
Symptomatic scapular body non-union, though rare, should be considered in patients with chronic shoulder pain after conservative fracture treatment. A modified posterior midline approach enables safe dual-plate fixation with limited muscle detachment and reliable restoration of scapular stability and function.
Dr. Sai Surya Dinesh Pydi, Department of Orthopaedics, Post Graduate Institute of Medical Education and Research, PGIMER, Chandigarh. E-mail: saisuryadinesh111@gmail.com
Abstract
Introduction: Scapular fractures are rare and usually unite with conservative treatment. Symptomatic non-union of the scapular body is exceptionally uncommon and can lead to chronic pain and functional limitation.
Case Report: A 42-year-old female with a right scapular body fracture initially treated non-operatively developed persistent posterior shoulder pain and radiographic non-union at 1 year. She underwent open reduction and internal fixation using a modified posterior midline approach with dual 3.5-mm reconstruction plates and autologous iliac crest cancellous bone grafting.
Conclusion: Solid union was achieved in 3 months, and the patient regained full, pain-free shoulder function at 1 year. A modified posterior approach allows dual-border exposure through a single incision with limited soft-tissue disruption, enabling stable fixation and excellent clinical outcome in scapular body non-union.
Keywords: Scapular body, non-union, modified posterior approach, open reduction internal fixation, dual plating, shoulder girdle.
Scapular fractures account for <1% of all fractures and approximately 3–5% of shoulder-girdle injuries [1,2]. They typically result from high-energy trauma such as motor-vehicle collisions, falls, or direct blows [3,4]. The scapula’s rich vascularity, cancellous structure, and muscular envelope contribute to its high rate of healing, and most fractures unite with conservative management [5,6]. Non-union of the scapular body is therefore an exceptionally rare entity, with only a few cases described in the literature [7,8,9,10]. When it occurs, patients present with chronic pain, crepitus, or fatigue during overhead activity, often long after the initial trauma. Radiological evaluation is essential to confirm the diagnosis and define the extent and configuration of non-union [8,9]. Despite this, certain cases fail to unite and may require surgical intervention. Surgical treatment is indicated for symptomatic non-union or persistent pain following failed conservative management. The key principles include meticulous debridement, autologous bone grafting, and rigid fixation. Traditional exposures, such as the Judet posterior approach, provide broad visualization but require extensive detachment of the deltoid and infraspinatus [10,11,12]. In contrast, a modified posterior approach – as used in this case – provides simultaneous access to both the lateral and vertebral borders through a single incision while preserving soft-tissue attachments. To our knowledge, no previous report has described this exposure for the fixation of scapular body fractures or non-union. This case demonstrates successful union of a rare scapular body non-union using dual-plate fixation through a modified posterior approach, emphasizing diagnostic vigilance and the advantages of limited yet versatile exposure.
A 42-year-old right-hand-dominant female sustained a right scapular body fracture after a high-energy road-traffic accident. The patient was evaluated and stabilized according to Advanced Trauma Life Support protocols. Initial shoulder radiographs demonstrated a minimally displaced extra-articular scapular body fracture without glenoid involvement. In keeping with standard management guidelines, she was treated conservatively in a sling for 6 weeks, followed by supervised physiotherapy. At 1 year, the patient reported persistent posterior shoulder pain and fatigue during overhead activity. Examination revealed focal tenderness over the scapular body and pain beyond 100° of abduction, though overall range of motion was preserved. Radiographs confirmed a fibrous non-union of the scapular body with minimal displacement (Fig. 1). Given the need to access both the lateral and vertebral borders for stable dual-plate fixation, a modified posterior approach was selected. This approach was chosen to permit dual-border exposure through a single incision while preserving muscular attachments.
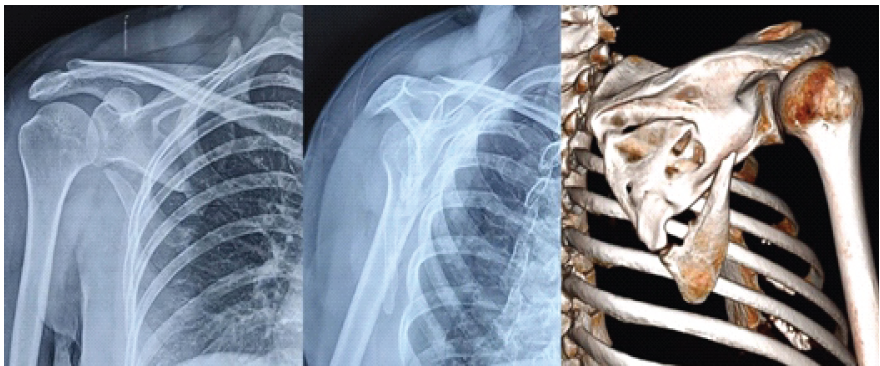
Figure 1: Radiograph showing scapular body non-union 1 year after injury.
Under general anesthesia, the patient was positioned in the lateral decubitus position on a radiolucent table with the arm abducted to approximately 70° and gently externally rotated to relax the posterior deltoid, infraspinatus, and teres minor. All bony prominences were padded, and the shoulder and iliac crest were prepared and draped.
A longitudinal incision was made along the midline of the scapula, extending from the spine of the acromion to the inferior angle. Full-thickness skin flaps were raised medially and laterally to expose the trapezial fascia. The trapezius muscle was detached subperiosteally from the spine of the scapula and retracted medially with Langenbeck retractors, preserving its acromial insertion. The deltoid fascia was incised along the lateral scapular spine and reflected laterally, maintaining continuity with the deltoid muscle to prevent devascularization. The interval between the infraspinatus and teres minor (Fig. 2) was identified and developed bluntly with a peanut dissector, providing a safe and direct approach to the lateral border while avoiding the axillary nerve inferiorly and suprascapular nerve superiorly. During dissection along the lateral border, the circumflex scapular artery was carefully mobilized, double-clipped, and divided to prevent inadvertent bleeding and to allow safe retraction of the teres minor and exposure of the lateral scapular border.
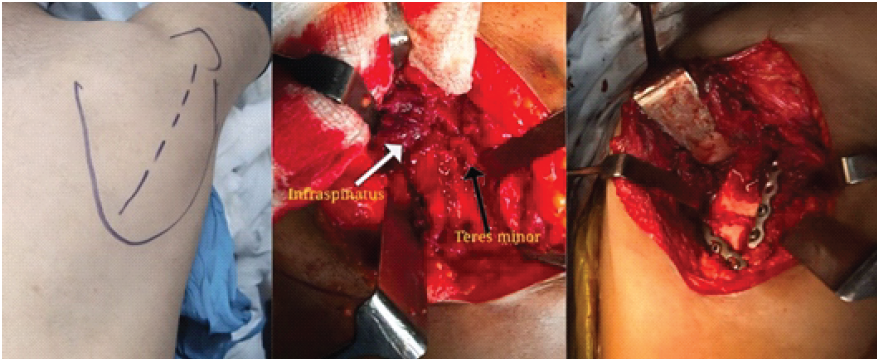
Figure 2: Intraoperative photographs illustrating the posterior midline approach.
The infraspinatus was gently retracted superomedially and the teres minor inferolaterally, exposing the lateral border and body of the scapula. A separate subperiosteal plane was created beneath the infraspinatus medially, allowing exposure of the vertebral border for plate placement. Broad, gentle retraction minimized muscle strain and preserved perfusion. At the non-union site, fibrous tissue and sclerotic bone were excised until fresh bleeding cancellous bone was encountered. The fragments were mobilized and anatomically reduced. A pointed Verbrugge bone clamp was applied across the fracture – one jaw along the lateral border and the other on the vertebral fragment – providing compression while maintaining alignment. Temporary fixation was confirmed both visually and fluoroscopically. An autologous cancellous bone graft harvested from the ipsilateral iliac crest was packed into the defect. Fixation was achieved using two contoured 3.5-mm reconstruction plates: one along the lateral border to resist bending and shear, and another along the vertebral border to restore the scapular ring and resist torsional forces [10]. Screws were tightened sequentially to maintain compression across the fracture, and fluoroscopy confirmed satisfactory alignment and fixation. After irrigation, hemostasis, and drain placement, the infraspinatus and teres minor were reapproximated with absorbable sutures to restore the posterior envelope. The deltoid fascia was closed anatomically, followed by layered closure of subcutaneous tissue and skin. Postoperatively, the shoulder was immobilized in a sling for 3 weeks. Pendulum exercises were initiated thereafter, progressing to active-assisted and active motion at 6 weeks. At 3 months, radiographs confirmed solid union with resolution of pain (Fig. 3). At 1 year, the patient was pain-free, had full shoulder motion (abduction 170°, external rotation 70°, and internal rotation to the level of T8), and had returned to all pre-injury activities (Fig. 4).
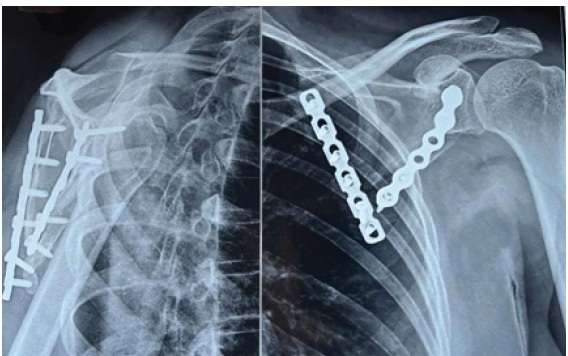
Figure 3: Post-operative radiograph at 3 months showing solid union with dual-plate fixation.
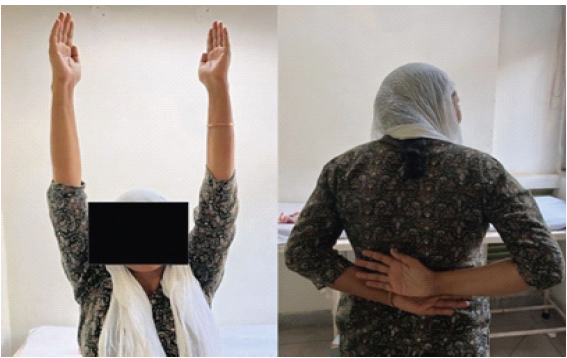
Figure 4: Clinical image at 1 year demonstrating full shoulder motion and functional recovery.
Scapular body non-union is among the rarest complications of shoulder-girdle trauma due to the scapula’s excellent vascularity and muscular protection [3,4,5,6]. Fewer than 10 such cases have been reported, most following conservative management of minimally displaced fractures [7,8,9,10,13,14]. The rarity of this condition and its subtle presentation make diagnosis challenging, and persistent shoulder pain after apparent fracture healing should prompt radiological evaluation to rule out non-union. Previous reports describe similar presentations with chronic pain, localized tenderness, and preserved but painful motion. Michael et al. [7] treated a scapular body non-union with open reduction and bone grafting, achieving full motion at 6 months. Ferraz et al.[8] reported a similar case managed with autologous grafting and obtained excellent recovery. Gupta et al.[12] and Marek et al.[9] likewise achieved solid union after rigid fixation and grafting. Collectively, these studies reinforce the importance of rigid fixation and biological augmentation for successful outcomes.
In the present case, the non-union was attributed to the interposition of the subscapularis muscle between the fracture fragments, which prevented cortical contact and created a mechanical barrier to healing despite otherwise favorable biological conditions. Soft-tissue interposition is uncommon in scapular fractures but represents a recognized cause of persistent non-union when the initial displacement is underestimated or not adequately reduced. The modified posterior approach used in this case offers distinct advantages. Unlike the extensile Judet approach, which often necessitates wide detachment of the deltoid and infraspinatus muscles, the midline incision from the acromion to the inferior angle permits elevation of full-thickness flaps and subperiosteal access to both borders through a single exposure. Developing the interval between the infraspinatus and teres minor provides safe access to both surfaces, enabling dual-plate fixation while preserving muscle insertions and minimizing morbidity. Our construct employed two contoured 3.5-mm reconstruction plates, one along the lateral and one along the vertebral border, restoring scapular ring integrity and neutralizing multidirectional forces, consistent with Marek et al.[9] The use of autologous bone graft enhanced osteogenesis. This construct permitted early mobilization without loss of fixation, leading to rapid union and complete recovery. A summary of reported cases of scapular body non-union is presented in Table 1. This case adds to the limited literature on scapular body non-union in two important ways. First, it describes a modified posterior approach, a reproducible exposure allowing dual-border fixation with minimal dissection. Second, it demonstrates that even chronic scapular body non-union can unite successfully when biological and mechanical principles are respected.
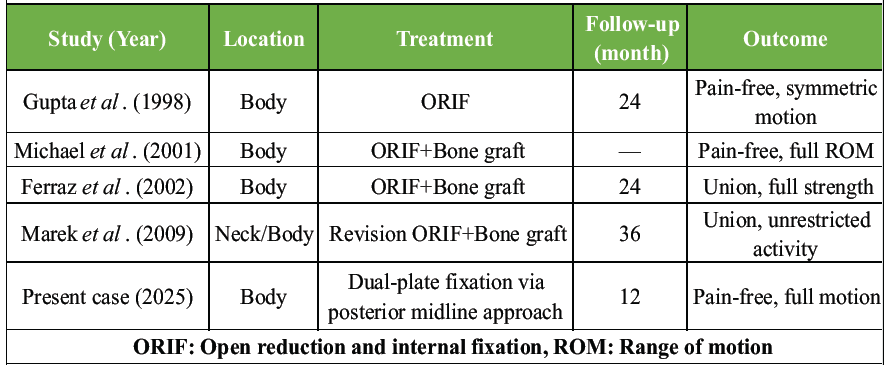
Table 1: Reported cases of scapular body non-union
Beyond its rarity, this case underscores the importance of maintaining diagnostic vigilance in patients with unresolved scapular pain and highlights how precise surgical planning and tissue-sparing exposure can yield reliable union and excellent function. For orthopedic surgeons, it exemplifies how innovation within established principles can minimize morbidity and optimize recovery in rare and challenging injuries.
Scapular body non-union is an exceptionally rare but clinically significant cause of persistent shoulder pain following conservative management of minimally displaced fractures. A high index of suspicion is required in patients with ongoing symptoms despite apparent radiological healing. Meticulous debridement, autologous bone grafting, and rigid dual-plate fixation can reliably achieve union and restore function. The modified posterior approach described in this report provides safe and versatile exposure to both the lateral and vertebral borders through a single incision while preserving soft tissues. Respecting biological and mechanical principles remains the cornerstone of successful management in these uncommon injuries.
Persistent posterior shoulder pain following a conservatively treated scapular fracture should prompt evaluation for non-union. When symptomatic non-union is identified, rigid fixation combined with autologous bone grafting provides predictable union. A modified posterior approach allows dual-border fixation with minimal soft-tissue disruption and excellent functional outcomes.
References
- 1. Court-Brown CM, Aitken SA, Forward DP, Clement ND, Duckworth AD, McQueen MM, et al. Rockwood and Green’s Fractures in Adults. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010. [Google Scholar] [PubMed]
- 2. Rowe CR. Fractures of the scapula. Surg Clin North Am 1963;43:1565-71. [Google Scholar] [PubMed]
- 3. Goss TP. Scapular fractures and dislocations: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:22-33. [Google Scholar] [PubMed]
- 4. Zlowodzki M, Bhandari M, Zelle BA, Kregor PJ, Cole PA. Treatment of scapula fractures: Systematic review of 520 fractures in 22 case series. J Orthop Trauma 2006;20:230-3. [Google Scholar] [PubMed]
- 5. Schofer MD, Sehrt AC, Timmesfeld N, Störmer S, Kortmann HR. Fractures of the scapula: Long-term results after conservative treatment. Arch Orthop Trauma Surg 2009;129:1511-9. [Google Scholar] [PubMed]
- 6. Cole PA, Freeman G, Dubin JR. Scapula fractures. Curr Rev Musculoskelet Med 2013;6:79-87. [Google Scholar] [PubMed]
- 7. Michael D, Fazal MA, Cohen B. Nonunion of a fracture of the body of the scapula: Case report and literature review. J Shoulder Elbow Surg 2001;10:385-6. [Google Scholar] [PubMed]
- 8. Ferraz IC, Papadimitriou NG, Sotereanos DG. Scapular body nonunion: A case report. J Shoulder Elbow Surg 2002;11:98-100. [Google Scholar] [PubMed]
- 9. Marek DJ, Sechriest VF 2nd, Swiontkowski MF, Cole PA. Case report: Reconstruction of a recalcitrant scapular neck nonunion and literature review. Clin Orthop Relat Res 2009;467:1370-6. [Google Scholar] [PubMed]
- 10. Judet R, Judet J. Fractures of the scapula. Acta Orthop Belg 1987;53:143-9. [Google Scholar] [PubMed]
- 11. Rowe CR, Yee L. A posterior approach to the shoulder joint. J Bone Joint Surg Am 1944;26:111-5. [Google Scholar] [PubMed]
- 12. Gupta R, Sher J, Williams GR Jr., Iannotti JP. Nonunion of the scapular body. J Bone Joint Surg Am 1998;80:428-30. [Google Scholar] [PubMed]
- 13. Hardegger FH, Simpson LA, Weber BG. The operative treatment of scapular fractures. J Bone Joint Surg Br 1984;66:725-31. [Google Scholar] [PubMed]
- 14. Matsuo T, Yoshikawa K, Oki S, Takeuchi D. Reconstruction surgery of intra-articular scapular fracture nonunion. JSES Rev Rep Tech 2022;2:68-74. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Surgical Treatment of a Non-union of Medial End Clavicle Fracture with Dual Plating and its Clinical Outcome – A Case Report
October 1, 2025 Surgical Treatment of a Non-union of Medial End Clavicle Fracture with Dual Plating and its Clinical Outcome – A Case Report October 1, 2024 Neglected Ipsilateral Non-Union Neck of Femur with Shaft of Femur Non-Union in A Young Patient and Its Management – A Rare Case Report
October 1, 2024 Neglected Ipsilateral Non-Union Neck of Femur with Shaft of Femur Non-Union in A Young Patient and Its Management – A Rare Case Report July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report
July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report July 1, 2026 Three-column Plating for Complex Tibial Plateau Fractures: Multivariate Predictors of Superior Functional Recovery
July 1, 2026 Three-column Plating for Complex Tibial Plateau Fractures: Multivariate Predictors of Superior Functional Recovery