
Diagnostic awareness of Morel-Lavallée lesions with arthroscopic management is an effective way to treat these rare soft-tissue injuries in a minimally invasive manner.
Mr. Stefan W. Fleps, Department of Orthopaedics and Physical Performance, University of Rochester, New York, United States. E-mail: Stefan_Fleps@urmc.rochester.edu
Abstract
Introduction: Morel-Lavallée lesions (MLLs) are uncommon soft-tissue injuries that can be easily mistaken for other conditions, especially around the knee.
Case Report: We present the case of an 18-year-old female athlete who developed a large collection of fluid around the knee after a direct blow to the leg during a wrestling competition. The injury first appeared to be a simple prepatellar bursitis but was later found to be a large fluid collection on magnetic resonance imaging, which measured 9.0 × 2.2 × 18.1 cm and extended from the distal quadriceps to below the tibial tubercle. The patient had a minimally invasive arthroscopic procedure to drain and clean the area. This procedure was followed by a course of prophylactic antibiotics.
Conclusion: This case highlights the importance of considering MLLs when evaluating knee swelling and shows that arthroscopic surgery can be an effective and less invasive treatment option for young active patients.
Keywords: Morel-Lavallée lesion, arthroscopy, sports medicine, injury.
French surgeon Maurice Morel-Lavallée first described the Morel-Lavallée lesion (MLL) in 1853 as a closed degloving injury caused by trauma [1]. Common causes of MLLs include high-energy, blunt, or crushing injuries that generate a shearing force which separates the subcutaneous tissue from the underlying fascia [2,3]. This separation creates a potential space that can fill with hemolymphatic fluid, necrotic fat, and debris [4]. MLLs most frequently occur at the greater trochanter, pelvis, thigh, and knee, and are typically associated with high-energy trauma such as motor vehicle accidents and sports injuries [5,6]. MLLs of the knee are less common and generally occur in athletes following a shearing force with the knee in active flexion [7]. The true prevalence of MLLs is difficult to estimate, as the diagnosis is often missed or misdiagnosed. Moriarty et al. identified sixty-six MLL cases over 10-years at a Level 1 trauma center [8]. A review article noted an approximate 2:1 male-to-female ratio in MLL incidence, possibly due to higher trauma rates in males [9]. No consensus currently exists regarding the precise prevalence of MLLs or its gender distribution. Clinically, MLLs present a diagnostic challenge. They are often misdiagnosed as hematomas, abscesses, or soft-tissue tumors, and may be overlooked when associated with more severe trauma such as fractures or polytrauma requiring immediate intervention [10]. When left untreated, MLLs can evolve into chronic encapsulated fluid collections or become infected, leading to tissue necrosis [11]. The clinical presentation can be acute or delayed, typically appearing as a painful, tender, and fluctuant collection at the site of trauma [12,13]. Discoloration of the overlying skin, hypermobility, and ecchymosis may also be present [14]. Diagnosis is best established through a thorough clinical assessment combined with external skin findings, and advanced imaging, such as magnetic resonance imaging (MRI), computed tomography (CT), or ultrasound (US). Here, we present a case of a young female athlete with a traumatic pre-patellar MLL diagnosed by MRI and treated with arthroscopic surgical debridement. This case highlights the radiographic features and surgical management of a rare MLL of the knee in a young female athlete.
An 18-year-old female athlete with no significant past medical history presented with left knee pain and subsequent swelling following a traumatic sports-related injury. While wrestling her opponent on the mat, she was able to lift her competitor off the ground and forcefully landed with her competitor in her arms. With her competitor in her arms, she forcefully attempted a take down, and at that time, the bodyweight of her competitor fell directly over her leg. She noticed near immediate effusion over her left leg and significant pain. Initial evaluation suggested extensive prepatellar bursitis without signs of infection. However, further workup revealed that the lesion extended well beyond the boundaries of the prepatellar bursa. On physical examination, there was a large, fluctuant fluid collection over the anterior aspect of the left leg, extending from the mid to distal quadriceps to a point distal to the tibial tubercle. A positive wave sign indicated significant fluctuance. The extensor mechanism was intact, and the knee was stable on ligamentous examination. Knee flexion was limited to 90° due to the mass effect of the fluid accumulation. There were no signs of systemic or local infection: no warmth, erythema, ecchymosis, lymphadenopathy, or radicular symptoms were noted. Radiographic imaging was obtained to evaluate the extent of the lesion and to rule out fracture, dislocation, ligamentous injury, and meniscal pathology.
MRI results
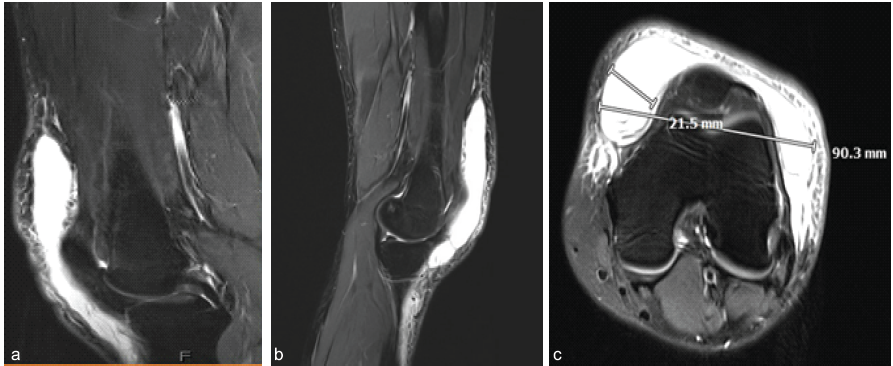
Figure 1: Magnetic resonance imaging of Morel-Lavallée lesion. (a and b) Sagittal T2-weighted magnetic resonance imaging (MRI). (c) Axial T2-weighted MRI. The large lesion is noted as a hyperintense collection originating from the distal quadriceps that continues distally past the tibial tubercle. The dimensions of the lesion are seen in the axial slices, with included dimensions in mm.
Fig. 1 displays a relevant pre-operative MRI of the left knee. T1- weighted sequences revealed a large, 9.0 × 2.2 × 18.1 cm, horseshoe-shaped fluid collection located in the subcutaneous and perifascial planes overlying the distal quadriceps muscle, quadriceps tendon, patella, and patellar tendon. Associated sub-cutaneous edema was also noted. T1-weighted MRI imaging revealed an at least 18.1 cm long distal pre-quadriceps, pre-patellar fascial collection on the left thigh. The fluid extended distally past the anterior knee, with the collection involving deep subcutaneous fascial planes (Fig. 2). No ligamentous, meniscal, or osseous abnormalities were identified. Based on the clinical presentation and MRI findings, a diagnosis of a MLL was made.
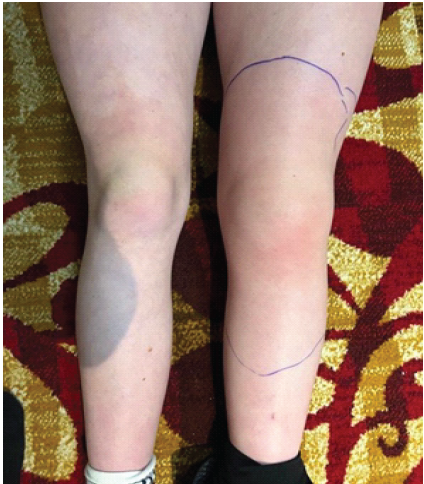
Figure 2: Bilateral lower extremities prior to surgical intervention. A large effusion of the left leg is seen and outlined in comparison to the right leg.
Surgical treatment
A minimally invasive arthroscopic approach was used to debride and irrigate the lesion. Standard anteromedial and anterolateral portal incisions were created, allowing access to the lesion with an arthroscopic shaver. However, the joint capsule was not entered, as the fluid collection was readily accessible from extra-articular space. Intraoperatively, the collection was found to extend from above the quadriceps tendon proximally and past the tibial tubercle. The cavity was drained, and the area was extensively irrigated. The volume and extent of the collection were significantly greater than what is typically seen in prepatellar bursitis. Intraoperative cultures were obtained, and prophylactic antibiotics were administered. In addition, a vancomycin infusion was delivered directly into the subcutaneous pocket to minimize the risk of infection. A compressive dressing was applied, extending from the foot to the mid-thigh. The patient tolerated the procedure well and was discharged on the same day with no additional precautions required (Fig. 3).

Figure 3: Bilateral lower extremities post-operatively. Significantly reduced effusion over the left extremity following arthroscopic debridement and irrigation. Wound dressings were placed over the incisions.
Management of MLLs depends on several factors, including lesion size, location, the presence of a pseudo capsule, and signs of infection. There is currently no standardized treatment protocol for MLLs, and management options range from conservative methods to surgical intervention [14]. Nonsurgical treatments, such as compressive dressings and percutaneous aspiration, may be effective in acute, small-volume lesions without evidence of capsule formation [15]. Surgical management is typically indicated for chronic, large, or symptomatic lesions, especially when a well-defined capsule is present. In the present case, a minimally invasive arthroscopic debridement and irrigation technique was employed. Although there were no signs or symptoms of infection, vancomycin was infused into the subcutaneous pocket as a prophylactic measure. The patient tolerated the procedure well, with an immediate notable reduction in swelling and no postoperative compilations. At the 11-day follow-up, the patient demonstrated no fluid accumulation, and the affected area was non-tender. The athlete was cleared to return to activity gradually, as tolerated. This case supports the use of arthroscopic techniques as a safe and effective treatment option for MLLs in young, active patients. The diagnosis of MLL is typically based on a combination of clinical history, mechanism of injury, physical examination, and imaging. Early and accurate diagnosis is critical, as untreated MLLs carry a high risk of infection that can lead to tissue necrosis [16]. Because MLLs, particularly around the knee, can mimic common pathologies such as prepatellar bursitis, imaging plays a crucial role in distinguishing them. MRI is the preferred imaging modality for diagnosing MLLs due to its ability to visualize the lesion’s extent, fluid characteristics, and capsule formation. US can also be a valuable tool, particularly for initial or bedside assessments. It provides rapid visualization of fluid collections and may aid in aspirations; however, it is highly operator dependent and less effective for evaluating chronic or deep lesions involving pseudocapsules. CT may be used in the acute trauma setting to assess bony injury, but it is limited in its ability to characterize soft-tissue injuries such as MLLs [3]. Overall, MRI remains the gold standard for imaging modality, particularly when integrated with a detailed history and physical exam to assess lesion size, chronicity, and complexity.
This case highlights a rare traumatic MLL initially thought to be prepatellar bursitis. Prompt recognition and treatment of MLLs is essential, as delayed management can increase the risk of injection, tissue necrosis, and prolonged functional impairment. On physical examination, the patient exhibited a large, fluctuant fluid collection with a positive wave sign and restricted range of motion. MRI demonstrated a large fluid-filled cavity extending well beyond the boundaries of the prepatellar bursa. The patient underwent successful arthroscopic debridement, with immediate reduction in lesion size. This case underscores the importance of considering and recognizing MLLs in the differential diagnosis of anterior knee swelling and offers a minimally invasive treatment approach for effective management.
MLLs can present in multiple ways and present a diagnostic challenge from a radiology perspective. They are formed via an interesting mechanism, and management of them is not heterogenous amongst physicians. Awareness of MLLs is important as they increased risk of a multitude of complications. Arthroscopy is a unique and minimally invasive strategy for treating these lesions.
References
- 1. Bonilla-Yoon I, Masih S, Patel DB, White EA, Levine BD, Chow K, et al. The morel-lavallee lesion: Pathophysiology, clinical presentation, imaging features, and treatment options. Emerg Radiol 2014;21:35-43. [Google Scholar] [PubMed]
- 2. Nair AV, Nazar P, Sekhar R, Ramachandran P, Moorthy S. Morel-Lavallee lesion: A closed degloving injury that requires real attention. Indian J Radiol Imaging 2014;24:288-90. [Google Scholar] [PubMed]
- 3. Diviti S, Gupta N, Hooda K, Sharma K, Lo L. Morel-lavallee lesions-review of pathophysiology, clinical findings, imaging findings and management. J Clin Diagn Res 2017;11:TE01-4. [Google Scholar] [PubMed]
- 4. Mellado JM, Bencardino JT. Morel-Lavallee lesion: Review with emphasis on MR imaging. Magn Reson Imaging Clin N Am 2005;13:775-82. [Google Scholar] [PubMed]
- 5. Vanhegan IS, Dala-Ali B, Verhelst L, Mallucci P, Haddad FS. The morel-lavallee lesion as a rare differential diagnosis for recalcitrant bursitis of the knee: Case report and literature review. Case Rep Orthop 2012;2012:593193. [Google Scholar] [PubMed]
- 6. Puig J, Pelaez I, Banos J, Balliu E, Casas M, Maroto A, et al. Long-standing Morel-Lavallee lesion in the proximal thigh: Ultrasound and MR findings with surgical and histopathological correlation. Australas Radiol 2006;50:594-7. [Google Scholar] [PubMed]
- 7. Tejwani SG, Cohen SB, Bradley JP. Management of morel-lavallee lesion of the knee: Twenty-seven cases in the national football league. Am J Sports Med 2007;35:1162-7. [Google Scholar] [PubMed]
- 8. Moriarty HK, Ban EJ, Schlegel RN, Goh GS, Matthew JK, Clements W. Ten-year incidence and treatment outcomes of closed degloving injuries (morel-lavallee lesions) in a level 1 trauma centre. J Med Imaging Radiat Oncol 2023;67:260-6. [Google Scholar] [PubMed]
- 9. Shen C, Peng JP, Chen XD. Efficacy of treatment in peri-pelvic morel-lavallee lesion: A systematic review of the literature. Arch Orthop Trauma Surg 2013;133:635-40. [Google Scholar] [PubMed]
- 10. Singh R, Rymer B, Youssef B, Lim J. The morel-lavallee lesion and its management: A review of the literature. J Orthop 2018;15:917-21. [Google Scholar] [PubMed]
- 11. Khan KK, Dhaniwala NS, Gupta S, Kekatpure AL. The importance of prompt management of morel-lavallee lesions. Cureus 2022;14:e24639. [Google Scholar] [PubMed]
- 12. Stiff KM, Vargas C, Bates M, Somach SC. Chronic morel-lavallee lesion: Presentation as a pseudotumor. JAAD Case Rep 2022;27:75-8. [Google Scholar] [PubMed]
- 13. Yang Y, Tang TT. The morel-lavallee lesion: Review and update on diagnosis and management. Orthop Surg 2023;15:2485-91. [Google Scholar] [PubMed]
- 14. Scolaro JA, Chao T, Zamorano DP. The morel-lavallee lesion: Diagnosis and management. J Am Acad Orthop Surg 2016;24:667-72. [Google Scholar] [PubMed]
- 15. McKenzie GA, Niederhauser BD, Collins MS, Howe BM. CT characteristics of Morel-Lavallee lesions: An under-recognized but significant finding in acute trauma imaging. Skeletal Radiol 2016;45:1053-60. [Google Scholar] [PubMed]
- 16. Hak DJ, Olson SA, Matta JM. Diagnosis and management of closed internal degloving injuries associated with pelvic and acetabular fractures: The Morel-Lavallee lesion. J Trauma 1997;42:1046-51. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2024 Flag Sign: A Case Report of an Unusual Magnetic Resonance Imaging Finding of a Medial Meniscal Root Fragment in an Adolescent Water Polo Player
November 1, 2024 Flag Sign: A Case Report of an Unusual Magnetic Resonance Imaging Finding of a Medial Meniscal Root Fragment in an Adolescent Water Polo Player November 1, 2024 Paralabral Cysts with Associated Infraspinatus and Teres Minor Denervation: A Case Report
November 1, 2024 Paralabral Cysts with Associated Infraspinatus and Teres Minor Denervation: A Case Report July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates
July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study