
V-Y Quadricepsplasty in Total knee arthroplasty for ankylosed flexion knees in a patient with rheumatoid arthritis.
Dr. Florent Francony, Department of Orthopedic and Trauma Surgery, CH Métropole Savoie, Chambéry, Cedex, France. E-mail: dr.francony@gmail.com
Abstract
Introduction: Total knee arthroplasty (TKA) in ankylosed knees with patella baja represents a major surgical challenge, especially in rheumatoid arthritis (RA) patients. Adequate exposure is critical and may require extensile approaches.
Case Report: We report the case of a 64-year-old female with long-standing RA and bilateral knee ankylosis in 40° flexion. She underwent bilateral TKA with V-Y quadricepsplasty, which allowed satisfactory patellar mobilization and exposure. Postoperatively, she regained full extension and 90° of flexion at 6 months without extensor lag or complications.
Conclusion: V-Y quadricepsplasty is a reliable and safe option for surgical exposure in TKA for ankylosed knees with patella baja, avoiding the risks associated with tibial tubercle osteotomy, particularly in patients with fragile bone quality due to RA.
Keywords: Total knee arthroplasty, rheumatoid arthritis, ankylosed knee, V-Y quadricepsplasty, tibial tubercle osteotomy.
Rheumatoid arthritis (RA) can cause severe joint destruction, stiffness, and ankylosis of the knee [1]. Performing a total knee arthroplasty (TKA) in this setting is technically demanding, especially when the knee is ankylosed in flexion [2]. Adequate surgical exposure is often the most critical step. Several extensile techniques have been described, including the quadriceps snip [3], tibial tubercle osteotomy (TTO) [4], and V-Y quadricepsplasty [5]. We report a case of bilateral TKA using a V-Y quadricepsplasty to facilitate exposure, and we compare the benefits and risks of this technique with TTO.
A 64-year-old female with a long-standing history of RA presented with bilateral knee ankylosis fixed in 40° of flexion, irreducible and painful. Functional disability was severe, rendering standing and walking impossible and leading to continuous bed confinement (Fig. 1).
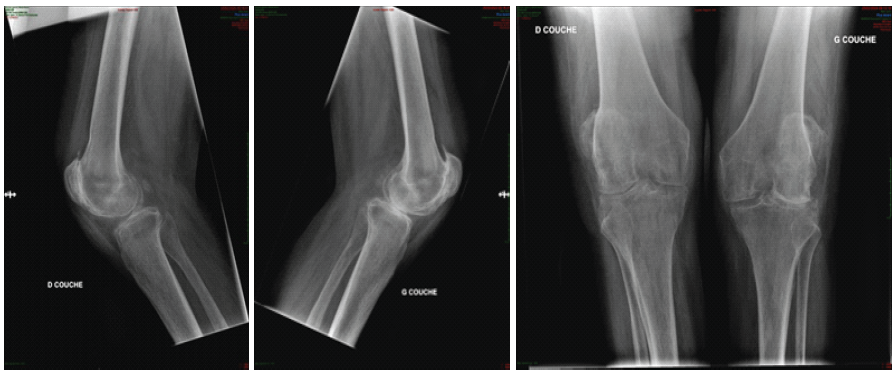
Figure 1: Pre-operative X-ray.
Surgical technique
Bilateral TKA was performed. A V-Y quadricepsplasty was carried out on both sides. This maneuver allowed mobilization of the patellae and satisfactory access to the joint surfaces. Postoperatively, full weight-bearing was authorized under bilateral hinged braces, locked at 0–45° for the 1st month, then 0–90° for the following month.
Outcomes
The post-operative course was satisfactory: the patient regained full extension and 90° of flexion at 6 months, without extensor lag or wound complications. She recovered independent ambulation with the use of canes at 1 year (Fig. 2).
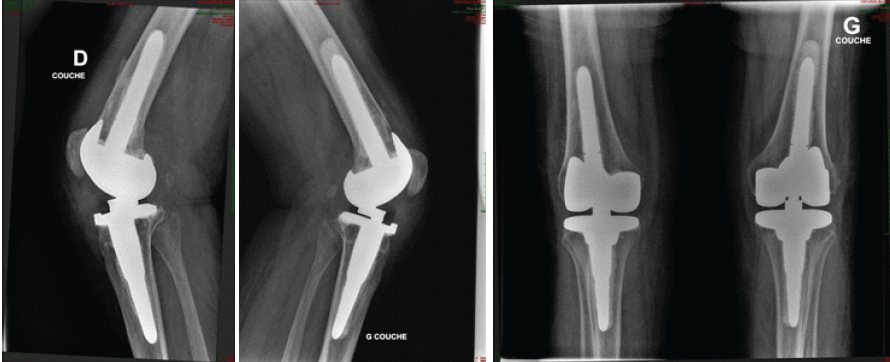
Figure 2: Post-operative X-ray.
Adequate exposure is a major challenge in TKA for stiff or ankylosed knees [2,6]. Forceful patellar eversion may cause extensor mechanism rupture, patellar tendon avulsion, or malpositioning of components. Extensile approaches are therefore recommended. The V-Y quadricepsplasty, first described by Coonse and Adams [7], lengthens the quadriceps tendon and facilitates patellar mobilization. It is particularly useful in cases with severe quadriceps contracture and patella baja [5,8]. Molina et al. [9] demonstrated that this technique provides safe exposure in stiff knees undergoing TKA without significantly increasing complication rates. Potential drawbacks include transient extensor weakness and delayed tendon healing [10]. Previous studies suggest that extensile approaches such as V-Y quadricepsplasty do not necessarily compromise post-operative quadriceps function. Trousdale et al. [11] reported no significant differences in isokinetic knee strength between knees undergoing TKA with V-Y quadricepsplasty and either the contralateral knees treated without an extensile approach or age-matched controls undergoing a standard medial parapatellar arthrotomy. Likewise, Zhamilov et al. [12], in a comparative cohort study, found no significant differences between quadriceps snip and V-Y quadricepsplasty with respect to extensor lag, flexor and extensor muscle strength, or functional outcome scores. TTO, described by Whiteside and Ohl [4], also provides excellent exposure [13]. However, it carries risks of non-union, tibial fracture, or migration [14], which are accentuated in RA patients with poor bone quality. In our patient, bilateral V-Y quadricepsplasties were preferred over TTO to avoid osteotomy-related complications. The post-operative outcome confirmed the benefit of this choice, with good functional recovery and no extensor deficit. Thus, V-Y quadricepsplasty represents a valuable and safe option for complex TKA in ankylosed knees.
V-Y quadricepsplasty is a safe and effective technique for improving exposure in bilateral TKA for ankylosed flexion knees, particularly in RA patients. It avoids the complications of TTO while ensuring satisfactory surgical access.
In patients with ankylosed knees, V-Y quadricepsplasty provides reliable exposure for TKA, reducing the need for tibial tubercle osteotomy and its associated risks, especially in rheumatoid arthritis patients with fragile bone.
References
- 1. Insall JN, Scott WN. Surgery of the Knee. 5th ed. Philadelphia, PA: Elsevier; 2012. [Google Scholar] [PubMed]
- 2. Rand JA. Extensile exposures for difficult total knee arthroplasty. J Arthroplasty 1990;5 Suppl:S21-6. [Google Scholar] [PubMed]
- 3. Vince KG, Insall JN, Kelly MA. The quadriceps snip for difficult exposure in total knee arthroplasty. J Bone Joint Surg Br 1989;71:837-40. [Google Scholar] [PubMed]
- 4. Whiteside LA, Ohl MD. Tibial tubercle osteotomy for exposure of the difficult total knee arthroplasty. Clin Orthop Relat Res 1990;260:6-9. [Google Scholar] [PubMed]
- 5. Keblish PA, Varma AK, Greenwald AS. Quadriceps V-Y turndown technique for exposure of the difficult total knee arthroplasty. Clin Orthop Relat Res 1991;260:203-8. [Google Scholar] [PubMed]
- 6. Trousdale RT, Pagnano MW. Extensile exposures in revision total knee arthroplasty. Clin Orthop Relat Res 2004;427:131-8. [Google Scholar] [PubMed]
- 7. Coonse WG, Adams JD. A new operative approach to the knee joint. Surg Gynecol Obstet 1943;77:344-9. [Google Scholar] [PubMed]
- 8. Buechel FF, Pappas MJ. Exposure of the difficult total knee arthroplasty. Orthop Clin North Am 1989;20:227-38. [Google Scholar] [PubMed]
- 9. Molina V, Casabianca L, Lambert T, Vincent C, Court C. Intérêt de la plastie en V-Y du quadriceps dans les PTG sur genou raide. Rev Chir Orthop Traumatol 2013;99:S358. [Google Scholar] [PubMed]
- 10. Dalury DF. Extensile exposures for revision total knee arthroplasty. J Arthroplasty 2013;28:729-34. [Google Scholar] [PubMed]
- 11. Trousdale RT, Hanssen AD, Rand JA, Cahalan TD. V-Y quadricepsplasty in total knee arthroplasty. Clin Orthop Relat Res 1993;286:48-55. [Google Scholar] [PubMed]
- 12. Zhamilov V, Karatosun V, Kalkan S, Unver B, Gunal I. Evaluation of extensor mechanism in revision knee arthroplasty. J Arthroplasty 2017;32:2484-6. [Google Scholar] [PubMed]
- 13. Rosenberg AG, Berger RA, Barden RM, Sheinkop MB, Jacobs JJ, Galante JO. Osteotomy of the tibial tubercle during total knee arthroplasty. J Bone Joint Surg Am 1993;75:940-8. [Google Scholar] [PubMed]
- 14. Barrack RL, Smith P, Munn B, Engh G, Rorabeck C. Comparison of surgical approaches in total knee arthroplasty. Clin Orthop Relat Res 1998;356:16-21. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2025 A Case Report on the Management of Peri-Prosthetic Fracture in a Post-TKA Patient with Rheumatoid Arthritis: Surgical Strategy and Treatment Outcome
June 1, 2025 A Case Report on the Management of Peri-Prosthetic Fracture in a Post-TKA Patient with Rheumatoid Arthritis: Surgical Strategy and Treatment Outcome June 10, 2024 V-Y Quadricepsplasty for Knee Stiffness Post Total Knee Arthroplasty: A Case Report and Literature Review
June 10, 2024 V-Y Quadricepsplasty for Knee Stiffness Post Total Knee Arthroplasty: A Case Report and Literature Review June 1, 2026 Efficacy of Tranexamic Acid in Reducing Blood Loss and Transfusion Requirements in Primary Total Knee Arthroplasty: A Prospective Comparative Study
June 1, 2026 Efficacy of Tranexamic Acid in Reducing Blood Loss and Transfusion Requirements in Primary Total Knee Arthroplasty: A Prospective Comparative Study June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty
June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty