. Similarly, Martin et al. identified increased femoral offset as a primary factor significantly associated with elevated serum cobalt concentrations [26]. However, other studies have not validated these findings [27,28]. A biomechanical study would have been valuable to better understand the cause of the fracture. However, this is not feasible, as the ceramic head was fragmented into multiple small pieces. It is important to note that the majority of existing studies examining the effects of increased offset on taper performance primarily involve cobalt-chrome femoral heads. Few studies have specifically addressed the consequences of high offset in ceramic heads, which are known to exhibit lower fretting and corrosion rates compared to metal heads [29,30]. Indeed, Kurtz’s study, which analyzed fretting across various generations of ceramic components, found no direct correlation with increased femoral offset [30]. Given the conflicting data in the present literature, definitively confirming our hypothesis remains challenging. In this case, it appeared important to change the bearing of the prosthetic head for a metal head to avoid any risk of a third ceramic head fracture. Careful consideration should be given to implant selection in prosthetic surgery. While the patient has currently been followed for 8 months, this relatively short follow-up period can be considered a limitation. Continued follow-up is planned at 12 months after the past revision and at 24 months.
This case challenges the presumed mechanical reliability of ceramic femoral heads in dual mobility THA. The recurrence of ceramic head fracture within the same implant, occurring without major trauma and despite confirmed implant compatibility and correct positioning, highlights the potential biomechanical vulnerability of ceramic heads in the dual mobility context. The combination of a high-offset femoral stem, an extended ceramic head, and patient-specific risk factors, notably elevated BMI, may have resulted in excessive localized mechanical stress at the head–trunnion junction, precipitating these fractures. Given the rarity and severity of this complication, further biomechanical and clinical investigations specifically focusing on ceramic heads within dual mobility systems are warranted. Pending more definitive evidence, clinicians should carefully consider patient and implant-related factors before selecting ceramic heads for dual mobility constructs, particularly in scenarios with increased mechanical demand.
Dual mobility constructs do not eliminate the risk of ceramic head fracture. When using extended heads and high-offset stems in patients with elevated BMI, clinicians should consider the mechanical stresses imposed at the head–trunnion interface.
References
- 1. Hernigou P, Roubineau F, Bouthors C, Flouzat-Lachaniette CH. What every surgeon should know about Ceramic-on-Ceramic bearings in young patients. EFORT Open Rev 2016;1:107-11. [Google Scholar] [PubMed]
- 2. Santavirta S, Böhler M, Harris WH, Konttinen YT, Lappalainen R, Muratoglu O, et al. Alternative materials to improve total hip replacement tribology. Acta Orthop Scand 2003;74:380-8. [Google Scholar] [PubMed]
- 3. Abdelghafour KM, Jaques A, Shah N. Ceramic-on-ceramic bearings: Can we avoid the complications? Long-term outcomes of big head CoC bearings in primary total hip arthroplasty. Eur J Orthop Surg Traumatol 2025;35:80. [Google Scholar] [PubMed]
- 4. Alshammari MO, De Petrillo G, Epure LM, Huk OL, Zukor DJ, Antoniou J. Outcomes of ceramic-on-ceramic bearing total hip arthroplasty: A minimum 10-year follow-up study. J Arthroplasty 2023;38:S146-51. [Google Scholar] [PubMed]
- 5. Pawar ED, Yadav AK, Sharma A, Harsoor A. Ceramic liner fracture in ceramic on ceramic Total hip arthoplasty: A case report. Int J Surg Case Rep 2019;65:242-4. [Google Scholar] [PubMed]
- 6. Tucker D, Acharya M. Unusual prosthetic femoral head fracture in total hip arthroplasty: Ceramic on polyethylene articulation. BMJ Case Rep 2014;2014:bcr2013202685. [Google Scholar] [PubMed]
- 7. Heiner AD, Mahoney CR. Fracture of a BIOLOX delta ceramic femoral head articulating against a polyethylene liner: A case report. JBJS Case Connect 2014;4:e97. [Google Scholar] [PubMed]
- 8. Rankin CS, Robinson PG, Beattie N, Gaston P. Fracture of a BIOLOX delta ceramic femoral head: A case report and update of the literature. JBJS Case Connect 2019;9:e0336. [Google Scholar] [PubMed]
- 9. Patetta MJ, Kayupov E, Karam JA, Chmell SJ. Fourth-generation ceramic head fracture in dual mobility total hip arthroplasty: A case report. J Orthop Case Rep 2022;12:98-101. [Google Scholar] [PubMed]
- 10. Massin P, Lopes R, Masson B, Mainard D, French Hip and Knee Society (SFHG). Does biolox delta ceramic reduce the rate of component fractures in total hip replacement? Orthop Traumatol Surg Res 2014;100 6 Suppl:S317-21. [Google Scholar] [PubMed]
- 11. Michaud RJ, Rashad SY. Spontaneous fracture of the ceramic ball in a ceramic-polyethylene total hip arthroplasty. J Arthroplasty 1995;10:863-7. [Google Scholar] [PubMed]
- 12. Callaway GH, Flynn W, Ranawat CS, Sculco TP. Fracture of the femoral head after ceramic-on-polyethylene total hip arthroplasty. J Arthroplasty 1995;10:855-9. [Google Scholar] [PubMed]
- 13. Howard DP, Wall PD, Fernandez MA, Parsons H, Howard PW. Ceramic-on-ceramic bearing fractures in total hip arthroplasty: An analysis of data from the National Joint Registry. Bone Joint J 2017;99-B:1012-9. [Google Scholar] [PubMed]
- 14. Amanatullah DF, Landa J, Strauss EJ, Garino JP, Kim SH, Di Cesare PE. Comparison of surgical outcomes and implant wear between ceramic-ceramic and ceramic-polyethylene articulations in total hip arthroplasty. J Arthroplasty 2011;26 6 Suppl:72-7. [Google Scholar] [PubMed]
- 15. Dobria P, Patel A, Levine B. Catastrophic intraoperative failure of a ceramic femoral head. Arthroplast Today 2021;11:234-8. [Google Scholar] [PubMed]
- 16. Papaioannou I, Repantis T, Pantazidou G, Baikousis A, Korovessis P. Late onset atraumatic ceramic head fracture of a hybrid ceramic bearings total hip arthroplasty. Cureus 2021;13:e13726. [Google Scholar] [PubMed]
- 17. Hungerford M, Neubauer P, Boner A, Kowalewski A. Late atraumatic ceramic head fracture in total hip arthroplasty: A case report. J Orthop Case Rep 2023;13:65-8. [Google Scholar] [PubMed]
- 18. Yoo JI, Ha YC, Kim DH, Lee YK, Koo KH. Total hip arthroplasty using hybrid ceramic bearing: A minimum 10-year followup study. Indian J Orthop 2019;53:637-40. [Google Scholar] [PubMed]
- 19. Kang BJ, Ha YC, Hwang SC, Lee YK, Koo KH. Midterm results of large diameter Biolox forte ceramic head on delta ceramic liner articulation in total hip arthroplasty. J Arthroplasty 2014;29:2412-4. [Google Scholar] [PubMed]
- 20. Giovanoulis V, Koutserimpas C, Kenanidis E, Tsiridis E, Lustig S, Dubory A, et al. Modular versus monobloc dual mobility components for primary cementless total hip arthroplasty: A systematic review and meta-analysis of implants’ survival, complication rates, clinical and radiographic outcomes. Eur J Orthop Surg Traumatol 2024;35:7. [Google Scholar] [PubMed]
- 21. Minelli M, Kon E, D’Addona A, Rosolani M, Di Matteo B, Della Rocca F. Minimum five years outcomes of modular dual mobility in primary total hip arthroplasty: A systematic review. Int Orthop 2025;49:1699-707. [Google Scholar] [PubMed]
- 22. Parikh N, Lam AD, Waren D, Hobbs J, Pipa D, Schwarzkopf R, et al. Serum metal ion levels in modular dual mobility liners after total hip arthroplasty: A comparison by years and implant manufacturers. J Arthroplasty 2025;40:2922-9. [Google Scholar] [PubMed]
- 23. Dutta A, Nutt J, Slater G, Ahmed S. Review: Trunnionosis leading to modular femoral head dissociation. J Orthop 2021;23:199-202. [Google Scholar] [PubMed]
- 24. Higgs GB, Hanzlik JA, MacDonald DW, Gilbert JL, Rimnac CM, Kurtz SM, et al. Is increased modularity associated with increased fretting and corrosion damage in metal-on-metal total hip arthroplasty devices?: A retrieval study. J Arthroplasty 2013;28 8 Suppl:2-6. [Google Scholar] [PubMed]
- 25. Del Balso C, Teeter MG, Tan SC, Lanting BA, Howard JL. Taperosis: Does head length affect fretting and corrosion in total hip arthroplasty? Bone Joint J 2015;97-B:911-6. [Google Scholar] [PubMed]
- 26. Martin JR, Camp CL, Wyles CC, Taunton MJ, Trousdale RT, Lewallen DG. Increased femoral head offset is associated with elevated metal ions in asymptomatic patients with metal-on-polyethylene total hip arthroplasty. J Arthroplasty 2016;31:2814-8. [Google Scholar] [PubMed]
- 27. Lanting BA, Wood TJ, Young S, Van Citters DW, MacDonald SJ, Howard JL, et al. The effect of altering head length on corrosion using a material loss method. Hip Int 2019;29:368-72. [Google Scholar] [PubMed]
- 28. Valente G, Lanting B, MacDonald S, Teeter MG, Van Citters D, Howard J. Femoral head material loss at the head-neck junction in total hip arthroplasty: The effect of head size, stem material and stem offset. Hip Int 2019;29:647-51. [Google Scholar] [PubMed]
- 29. Hallab NJ, Messina C, Skipor A, Jacobs JJ. Differences in the fretting corrosion of metal-metal and ceramic-metal modular junctions of total hip replacements. J Orthop Res 2004;22:250-9. [Google Scholar] [PubMed]
- 30. Kurtz SM, Kocagöz SB, Hanzlik JA, Underwood RJ, Gilbert JL, MacDonald DW, et al. Do ceramic femoral heads reduce taper fretting corrosion in hip arthroplasty? A retrieval study. Clin Orthop Relat Res 2013;471:3270-82. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 November 10, 2021 Freeman-Sheldon Syndrome with Stiff Knee Gait – A Case Report
November 10, 2021 Freeman-Sheldon Syndrome with Stiff Knee Gait – A Case Report September 1, 2025 Neglected Isolated Lunate Dislocation in a Polytrauma Patient Presenting as Acute Carpal Tunnel Syndrome – A Case Report with Review of Literature
September 1, 2025 Neglected Isolated Lunate Dislocation in a Polytrauma Patient Presenting as Acute Carpal Tunnel Syndrome – A Case Report with Review of Literature April 14, 2013 Decreasing Complications of Quadricepsplasty for Knee Contracture after Femoral Fracture Treatment with an External Fixator; Report of Four Cases – A Response
April 14, 2013 Decreasing Complications of Quadricepsplasty for Knee Contracture after Femoral Fracture Treatment with an External Fixator; Report of Four Cases – A Response- January 10, 2021 Diagnosis and Arthroscopic Treatment of Synovial Chondromatosis of Glenohumeral Joint: A Case Report