
Early CT evaluation is essential for detecting subtle posteromedial process (Cedell’s) fractures of the talus that may appear normal on plain radiographs. Prompt surgical fixation through a posteromedial approach can restore joint stability and achieve excellent functional outcomes.
Dr. Jaideep Das, Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: jaideepdas01@gmail.com
Abstract
Introduction: Cedell’s fracture is an uncommon avulsion of the posteromedial process of the talus that may appear normal on radiographs. Early identification and anatomical fixation are essential to prevent long-term dysfunction.
Case Report: A 35-year-old male resident doctor sustained a twisting ankle injury after a fall from stairs. Radiographs were inconclusive, but computed tomography (CT) revealed a displaced posteromedial process (Cedell’s) fracture of the talus. The patient underwent open reduction and internal fixation through a posteromedial approach using two 3.0 mm Herbert screws. Postoperatively, the limb was immobilized in a below-knee slab for 2 weeks, followed by a below-knee cast for an additional 4 weeks. The cast was removed at 6 weeks. Gradual mobilization and partial weight-bearing were initiated, progressing to full weight-bearing by 8 weeks. Results: At 1 year, radiographs confirmed fracture union with full, pain-free ankle and subtalar motion and return to normal activity.
Conclusion: Cedell’s fracture should be suspected in patients with posteromedial ankle pain after trauma, even with normal radiographs. CT imaging is crucial for diagnosis, and early fixation through a posteromedial approach with Herbert screws provides stable fixation and excellent functional recovery.
Keywords: Cedell’s fracture, talus, posteromedial process, Herbert screw, posteromedial approach.
Fractures of the talus are rare, comprising approximately 0.1–0.85 % of all fractures and 3–5% of foot fractures [1,2]. Cedell’s fracture, first described in 1974 by Cedell as an avulsion of the posteromedial tubercle of the talus caused by dorsiflexion–pronation injury, is even rarer—representing <0.1% of all ankle and foot fractures and under 1% of talar fractures [3,4]. Because the fragment is small and may not be visible on plain radiographs, the diagnosis is often missed, leading to delayed treatment and poor outcomes [5]. This report describes a case of Cedell’s fracture diagnosed by computed tomography (CT) and successfully treated by open reduction and Herbert screw fixation through a posteromedial approach, achieving excellent functional recovery.
A 35-year-old male resident doctor presented with pain and swelling over the left ankle after slipping and falling on stairs. Examination revealed localized tenderness over the posteromedial aspect of the ankle with restricted movement. Plain radiographs (Fig. 1) appeared normal; however, due to high suspicion, a CT scan (Fig. 2) was performed, revealing a displaced fracture of the posteromedial process of the talus.

Figure 1: Pre-operative ankle radiographs (Anteroposterior and lateral) white arrow pointing to missed fracture.
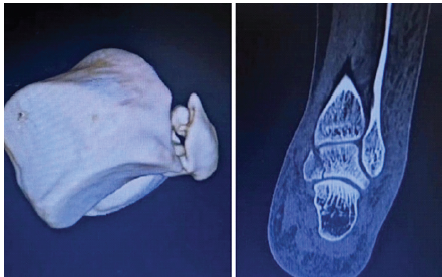
Figure 2: Pre-operative computed tomography showing displaced posteromedial process fracture (Cedell’s fracture).
The patient underwent surgery 1 day post-injury under spinal anesthesia in the prone position. A straight posteromedial incision was made just medial to the Achilles tendon (Fig. 3). 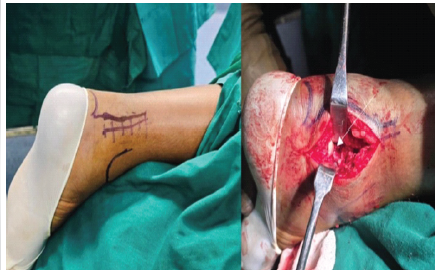
Figure 3: Intraoperative image showing posteromedial approach and white arrow showing fractured posteromedial talar process.The approach developed the interval between the flexor hallucis longus tendon laterally and the posterior tibial neurovascular bundle medially. The fracture fragment was exposed, anatomically reduced and temporarily fixed with a 1.5 mm K-wire. Under fluoroscopic guidance, two 3.0 mm Herbert screws were placed for definitive fixation (Fig. 4).
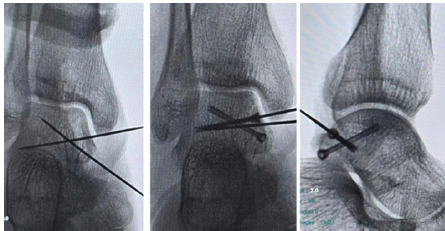
Figure 4: C-arm images showing placement of guide wires and Herbert screws.
Reduction and fixation were confirmed clinically and fluoroscopically, followed by thorough irrigation and layered wound closure was performed and a sterile dressing was applied. Postoperatively, the limb was immobilized in a below-knee slab for 2 weeks, followed by a below-knee cast for an additional 4 weeks. The cast was removed at 6 weeks. Subsequently, ankle and subtalar range-of-motion exercises were initiated, along with toe-touch weight bearing, gradually progressing to full weight bearing by 8 weeks. At 1 year, follow-up radiographs confirmed satisfactory implant position with good progression toward complete bony union (Fig. 5). Clinically, the patient was asymptomatic and demonstrated full, pain-free ankle range of motion at 1 year review (Fig. 6).
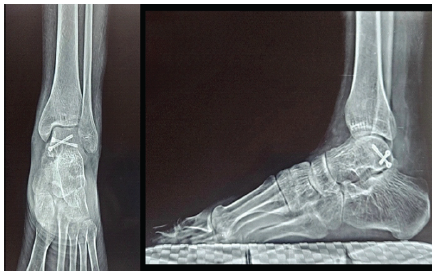
Figure 5: Anteroposterior and lateral ankle radiographs at 1-year follow-up showing complete radiological union with maintained alignment.

Figure 6: Clinical photographs at 1-year follow-up showing satisfactory foot alignment, primary intention healing of the operative scar, and near-normal ankle range of motion.
Cedell’s fracture is a rare injury caused by a dorsiflexion–pronation mechanism that avulses the posteromedial tubercle of the talus [3]. Because the fragment is small and lies deep to the medial malleolus, these fractures are frequently missed on plain radiographs. Watanabe et al. highlighted that most missed posteromedial talar fractures occurred due to reliance on normal-appearing radiographs despite persistent posteromedial ankle pain [5]. Similarly, Sallent et al. reported that delayed diagnosis often results in chronic pain, non-union, and subtalar arthritis, underscoring the need for early CT imaging in clinically suspicious cases [7]. In the present case, CT scanning played a pivotal role in establishing an early diagnosis, consistent with multiple studies advocating CT as the gold standard for detecting subtle or occult talar process fractures [5,6,7]. Early identification is crucial, as non-displaced fragments may heal with immobilization, but displaced fractures generally require operative fixation to restore subtalar joint congruity and prevent long-term dysfunction [7,8]. Our management aligned closely with existing literature supporting surgical fixation of displaced Cedell’s fractures. Li et al. reported that open reduction and internal fixation offered superior functional outcomes compared to conservative management in displaced talar process injuries, particularly in terms of restoring subtalar motion and reducing chronic pain [8]. Similar to their findings, our patient demonstrated full, pain-free range of motion by 1 year. The posteromedial surgical approach used in this case is widely endorsed for its direct access to the posteromedial talar process with minimal risk to the neurovascular bundle. Ebraheim et al. detailed the anatomical safety of this approach, allowing adequate visualization and precise fracture reduction [1,9]. Our experience closely paralleled these findings, enabling anatomical reduction without complications. Herbert screws were chosen for fixation due to their headless, compression design, which is advantageous for small intra-articular fragments. Mallon WJ documented excellent outcomes using Herbert screws for small talar fractures, reporting stable fixation and early mobilization without hardware prominence issues [10]. Our patient achieved similarly favorable results, with radiographic union and full functional recovery by 1 year. Overall, the clinical course of this case is consistent with the best outcomes described in the literature. Early CT-based diagnosis, anatomical reduction, and stable compression fixation through a posteromedial approach resulted in reliable fracture union and complete return of function. This case reinforces the importance of maintaining a high index of suspicion for Cedell’s fractures in patients with posteromedial ankle pain following trauma and supports early operative management of displaced fragments to prevent long-term morbidity [6,7,8].
Cedell’s fractures of the talus are rare and easily missed on initial imaging. CT scanning is crucial for diagnosis. Early surgical fixation using a posteromedial approach and Herbert screws can result in complete recovery with restoration of ankle function.
Subtle posteromedial process fractures of the talus may appear normal on radiographs. Early CT evaluation and anatomical fixation through the posteromedial approach can ensure full functional recovery.
References
- 1. Ebraheim NA, Padanilam TG, Wong FY. Posteromedial process fractures of the talus Foot Ankle Int 1995;16:764-9. [Google Scholar] [PubMed]
- 2. Zwiers R, de Leeuw PAJ, Wiegerinck EMA, van Dijk CN. Surgical treatment for posteromedial talar process fractures. Foot Ankle Surg. 2020;26(8):911–917. https://doi.org/10.1016/j.fas.2019.12.003. [Google Scholar] [PubMed] [CrossRef]
- 3. Cedell CA. Rupture of the posterior talotibial ligament with the avulsion of a bone fragment from the talus. Acta Orthop 1974;45:454-61. [Google Scholar] [PubMed]
- 4. Canale ST, Kelly FB Jr. Fractures of the neck of the talus. Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-56. [Google Scholar] [PubMed]
- 5. Moger NM, Pragadeeshwaran J, Verma A, K V A, Aditya KS, Meena PK. Outcome of Neglected Talus Neck Fracture and it’s Management: A Case Report. J Orthop Case Rep. 2021 Apr;11(4):41-44. doi: 10.13107/jocr.2021.v11.i04.2144. PMID: 34327163; PMCID: PMC8310639. [Google Scholar] [PubMed] [CrossRef]
- 6. Swords, M., Shank, J. & Benirschke, S. Surgical Treatment of Posteromedial Talus Fractures: Technique Description and Results of 10 Cases. IJOO 52, 269–275 (2018). https://doi.org/10.4103/ortho.IJOrtho_646_17 [Google Scholar] [PubMed] [CrossRef]
- 7. Sallent A, Núñez Pereira S, Maled I, Duarri G, Busquets R. Fractures of the posteromedial process of the talus (Cedell’s fracture): 3 cases and review of the literature. Foot Ankle Surg Tech Rep Cases. 2022;2:100127. doi:10.1016/j.fastrc.2021.100127. [Google Scholar] [PubMed] [CrossRef]
- 8. Li T, Zhang Q, Li J, et al. Open reduction for talar process fractures: outcomes and pitfalls. J Orthop Trauma. 2020;34(3):e91-e96. [Google Scholar] [PubMed]
- 9. Ebraheim NA, Padanilam TG, Wong FY. Anatomic considerations for posteromedial surgical exposure of the talus. Foot Ankle Int. 1996;17(12):719-725. [Google Scholar] [PubMed]
- 10. Mallon WJ, Wombwell JH, Nunley JA. Intra-Articular Talar Fractures: Repair Using the Herbert Bone Screw. Foot & Ankle. 1989;10(2):88-92. doi:10.1177/107110078901000207 [Google Scholar] [PubMed] [CrossRef]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Aneurysmal Bone Cyst of Talus: Case Report of a Rare Presentation
January 1, 2026 Aneurysmal Bone Cyst of Talus: Case Report of a Rare Presentation November 1, 2025 Assessment of Functional Outcome of Arthroscopic Microfractures for Osteochondral Defect of Talus
November 1, 2025 Assessment of Functional Outcome of Arthroscopic Microfractures for Osteochondral Defect of Talus November 1, 2025 Outcome of Non-thumb Metacarpal Shaft Fractures Treated by Two Different Techniques – K Wire and Herbert Screw Fixation: A Comparative Single Centre Study
November 1, 2025 Outcome of Non-thumb Metacarpal Shaft Fractures Treated by Two Different Techniques – K Wire and Herbert Screw Fixation: A Comparative Single Centre Study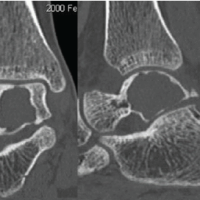 September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report
September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report