
The Eden-Hybinette procedure is an effective salvage technique for recurrent instability following failed Latarjet surgery with significant glenoid bone loss.
Dr. Suyog Wagh, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India. E-mail: suyogwagh6159@gmail.com
Abstract
Introduction: Anterior shoulder instability commonly affects young, active individuals and is often associated with traumatic dislocations and glenoid bone loss. The Latarjet procedure is widely performed in cases with significant bone loss, providing stability through coracoid transfer, the sling effect of the conjoint tendon, and capsulolabral repair. Despite its success, complications such as malpositioned bone block, hardware failure, graft resorption or non-union, and patient-related factors like laxity or inadequate rehabilitation may lead to recurrence. Revision surgery after failed Latarjet remains challenging, and no universal consensus exists regarding the optimal approach. The Eden-Hybinette procedure, using a tricortical iliac crest graft, is an accepted salvage option when the coracoid is non-viable.
Case Report: A 38-year-old male presented with recurrent right shoulder instability after undergoing a Latarjet procedure 4 years earlier. Instability recurred within 1 year, and the patient sustained multiple dislocations over the next 3 years. Clinical examination revealed anterior instability with a Beighton score of five. Imaging showed screw breakage with approximately 27% glenoid bone loss. Revision surgery was performed with the Eden-Hybinette technique. A tricortical iliac crest graft was harvested and secured to the glenoid with three cannulated screws. Post-operative recovery was uneventful. By 3 months, the patient had regained a full range of motion, and computed tomography at 6 months demonstrated complete graft union.
Conclusion: This case highlights the importance of individualized surgical planning in managing recurrent instability following a failed Latarjet procedure. The Eden-Hybinette technique provided reliable restoration of glenoid architecture and stability, achieving both favorable functional recovery and radiological union in this patient.
Keywords: Shoulder instability, Latarjet failure, Eden-Hybinette procedure, glenoid bone loss, iliac crest graft.
Anterior shoulder instability is a common condition, particularly among young and active individuals. It often results from a traumatic dislocation in susceptible individuals and is either a soft tissue or osseous defect of the glenoid and/or humeral head. Depending on the extent of bone loss, various treatment options are available. When glenoid bone loss exceeds 20%, a bony reconstruction procedure like Latarjet is typically recommended [1]. It involves transfer of the coracoid process to the antero-inferior part of glenoid and provides a three-way mechanism of stabilization; bony augmentation, sling effect of the conjoint tendon and capsulolabral repair. Despite its safety and efficacy, failure rates range from 7.5% to 14% with high prevalence in the 1st post-operative year [2].
Several factors have been reported as potential contributors to failure, including an incorrect diagnosis, malpositioned bone blocks or hardware, unrecognized associated lesions, graft resorption, non-union, coracoid migration, overly aggressive or improper rehabilitation, joint laxity, and new traumatic events [3]. Recent literature has highlighted a growing trend toward individualized management strategies for failed Latarjet surgeries, yet consensus on the optimal revision approach remains limited. One such salvage procedure is the Eden-Hybinette technique, which involves anatomical reconstruction of the glenoid using an autologous iliac crest. This technique addresses bone loss directly and has shown favorable outcomes, particularly when the coracoid graft is absent or non-viable [4]. However, this procedure does not come without limitations. Autograt harvesting from the iliac crest can be associated with donor site morbidity, including pain, hematoma, or infection. In addition, graft resorption and non-union remain concerns, particularly in cases with inadequate fixation or poor vascularization. Fixation methods-such as screws or cortical buttons-also present technical challenges, and complications like hardware loosening or intra-articular graft positioning may compromise outcomes [5].
In this report, we present a case of failed Latarjet surgery managed successfully with Eden-Hybinette procedure, demonstrating favorable post-operative outcomes and no complications during follow-up.
A 38-year-old male with a history of right shoulder instability in the past was managed with the Latarjet procedure 4 years ago. The patient had an uneventful post-surgical period, but symptoms recurred a year later without any significant event. He presented to us with complaints of right shoulder pain and instability since 3 years, having experienced multiple episodes of dislocations, which were managed with closed reduction at different centers. On examination, the Beighton score was five. 1 cm wasting was noted in the right arm. Sensations over the arm were intact. Tests for anterior instability, such as apprehension, relocation-release, and anterior drawer, were positive. There were no signs of instability in posterior and inferior directions. He had a nearly complete range of motion in all planes but was apprehensive to use the arm for overhead activities and lifting heavy objects. X-ray and computed tomography (CT) scan were done, which revealed a displaced as well as a broken screw near the right glenoid, likely from the previous surgery (Fig. 1 and 2). The anteroinferior part of the glenoid appeared to be resorbed. Bone loss was quantified using the perfect circle method in oblique sagittal plane, which was approximately 27% (Fig. 3). Infective etiology was ruled out via clinical examination and radiological investigations.
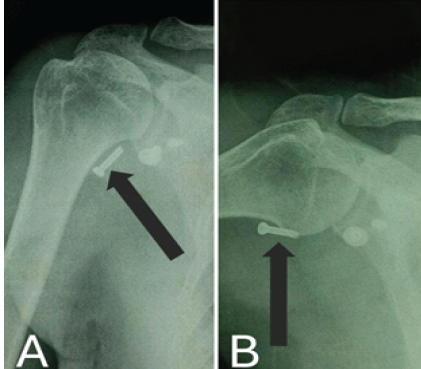
Figure 1: X-ray on presentation. (a) Anteroposterior X-ray in 10° abduction, (b) Anteroposterior X-ray in 60° abduction, both showing a displaced screw in soft-tissue marked with a black arrow.
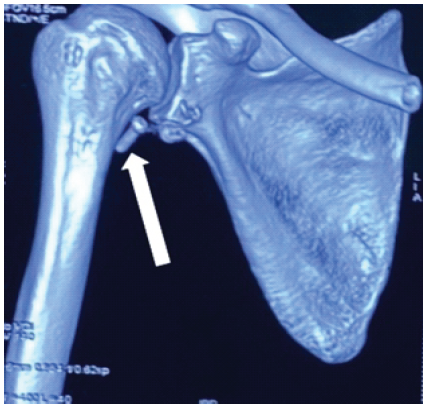
Figure 2: Computed tomography scan showing resorbed glenoid bone and a displaced screw marked with a white arrow.

Figure 3: Oblique sagittal view in computed tomography scan showing approximately 27% bone loss.
We managed the case with the Eden-Hybinette procedure using a tricortical iliac crest bone graft. Using the previous incision, adequate exposure was done. The displaced screw was removed. Broken part of the other screw could not be removed. Thorough wash was given, and edges of the glenoid were freshened. Iliac crest bone graft of size 3 × 3 × 1.5 cm was harvested and fixed with the freshened glenoid bone with three cannulated screws (Fig. 4).
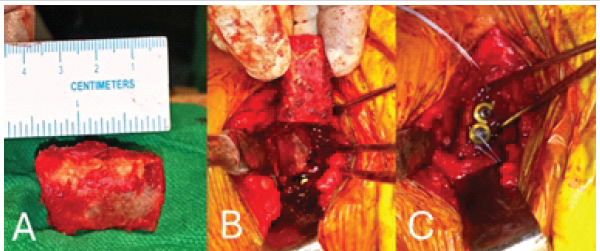
Figure 4: Intraoperative images, (a) Tricortical iliac crest graft harvested, (b) Placing the graft over freshened glenoid bone, (c) Fixation with screws.
Stability and range of motion were assessed intra-operatively. Thorough wash was given, and the incision was closed in layers. The patient received post-operative antibiotics and analgesics. Physiotherapy was started on post-operative day one as per the pain tolerance, and a plain radiograph was obtained (Fig. 5).
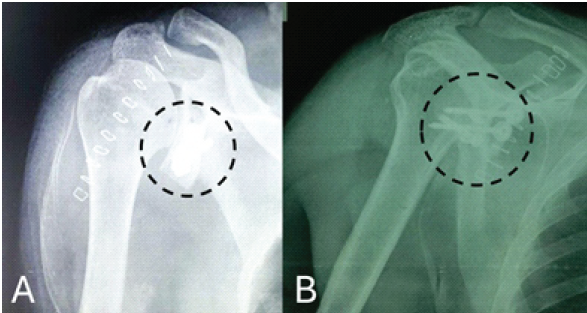
Figure 5: Immediate post-surgery plain radiograph, (a) Humerus in anteroposterior view, (b). Humerus in lateral view, both images showing reconstructed glenoid with screws. (marked with a dotted black circle).
Muscle strengthening was gradually started. The recovery was uneventful, and no significant donor site morbidity was encountered. Rehabilitation was continued, and the patient was followed up at regular intervals. Patient regained the complete range of motion at about 3 months postoperatively. CT scan was done at 6 months postoperatively, which was suggestive of signs of union (Fig. 6). The patient is currently able to do his activities of daily living without any apprehension (Fig. 7).

Figure 6: Computed tomography scan at 6 months follow-up showing signs of union. (marked with black arrow).
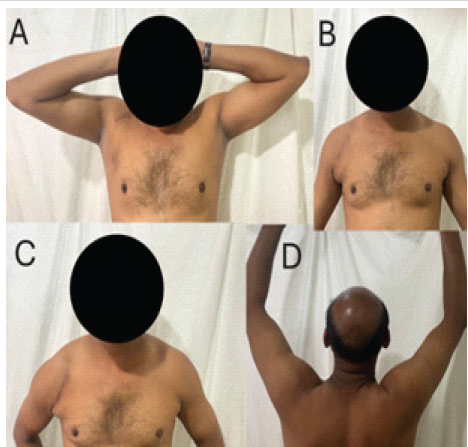
Figure 7: (a-d) Range of motion at 6-month follow-up showing near complete range of motion.
The Latarjet procedure is widely accepted for managing anterior shoulder instability in the presence of significant glenoid bone loss. [6-8] However, failure rates as high as 14% have been reported, particularly within the 1st post-operative year. Factors contributing to failure include technical errors (malpositioned bone block or hardware), graft non-union or resorption, unrecognized concurrent pathology, or patient-specific variables such as joint laxity or inadequate rehabilitation. [7] In this case, failure occurred within a year of the initial procedure, with imaging revealing hardware complications and significant glenoid bone resorption, necessitating revision surgery. [9] The Eden-Hybinette procedure offers a viable salvage option, particularly when the coracoid graft from the original Latarjet is non-viable or absent. [10] It directly addresses glenoid bone loss using a tricortical iliac crest autograft, which restores the bony architecture necessary for joint stability. Despite potential drawbacks including donor site morbidity, graft resorption, and fixation challenges-favorable outcomes have been documented when performed with meticulous technique. [11] In this case, the Eden-Hybinette technique successfully restored shoulder stability and function. The use of three cannulated screws provided rigid fixation, and early physiotherapy likely contributed to favorable functional outcomes. At 6 months, imaging confirmed graft union, and the patient resumed daily activities without apprehension. This case underscores the importance of individualized management and highlights Eden-Hybinette as an effective revision strategy following failed Latarjet.
Failed Latarjet procedures require careful evaluation to determine the underlying cause and appropriate revision strategy. The Eden-Hybinette procedure offers a reliable option for restoring shoulder stability, particularly in cases with significant glenoid bone loss or compromised coracoid grafts. When performed with proper technique and followed by structured rehabilitation, it can lead to favorable outcomes. Individualized surgical planning and close post-operative monitoring remain essential for successful recovery and long-term joint function.
Failed Latarjet procedures require thorough evaluation of the cause of failure and individualized surgical planning. The Eden-Hybinette technique, when performed meticulously with stable fixation and structured rehabilitation, can reliably restore stability and function with favorable outcomes.
References
- 1. Provencher MT, Bhatia S, Ghodadra NS, Grumet RC, Bach BR Jr., Dewing CB, et al. Recurrent shoulder instability: Current concepts for evaluation and management of glenoid bone loss. J Bone Joint Surg Am 2010;92:133-51. [Google Scholar] [PubMed]
- 2. Buda M, D’Ambrosi R, Bellato E, Blonna D, Cappellari A, Delle Rose G, et al. Failed latarjet procedure: A systematic review of surgery revision options. J Orthop Traumatol 2021;22:24. [Google Scholar] [PubMed]
- 3. Butt U, Charalambos CP. Complications associated with open coracoid transfer procedures for shoulder instability. J Shoulder Elbow Surg 2012;21:1110-9. [Google Scholar] [PubMed]
- 4. Hurley E, Bloom D, Manjunath A, Jazrawi L, Strauss E. Outcomes of revision surgery for a failed prior Latarjet procedure: A systematic review. Bull Hosp Jt Dis (2013) 2020;71:210-6. [Google Scholar] [PubMed]
- 5. Villatte G, Spurr S, Broden C, Martins A, Emery R, Reilly P. The eden-hybbinette procedure is one hundred years old! A historical view of the concept and its evolutions. Int Orthop 2018;42:2491-5. [Google Scholar] [PubMed]
- 6. Bedeir YH, Schumaier AP, Grawe BM. The failed latarjet procedure: Evaluation, treatment, and outcomes. JBJS Rev 2018;6:e10. [Google Scholar] [PubMed]
- 7. Provencher MT, Peebles LA, Aman ZS, Bernhardson AS, Murphy CP, Sanchez A, et al. Management of the failed Latarjet procedure: Outcomes of revision surgery with fresh distal tibial allograft. Am J Sports Med 2019;47:2795-802. [Google Scholar] [PubMed]
- 8. Gilat R, Lavoie-Gagne O, Haunschild ED, Knapik DM, Parvaresh KC, Fu MC, et al. Outcomes of the latarjet procedure with minimum 5- and 10-year follow-up: A systematic review. Shoulder Elbow 2020;12:315-29. [Google Scholar] [PubMed]
- 9. Weng PW, Shen HC, Lee HH, Wu SS, Lee CH. Open reconstruction of large bony glenoid erosion with allogeneic bone graft for recurrent anterior shoulder dislocation. Am J Sports Med 2009;37:1792-7. [Google Scholar] [PubMed]
- 10. Rabinowitz J, Friedman R, Eichinger JK. Management of glenoid bone loss with anterior shoulder instability: Indications and outcomes. Curr Rev Musculoskelet Med 2017;10:452-62. [Google Scholar] [PubMed]
- 11. Yamamoto N, Muraki T, An KN, Sperling JW, Cofield RH, Itoi E, et al. The stabilizing mechanism of the latarjet procedure: A cadaveric study. J Bone Joint Surg Am 2013;95:1390-7. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Single-Screw versus Two-Screw Fixation in the Latarjet Procedure: A Prospective Comparative Study
July 1, 2026 Single-Screw versus Two-Screw Fixation in the Latarjet Procedure: A Prospective Comparative Study December 1, 2025 Mid-term Functional Outcomes of Open Congruent Arc Latarjet for Recurrent Anterior Shoulder Instability: A Retrospective Cohort Study
December 1, 2025 Mid-term Functional Outcomes of Open Congruent Arc Latarjet for Recurrent Anterior Shoulder Instability: A Retrospective Cohort Study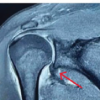 July 1, 2026 Humeral Avulsion of Glenohumeral Ligament Lesion – A Case Report and Surgical Considerations
July 1, 2026 Humeral Avulsion of Glenohumeral Ligament Lesion – A Case Report and Surgical Considerations July 1, 2025 Late Presentation of Acromioclavicular Joint Dislocation with Double Fracture of Coracoid Process Managed by Arthroscopic Stabilization Technique: A Case Report
July 1, 2025 Late Presentation of Acromioclavicular Joint Dislocation with Double Fracture of Coracoid Process Managed by Arthroscopic Stabilization Technique: A Case Report