
Long-standing humeral shaft non-union can lead to rare, delayed non-traumatic intramedullary nail breakage, and single-stage nail removal with compression plating and autogenous bone grafting reliably restores union by addressing both mechanical and biological deficiencies.
Dr. Akilan Soundararajan Narayanan, College-Vinayaka Mission’s Kirupananda Variyar Medical College and Hospital, University-Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: drakilns95@gmail.com
Abstract
Introduction: Non-union following humeral shaft fractures is an uncommon yet disabling complication that may ultimately lead to implant failure in the presence of persistent mechanical instability. Delayed, non-traumatic breakage of an intramedullary nail several decades after fixation is exceedingly rare.
Case Report: We report the case of a 44-year-old male who presented 20 years after primary intramedullary interlocking nailing for a humeral shaft fracture with progressive arm pain, functional limitation, established mid-diaphyseal non-union, and spontaneous nail breakage in the absence of new trauma. The patient was managed with a single-stage surgical procedure comprising implant removal, thorough debridement of the non-union site, open reduction and internal fixation using compression plating, and augmentation with autogenous iliac crest bone graft. The post-operative course was uneventful, and serial radiographs demonstrated progressive healing with solid union and restoration of function.
Conclusion: This case highlights the importance of addressing both mechanical stability and the biological environment in the management of chronic humeral shaft non-union and supports single-stage nail removal followed by compression plating with autologous bone grafting as a reliable treatment strategy for rare late implant failures.
Keywords: Humeral shaft fracture, non-union, intramedullary nail failure, nail breakage, compression plating, iliac crest bone graft.
Humeral shaft fractures account for approximately 3–5% of all fractures and nearly 30% of fractures involving the humerus. Although there is general agreement regarding the indications for operative management, the choice of fixation device – plate versus intramedullary nail – remains a subject of debate [1,2,3]. The reported incidence of non-union following operative treatment ranges between 3% and 5%; however, this rate is significantly higher after non-operative management, reaching up to 23% according to the literature. The risk of non-union is increased in the presence of open fractures, high-energy trauma, bone loss or fracture gap, soft-tissue interposition, unstable or segmental fracture patterns, compromised blood supply, infection, and initial treatment with traction or a hanging cast. Patient-related factors such as obesity, osteoporosis, alcohol abuse, malnutrition, and poor compliance further contribute to the development of non-union [4,5,6,7]. Humeral shaft non-union following previous intramedullary nailing poses a significant reconstructive challenge due to implant loosening, surrounding bone loss, and altered biology at the non-union site, which may complicate revision surgery and adversely affect outcomes. Various surgical strategies have been described to address these complex scenarios, including implant removal with compression plating, exchange intramedullary nailing, Ilizarov external fixation, and the use of wave plates [8,9,10]. We report a rare case of a 44-year-old male presenting 20 years after primary intramedullary interlocking (IMIL) nailing for a humeral shaft fracture, complicated by established mid-diaphyseal non-union and delayed implant failure. The patient was successfully managed with single-stage nail removal, open reduction, and internal fixation using compression plating and autogenous iliac crest bone grafting, highlighting an effective treatment strategy for long-standing humeral shaft non-union with late nail breakage.
A 44-year-old male patient presented to our hospital with complaints of moderate pain and functional limitation of the operated upper limb for 4 months. He had a significant history of a right humeral shaft fracture sustained in February 2005 following a road traffic accident. At that time, he underwent surgical fixation at his hometown hospital, reportedly by closed reduction and internal fixation using an IMIL nail for the humerus on February 08, 2005. The post-operative period was uneventful, and he remained asymptomatic for many years (Fig. 1).
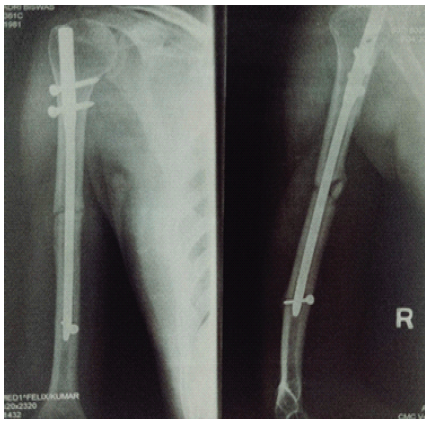
Figure 1: Post-operative anteroposterior and lateral radiographs showing intramedullary interlocking nailing of the right humerus performed in February 2005.
In April 2024, the patient developed vague, chronic pain at the fracture site and was evaluated by a nearby orthopedic surgeon. Anteroposterior and lateral radiographs of the right humerus demonstrated a mid-diaphyseal non-union with a persistent fracture line, sclerotic fracture margins, and an IMIL nail in situ. Surgical intervention was advised; however, the patient did not comply with follow-up as recommended (Fig. 2).
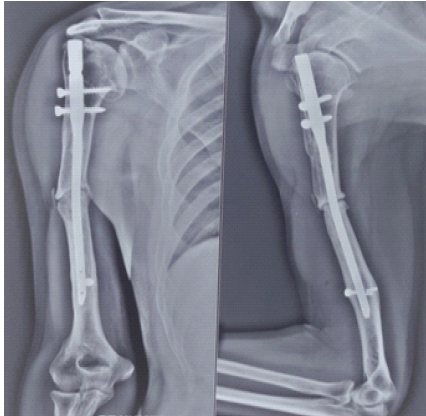
Figure 2: Anteroposterior and lateral radiographs of the right humerus taken in April 2024 demonstrating mid-diaphyseal non-union with a persistent fracture line, sclerotic bone ends, and an intramedullary interlocking nail in situ.
In May 2025, he developed insidious-onset pain and progressive difficulty in using the affected limb without any preceding history of trauma or fall. He also reported having undergone pacemaker implantation 3 months before presentation for a cardiac indication. On clinical examination, there was localized tenderness over the right mid-arm region with restriction of shoulder and elbow movements secondary to pain, raising suspicion of implant failure and non-union, which was subsequently confirmed on imaging studies.
Radiological evaluation revealed a non-union of the right mid-diaphyseal humerus associated with non-traumatic breakage of the IMIL nail. All routine pre-operative investigations were within normal limits (Fig. 3).
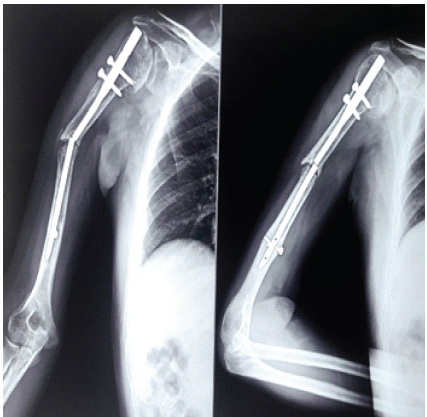
Figure 3: Current (May 2025) anteroposterior and lateral radiographs of the right humerus showing established mid-diaphyseal non-union with implant failure due to breakage of the intramedullary interlocking nail.
A single-stage surgical strategy was planned with the objective of achieving stable fixation and biological augmentation of the non-union. The procedure included removal of the failed IMIL nail along with the associated locking screws, followed by open reduction of the fracture site and internal fixation using plate osteosynthesis. Thorough debridement of fibrous tissue at the non-union site and freshening of the sclerotic fracture ends were performed to enhance the biological healing potential. Autologous cancellous bone graft harvested from the ipsilateral iliac crest was packed circumferentially around the fracture site to promote osteogenesis and facilitate union (Fig. 4).
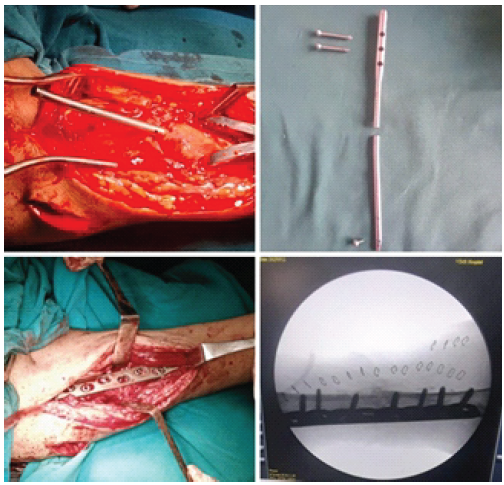
Figure 4: Intra-operative clinical photographs and C-arm images demonstrating implant removal, fracture site preparation, compression plating, and bone grafting.
The post-operative course was uneventful. Early shoulder and elbow mobilization was initiated following wound healing. Immediate post-operative radiographs demonstrated stabilization of the right mid-shaft non-union with plate osteosynthesis, adequately bridging the previous fracture site and maintaining satisfactory alignment and length of the humerus (Fig. 5).
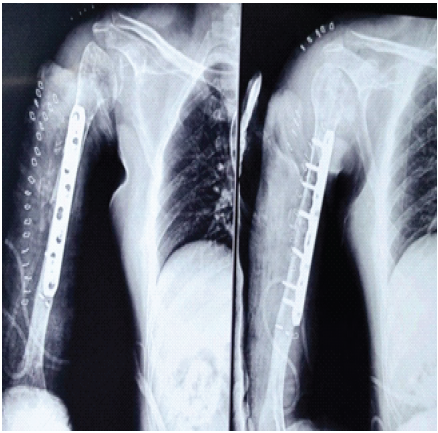
Figure 5: Immediate post-operative anteroposterior and lateral radiographs showing stabilization of the right mid-shaft nonunion with plate osteosynthesis, bridging the previous fracture site and maintaining satisfactory alignment and humeral length.
At the 6th post-operative month follow-up, the patient reported complete resolution of pain and significant functional improvement, achieving a near-full range of motion and return to daily activities. Radiographs of the right humerus at the 6th post-operative month showed satisfactory fracture union with bony callus formation at the fracture site, with no evidence of implant breakage or loosening (Fig. 6).
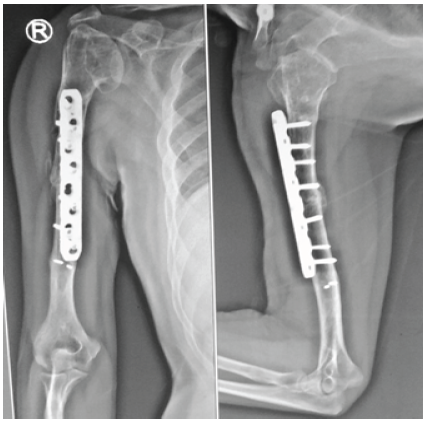
Figure 6: Anteroposterior and lateral radiographs of the right humerus at the 6th post-operative month demonstrating satisfactory fracture union with bony callus formation and no evidence of implant loosening or breakage.
Humeral shaft non-union is an uncommon but disabling complication, with reported rates ranging from 0% to 13% following operative fixation and up to 23% after conservative treatment [11,12]. Persistent mechanical instability – particularly rotational stress and fracture gap distraction – is a major contributor to failure of union following intramedullary nailing [4]. Delayed, non-traumatic breakage of a humeral intramedullary nail is exceedingly rare. Ziveri and De Biase reported a similar case occurring 11 years after index surgery and emphasized prolonged cyclic loading across an ununited fracture as the principal mechanism leading to implant fatigue failure [4]. In longstanding non-unions, continuous rotational and bending stresses transmitted through the implant can ultimately result in fatigue fracture, even in the absence of new trauma. Compression plating combined with autogenous iliac crest bone grafting has consistently been recommended as the gold standard treatment for established humeral shaft non-union [11,13]. Feng et al. demonstrated successful union in all patients with long-standing humeral non-union treated using locking compression plates and iliac crest bone graft, with marked improvement in shoulder and elbow function [13]. Comparable results have also been reported in recalcitrant cases managed with double-plate fixation and biological augmentation, particularly in the presence of poor bone quality or extensive non-union [11]. The principles of restoring mechanical stability while enhancing biological healing correspond to the “diamond concept” of fracture union, which emphasizes fixation rigidity, osteogenic cells, osteoconductive scaffold, and growth factors [12]. While minimally invasive plate osteosynthesis without bone grafting has been described for biologically active non-unions where instability is the predominant factor, chronic non-unions with sclerotic fracture margins favor formal debridement and graft augmentation to achieve reliable union [13]. Exchange nailing alone has demonstrated inferior outcomes compared with nail removal and compression plating with bone grafting, unless supplemented with extensive decortication and biological augmentation [4].
Non-traumatic intramedullary nail breakage secondary to long-standing humeral shaft non-union is an exceptionally rare event and may present several decades after the index procedure. Persistent rotational stresses across an ununited fracture appear to be the principal mechanism leading to implant fatigue failure. A single-stage approach involving nail removal, meticulous debridement, rigid compression plate fixation, and autogenous iliac crest bone grafting can achieve reliable fracture union and excellent functional recovery. Surgeons should maintain long-term vigilance in patients with suspected humeral non-union and consider definitive revision surgery at an early stage to prevent catastrophic implant failure.
Delayed, non-traumatic intramedullary nail breakage can occur decades after fixation in the presence of an untreated humeral shaft non-union due to prolonged cyclic mechanical stress. Early recognition of persistent non-union and timely definitive revision surgery are essential to prevent catastrophic implant failure. Single-stage nail removal with compression plating and autogenous bone grafting provides reliable union by addressing both mechanical stability and biological deficiency in chronic humeral shaft non-union.
References
- 1. Court-Brown CM, Caesar B. Epidemiology of adult fractures: A review. Injury 2006;37:691-7. [Google Scholar] [PubMed]
- 2. Ekholm R, Adami J, Tidermark J, Hansson K, Törnkvist H, Ponzer S. Fractures of the shaft of the humerus. An epidemiological study of 401 fractures. J Bone Joint Surg Br 2006;88:1469-73. [Google Scholar] [PubMed]
- 3. Sarmiento A, Zagorski JB, Zych GA, Latta LL, Capps CA. Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am 2000;82:478-86. [Google Scholar] [PubMed]
- 4. Ziveri G, De Biase CF. A case report of humeral nail breakage after 11 years secondary to shaft nonunion: Treatment with autogenous iliac crest bone graft and compression plate. J Orthop Case Rep 2020;10:89-92. [Google Scholar] [PubMed]
- 5. Lin J, Hou SM, Hang YS, Chao EK. Treatment of humeral shaft nonunions after failure of locking intramedullary nails. J Trauma 2003;54:784-9. [Google Scholar] [PubMed]
- 6. McKee MD, Miranda MA, Riemer BL, Blasier RB, Redmond BJ, Sims SH, et al. Management of humeral nonunion after the failure of locking intramedullary nails. J Orthop Trauma 1996;10:492-9. [Google Scholar] [PubMed]
- 7. Finkkilä T, Ristiniemi J, Hyvönen P, Lakovaara M, Hämäläinen M. Nonunion after intramedullary nailing of humeral shaft fractures. J Orthop Trauma 2004;18:617-23. [Google Scholar] [PubMed]
- 8. Ring D, Perey BH, Jupiter JB. The functional outcome of operative treatment of ununited fractures of the humeral diaphysis in older patients. J Bone Joint Surg Am 1999;81:177-90. [Google Scholar] [PubMed]
- 9. Giannoudis PV, Einhorn TA, Marsh D. Fracture healing: The diamond concept. Injury 2007;38 Suppl 4:S3-6. [Google Scholar] [PubMed]
- 10. Brinker MR, O’Connor DP. The incidence of fractures and dislocations referred for orthopaedic services in a capitated population. J Bone Joint Surg Am 2004;86:290-7. [Google Scholar] [PubMed]
- 11. Feng D, Wang X, Sun L, Cai X, Zhang K, Wang Z, et al. Double plating with autogenous bone grafting as a salvage procedure for recalcitrant humeral shaft nonunion. BMC Musculoskelet Disord 2020;21:769. [Google Scholar] [PubMed]
- 12. Feng D, Zhang J, Zhu Y, Wu S, Shan J, Ye A, et al. Plate fixation with autogenous bone grafting for longstanding humeral shaft nonunion: A retrospective study of 6 cases. Medicine (Baltimore) 2018;97:e11974. [Google Scholar] [PubMed]
- 13. Suda Y, Oe K, Fukui T, Mifune Y, Inui A, Kawamoto T, et al. Minimally invasive plate osteosynthesis for humeral shaft nonunion: A report of two cases. Ann Med Surg (Lond) 2019;48:43-7. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report
July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction
June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction April 1, 2026 Modified Posterior Approach for Scapular Body Non-union: A Case Report
April 1, 2026 Modified Posterior Approach for Scapular Body Non-union: A Case Report April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report
April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report